Neurocardiogenic syncope Evidence review Introduction Neurocardiogenic vasovagal syncope

 syncope is one of the most common cause of syncope.")





 • Tilt-table testing is the only method for the diagnosis of neurocardiogenic")











 • Substudy (150) to assess whether the")


, with Positive")










 trial. circulation 2001 • Pts from")



 • 29 pts (53 ± 16 years; 19 women) with")


 pacing is preferred, since both")


 • The variation of intracardiac impedance is tracked every beat,")
 with severe and")









")



















- Slides: 94
Neurocardiogenic syncope Evidence review
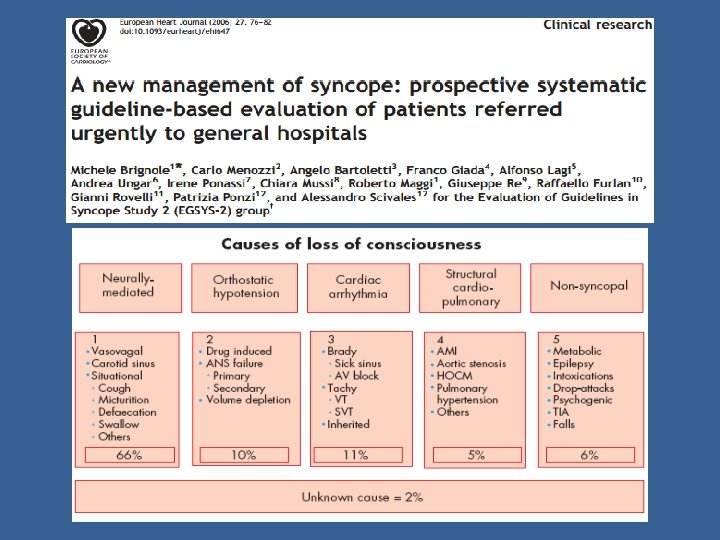
Introduction • Neurocardiogenic (vasovagal) syncope is one of the most common cause of syncope. • Occurs as a result of excessive peripheral venous pooling that causes a sudden drop in peripheral venous return. • Activation of carotid baroreceptors. • Leads to cardiac hypercontractile state, which activates mechano Rs. • Increased afferent neural traffic to brainstem. • Provokes paradoxical reflex bradycardia and drop in PVR. Mosqueda-Garcia R et al; The elusive pathophysiology of neurally mediated syncope. Circulation 2000
• provoked by prolonged standing, vigorous exercise in a warm environment, fear, emotional distress or severe pain. • Presyncopal symptoms may occur from 30 secs to few minutes before syncope. • Upto a third of pts (esp in older adults) will have little or no prodrome, results in physical trauma. • LOC is brief and recovery is rapid( 30 sec to 5 mts) Gruub et al; NEJM 2005
Incidence • The overall incidence rate of a first report of syncope was 6. 2/1000 person-years. • Incidence increases with age, with a sharp rise at 70 years. • Incidence of vasovagal syncope 1. 3/1000 person yrs. • 21. 6 % reported one or more recurrences of syncope. N Engl J Med, 2002; incidence and prognosis of syncope; Soteriades et al.
N Engl J Med, 2002; incidence and prognosis of syncope; Soteriades et al.
Prevalence N Engl J Med, 2002; incidence and prognosis of Linzer M et al; diagnosing syncope; Ann Intern Med 1997; 126: 989 -96 syncope; Soteriades et al.
Survival according to cause of syncope N Engl J Med, 2002; incidence and prognosis of syncope; Soteriades et al.
Tilt-table testing(HUTT) • Tilt-table testing is the only method for the diagnosis of neurocardiogenic syncope that undergone rigorous evaluation. • Passive tilt at angles between 60 -70⁰ for 20 - 30 mts. • A positive test is one that provokes a hypotensive episode that reproduces the patient’s symptoms.
Sutton and Benditt; evaluation & treatment of syncope. Proposed classification of tilt induced vaso vagal syncope; Euro J Cardiac Electrophysiology 1992; Sutton R et al.
