Nursing care for Pulmonary Embolism In Critically Ill

Nursing care for: Pulmonary Embolism In Critically Ill Patients ��. �����������

Pathophysiology ของ acute pulmonary embolism ตอ ระบบไหลเวยน โลหต

PULMONARY EMBOLISM RISK FACTORS Inherited conditions Acquired conditions • Factor V Leiden mutation • Prothrombin gene mutation • Deficiency of antithrombin III • Deficiency of protein C or protein S

• • • • Hyperhomocysteinemia Oral contraceptive pills Hormone replacement therapy Atherosclerotic disease Personal or family history of VTE Recent trauma, fracture, surgery, or hospitalization Immobilization Pregnancy Long-haul air travel Pacemaker or implantable cardiac defibrillator leads and indwelling venous catheters

How is pulmonary embolism diagnosed? • Chest X-ray plate-like atelectasis, pleural effusion • Ventilation-perfusion scan (V/Q scan) • Pulmonary angiogram • Spiral computed tomography (also called CT or CAT scan). วธการวนจฉยแบบรวดเรว สามารถชวยในการวนจฉยในผปวยทม major thrombusขนาดใหญใน pulmonary artery แตถากอนเลอดมขนาดเลกมกมองไมเหน
. • Duplex ultrasound (US) • Laboratory tests. check")
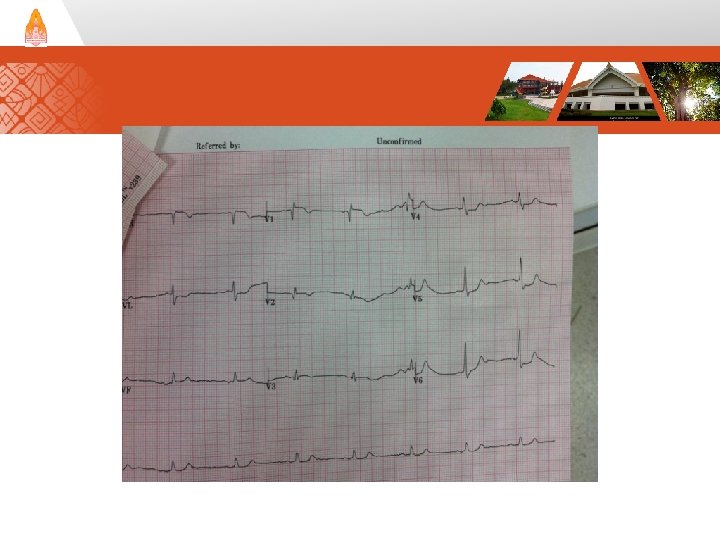
• Magnetic resonance imaging (MRI). • Duplex ultrasound (US) • Laboratory tests. check the blood's clotting status , arterial blood gases และ D-dimer level • Electrocardiogram (ECG or EKG) พบ sinus tachycardia และ RV pressure overload เชน T wave inversion ใน leads V 1 -V 4, S 1 Q 3 T 3, RBBB และ อาจพบลกษณะ ST-segment elevation มก พบบอยใน lead V 1

อาการแสดงผดปกตทพบบอยทสด • tachypnea • tachycardia อาจพบอาการแสดงของ DVT ได ในบางราย • cyanosis • RV pressure overload เชน jugular vein engorgement, RV heaving, loud P 2 sound, RV gallop และ tricuspid regurgitation murmur • hypoxemia พบประมาณรอยละ 20 และตรวจไมพบความผดปกตของ Pa. O 2 และ alveolar-arterial oxygen gradient จาก arterial blood Gas

Vena Caval filter

Surgical Management • Catheter Embolectomy : for patients in unstable condition with contraindications to thrombolytic therapy. Mechanical embolectomy has a success rate of 80%, but there is danger of distal migration of the pulmonary embolism. • Surgical Embolectomy: manual removal of the thrombus from the pulmonary artery. Extracorporeal membrane oxygenation is a temporary cardiopulmonary support system used sparingly in the treatment of patients with circulatory collapse due to pulmonary embolism. Extracorporeal membrane oxygenation is used to maintain oxygenation and tissue perfusion until the thrombus can be dissolved or removed.

Nursing Care - Preventative must be used routinely for any hospitalized patient. - Compression stockings should be placed on the lower extremities before the patient gets out of bed.

- External pneumatic compression boots, which intermittently compress the calf and accelerate deep venous flow, may be used in bed-bound patients. - Adequate hydration and early ambulation are encouraged to prevent deep venous thrombosis.

- Daily assessment of extremities for pain, erythema, and size discrepancy is vitally important. - The Homan sign (pain on dorsiflexion) is apparent in only 30% of the cases.

- The nurse must recognize risk factors for pulmonary embolism and vigilantly monitor patients who are immobilized or have had their activity restricted for unexplained tachypnea, tachycardia, and restlessness. - These signs must not be attributed to anxiety unless a physical cause has been sought first.