HUTT Specificity & sensitivity Reproducibility • As no “gold standard” test available, exact sensitivity is unknown. • The specificity of a negative test at 60 - 70⁰ ≈ 90%. • False positive rate=10%. • Specificity of positive test more without pharmacologic challenge. • 80 -95% for an initially negative test. • 30 - 90% for initial + test, if repeated days- wks. • Long term reproducibility ≈60%. • may not produce same hemodynamic effects and changes in heart rhythm as during spontaneous episodes. Blair grubb; circulation june 2005. Randomized assessment of syncope trial: Krahn etal; circulation 2001.
• A cardioinhibitory response on tilt table testing probably is neither an appropriate surrogate marker for pacing studies, nor can it be used to predict patients who might respond to pacing. Metaanalysis on role of pacing in vasovagal syncope; Sud et al, 2007
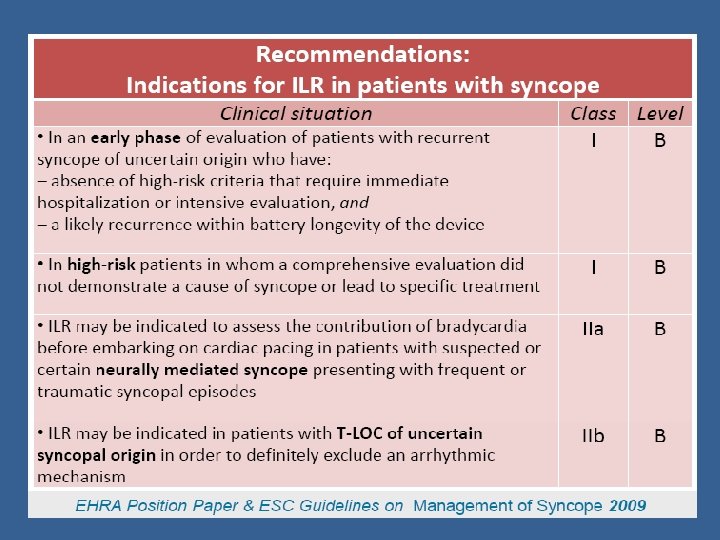
ILR • Device can store 45 mts of retrospective ECG recordings. • Reserved for pts with undiagnosed recurrent syncope( need for Sx and cost) • Diagnostic yield 25 - 40% during a period of 810 months. Fitzpatrick AP; Ambulatory electrocardiographic (AECG) monitoring for evaluation of syncope.
• ILR Inserted in 111 patients with syncope & absence of significant structural heart disease, and a normal ECG. • Tilt-testing was negative in 82 (isolated syncope) and positive in 29 (tilt-positive). • Follow up: 3 to 15 months
Results
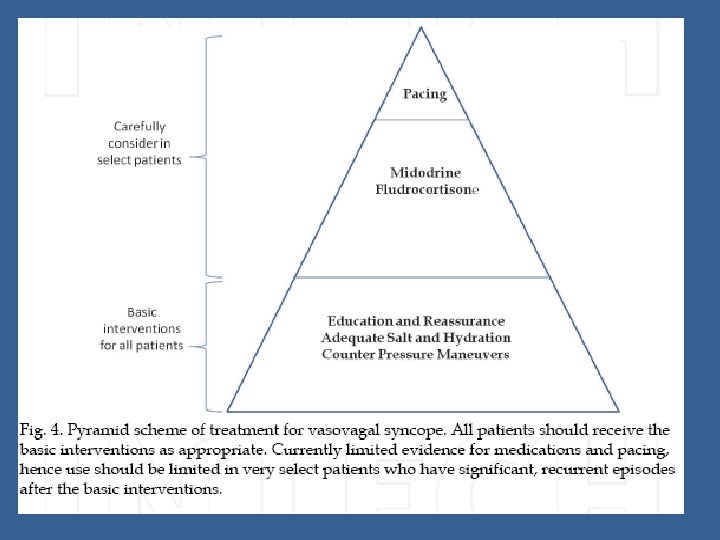
Management
Brignole et al; for the Task Force on Syncope, European Society of Cardiology. Guidelines on management (diagnosis and treatment) of syncope. Eur Heart J 2001
Beta blockers study Drug used Mean age No of episodes a yr before random. Follow Treatment Placebo up period Group group recurrence recurre nce Significa nt? Brignole et al Atenolol 50 mg/day 42 ± 12 y 2. 1 ± 1. 8 10 ± 7 months 2 /7 (28. 6%) 4/15 (25. 7%) Not reported Mahonon Atenolol 50 - 38 ± da et al 100 mg/day 13 y NA 1 month 6 /21 (28. 6%) 15/21 (71. 4%) Yes (p = 0. 02) Madrid etal Atenolol 50 mg/day 31 ± 10 y 3 1 yr 16 /26 (61. 5%) 11/24 (45. 8%) No (p = 0. 09) Sheldon etal Metoprolol (122 ± 61 mg/day) 42 ± 18 y 3 1 yr 63/106 (59. 4%) 58 /100 (58. 0%) No (p = 0. 87)
• Srikanth Vallurupalli, Smita Das; september 2010. Concluded • There is no clinical evidence for justifying the use of B 1 selective blockers in the treatment of adult neurocardiogenic syncope. • These agents may in fact lead to a higher rate of adverse events compared to placebo.
• Included all patients with 2 syncopial spells in last yr and a positive tilt test. • 208 pts (mean age 42± 18 years) with a median of 9 syncopal spells over a median of 11 years were randomized, 108( metoprolol) and 100(placebo group) • There were 63 of 108 subjects with treatment failure while taking metoprolol (39 with syncope+24 who withdrew from the study) compared with 58 of 100 with treatment failure (36 with syncope + 22 withdrawals) while taking placebo (P=0. 87).
Predictive Accuracy of Tilt Tests (POST trial) • Substudy (150) to assess whether the need for isoproterenol to produce a positive tilt response would predict a subsequent clinical benefit from metoprolol. • In the intent-to-treat analysis of subjects who had a positive drug-free tilt test, the number with treatment failure was 28 of 48 taking metoprolol and 27 of 45 taking placebo (P=1. 00). • In subjects who had a positive isoproterenol tilt test, the number with syncope was 13 of 34 taking metoprolol and 11 of 26 taking placebo (P=1. 00). • Baseline tilt-test conditions did not predict clinical benefit from metoprolol.
ETILEPHRINRE &MIDODRINE IN VVS
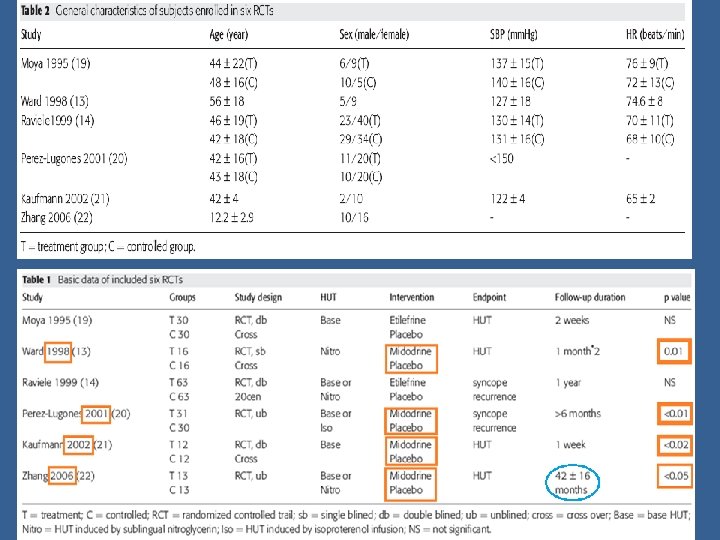
Results: Meta-analysis of the six RCTs (165 patients in the treatment group and 164 patients in the control group), shows that α- adrenoceptor agonists were more effective than placebos in treating VVS (OR = 0. 21, 95% CI: 0. 06– 0. 77, p = 0. 02). • On comparision with Etilefrine, Midodrine is a better choice for VVS.
Patients: 16 outpatients with frequent hypotensive symptoms (more than two syncopal episodes), with Positive head up tilt. Design : RCT placebo ( Midodrine Vs Placebo) controlled study of one month duration Results: Patients administered midodrine had an average of 7. 3 more symptom free days than those who received placebo (95% CI 4. 6 to 9; p < 0. 0001). Conclusion: Midodrine had significant beneficial effect in neurocardiogenic syncope over placebo
• 20 centers, 126 patients with recurrent vaso vagal syncope (at least 3 episodes in the last 2 years) and a positive baseline head-up tilt response were randomly assigned to placebo (63 patients) or Etilefrine at a dosage of 75 mg/d (63 patients). • Follow up for 1 year or until syncope recurred. • Primary end-point : First recurrence of syncope. • Result: Group treated with Etilefrine had a similar incidence of first syncopal recurrence to that of placebo group. • Concluson: Oral etilefrine is not superior to placebo in preventing spontaneous episodes of vasovagal syncope in this study.
Incluson Criteria: Monthly occurrences of syncope and a positive tilt-table test. Randomisation: A 61 patients were randomly allocated to Rx either with midodrine or with Fluid, salt tablets, and counseling. 31 patients were assigned to Rx with Midodrine. Follow-up : Results: For 6 months. At the 6 -month follow-up, 25 (81%) of 31 midodrine Rx patients and 4 (13%) of the 30 Fluid-therapy patients had remained asymptomatic (P < 0. 001). Conclusion: Midodrine appeared to provide a significant benefit in patients with neurocardiogenic syncope.
• Treatment periods: 3 months with a wash-out period of 1 week inbetween (Cross Over Trial) • Results: The proportion of patients who experienced syncopal and presyncopal recurrences did not differ significantly between Midodrine and placebo treatment (syncope: 48 vs. 65%, P=0. 22; pre-syncope: 74 vs. 78%, P= 0. 99). • Conclusion: Midodrine not useful
Role of pacing • Bradycardia has long been recognized as a component of vasovagal syncope Sharpey-Schafer, 1956. • Bradycardia also detected by pacemaker or ILR or during tilt testing during VVS episode. • This suggested pacing could prevent VVS by treating bradycardia component.