• The nurse should suspect pulmonary embolism as an underlying cause of syncope and cardiac arrest with pulseless electrical activity. Vigilance during anticoagulation or administration of thrombolytic agents is warranted to prevent significant bleeding complications. A decrease in hemoglobin level and hematocrit may alert the nurse to occult bleeding in the retroperitoneum or gastrointestinal tract. If the nurse encounters a change in mental status or new focal neurological deficits in a patient receiving thrombolytics, intracranial hemorrhage must be eliminated as a possible cause. An emergent neurosurgical consultation and an unenhanced computed tomography scan of the brain is warranted in this situation. • Avoidance of unnecessary phlebotomy, arterial puncture, and other invasive procedures may reduce the risk of hemorrhage during thrombolytic administration. Significant hemorrhage requires discontinuation of the thrombolytic agent and administration of cryoprecipitate or fresh frozen plasma to reverse the coagulopathy. Decreasing platelet counts during heparin administration may suggest a diagnosis of HIT.

Education of Patients • During recovery, the nurses were instrumental in preparing the patient for discharge. The nurses instructed Shelby and her family on the importance of continued warfarin administration for 3 to 6 months to prevent further thrombus development. • Foods high in vitamin K, such as dark green vegetables and apricots, must be limited during this time period to prevent decreased warfarin action. The nurses informed Shelby that a therapeutic INR value is between 2 and 3 and that adjustments in the dosage of warfarin may be needed to maintain her INR in this range.

• Shelby was advised not to use warfarin with acetaminophen, nonsteroidal anti-inflammatory drugs, amiodarone, or fluoroquinolone antibiotics because such combinations can quickly elevate the INR. • The nurses reminded Shelby to stretch every hour during confined travel and to remain well hydrated because patients with history of deep venous thrombosis or pulmonary embolism are at a greater risk for subsequent development of venous thrombosis. The nurses encouraged Shelby to recount her history of deep venous thrombosis and pulmonary embolism to future healthcare providers and to wear a Medic -Alert bracelet indicating her history of pulmonary embolism.

Nursing care plan primary nursing diagnosis : Impaired gas exchange related to impaired pulmonary blood flow and alveolar collapse. - patient’s airway - breathing - circulation are maintained - Administer oxygen immediately to support gas exchange and prepare for the possibility of intubation and mechanical ventilation. - Obtain intravenous (IV) access for administration of fluids and pharmacologic agents. - Before administration of thrombolytic agents, draw a coagluation profile and complete blood count to obtain a baseline.
 access for administration of fluids and pharmacologic agents. - Before")
- Obtain intravenous (IV) access for administration of fluids and pharmacologic agents. - Before administration of thrombolytic agents, draw a coagluation profile and complete blood count to obtain a baseline.

Nursing care plan discharge and home health care guidelines Teach the patient and family methods of prevention. Explain that patients should avoid prolonged sitting, crossing of their legs, placing pillows beneath the popliteal fossae, and wearing tight-fitting clothing such as girdles. Encourage hospitalized patients to ambulate as soon as possible after surgery and to wear antiembolic hose or pneumatic compression boots while they are bedridden. Encourage patients to drink at least 2 L of fluid a day unless they are on fluid restriction. Suggest that obese patients limit calorie intake to reduce their weight.

- ดแลใหไดรบ heparin or low-molecular-weight heparin subcutaneously or intravenously. - institute appropriate fluid administration and inotropic support to maintain a systolic blood pressure of 90 mm Hg. - If pulmonary hypertension and right-sided heart failure are present, the nurse may consider cautious use of a vasodilator such as nitric oxide.

- The nurse can provide short explanations of the diagnostic tests and invasive procedures to reassure the patient that this life-threatening condition is treatable. - Neurological and vascular assessments should be performed hourly to evaluate organ perfusion. Confusion or agitation may indicate respiratory acidosis (increased Pa. CO 2 and decreased p. H). - Weakened pulses and cool, mottled extremities are late physical findings that indicate impending circulatory collapse.

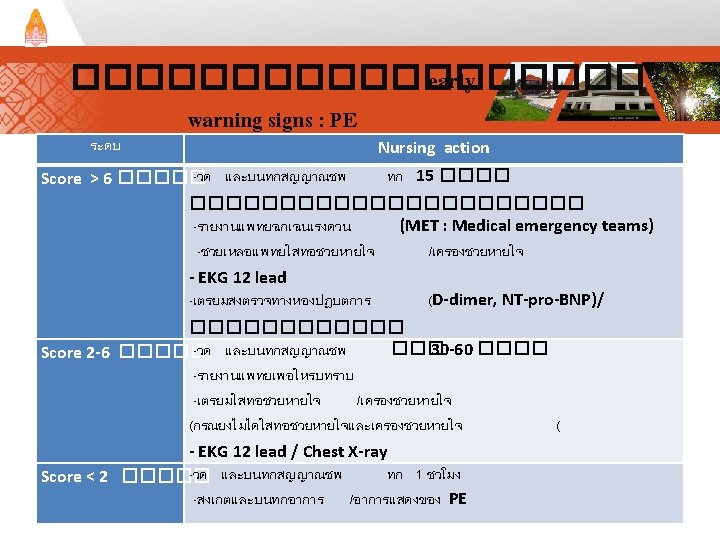
������� Early Warning sign for Pulmonary Embolism วน /เดอ น/ป คาคะแนน <2 26 สรป เกด Nursing Intervention EKG 12 lead เตรยมอปกร ณใส ทอชวยหายใ จ สงตรวจทาง หองปฏบตการ Yes )ระบ ( หมายเหต No PE yes no Result of treatment Improve no change Deteriorated Dead >6 v/s q Notify - - - แพทย 15 30 60 min min Doctor management

Thank you
- Slides: 35