Fitzpatrick et al, 1991 • Those patients with tilt table induced syncope associated with bradycardia, underwent repeat test with temporary pacing. • This prevented syncope in >50% of subjects. • Training effect? • The hemodynamic changes seen on tilt table induced syncopal episodes may not correlate with clinical episodes Menozzi et al. , 1993
Initial pacing studies
• Objective: to evaluate pacemaker therapy for severe recurrent vasovagal syncope. • Patients with ≥ 6 lifetime episodes of syncope +a tilt-table test that induced syncope or presyncope & relative bradycardia, were randomized to receive a DDI (rate drop response) or not. • There was a marked reduction in the post randomization risk of syncope in pacemaker patients (relative risk reduction 85. 4%, 95% confidence interval 59. 7% -94. 7%; p= 0. 000022).
Results
s • 42 pts from 18 European centers were randomized to receive a DDI pacemaker programmed to 80 bpm with hysteresis of 45 bpm (19) or no pacemaker (23). • Pts with ≥ 3 syncopes over the last 2 years and a positive cardioinhibitory (VASIS 2 A and 2 B) response to tilt testing. • Followed up for min 1 yr (mean=3. 7± 2. 2). • One patient (5%) in the pacemaker arm experienced recurrence of syncope compared with 14 patients (61%) in the no-pacemaker arm (P=0. 0006). Circulation 2000; VASIS trial
Results
s • SYDIT(Syncope Diagnosis and Treatment Study Investigators) trial. circulation 2001 • Pts from 14 centers -randomized to receive either a DDD pacemaker (rate-drop response)or atenolol (100 mg OD). • Included pts with ≥ 3 syncopes in last 2 years, and positive tilt table testing with syncope occurring+ relative bradycardia. • The primary outcome-The first recurrence of syncope after randomization. • 93 pts(46 PM/47 Atenolol). • Analysis showed significance in favour of permanent cardiac pacing (recurrence of syncope in 2 patients [4. 3%] after a median of 390 days) compared with medical treatment (recurrence of syncope in 12 patients [25. 5%] after a median of 135 days; OR-0. 133; 95% CI, 0. 028 to 0. 632; P=0. 004).
SYDIT trial- results
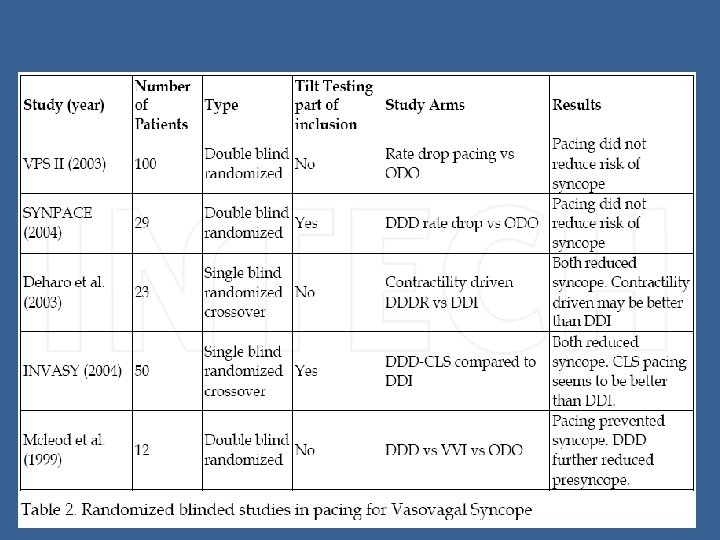
Randomized, double blind studies comparing active pacing to sensing only
Sheldon R; Connolly S • 100 patients received pacemakers (pacing with rate drop sensing vs sensing only). • The cumulative risk of syncope at 6 months was 40% for the control group and 31% for the actively paced group. • The relative risk reduction in time to syncope with pacing was 30% (p = 0. 14) • Pacing did not reduce the risk of syncope.
European Heart Journal (2004) • 29 pts (53 ± 16 years; 19 women) with severe recurrent vasovagal syncope (median 12 syncopes in the lifetime) and 1 syncopal relapse after head-up tilt testing underwent implantation of a pacemaker and were randomized to pacemaker ON or to pacemaker OFF. • During a median of 715 days of F/U, 8 (50%) patients randomized to pacemaker ON had recurrence of syncope compared to 5 (38%) of patients randomized to pacemaker OFF. • No significant difference in the subgroups of patients who had a mixed response and in those who had an asystolic response during head-up tilt testing.
Synpace trial: analysis
Kaplan–Meier estimates of the probability of remaining free of syncopal recurrence
Pacing mode • In general dual chamber (AV sequential) pacing is preferred, since both sinus and AV nodal function can be affected during a vasovagal episode. • Mc. Leod, Wilson, Hewitt, Norrie, & Stephenson, 1999 • DDD pacing was compared to VVI and to sensing only (ODO) in 12 children with vasovagal syncope and found both modes of pacing to prevent syncope. • All 12 were implanted with dual chamber pacemakers. • Then programmed to ODO, VVI, and DDD with rate drop response for four month periods. Parents and patients were blinded to the pacemaker mode. • Both pacing modes prevented syncope. DDD was better than VVI for reducing presyncopal events.
Rate-changing programming: • The goals of these programming strategies are to treat the bradycardia and also to compensate for the vasodepressive response. • Rate hysteresis triggers pacing at a higher rate when the intrinsic heart rate falls below a preset rate. • Rate drop response results in high rate pacing for a few minutes when a drop in native heart rate is detected. • Rate response programming -used in many syncope studies like VPS and VPS II.
Ammirati et al; 1998 • Compared DDD with rate drop response to DDI with rate hysteresis. • Randomized 20 VVS pts with cardioinhibitory response during tilt testing to rate drop response or rate hysteresis. • During the 17 month follow up, no pts with rate drop response had syncope but 3 of 8 in the rate hysteresis group. • Hence rate drop response was found to be more effective.
Closed loop stimulation (CLS) • The variation of intracardiac impedance is tracked every beat, so that contractility changes can be detected in the early phase (prior to changes in heart rate) of a vasovagal episode and dual chamber pacing is activated. • The INVASY trial randomized 55 patients with vasovagal syncope and positive tilt test to a CLS pacemaker or DDI and found CLS to be effective in preventing syncope over two-year follow-up period. • The recently completed (not published) SCANSYNC study also used CLS pacing.
• 50 pts (27 males, mean age 59± 18 year) with severe and recurrent vasovagal syncope and positive Head Up Tilt Test (HUTT) with cardioinhibition, received a CLS pacemaker. • Randomized to DDD-CLS(17/26) and DDI mode (9/26) pacing was performed only during the first stage of the study (first year). • All the 24 patients recruited in the second stage of the study (second year) were programmed in DDD-CLS mode. • Follow up period(mean 18. 9± 4. 2 ; range 12 -36 months)
Results
• 7/9 pts in the control arm crossed over to CLS arm (4 pts after 1 yr; 3 pts at the end of study period). Predictive value of HUTT: • HUTT was performed at the end of 1 st yr or just before cross over, in 39/50 pts (30 in CLS and 9 in control group). – 15 HUTTs (38%) had a response concordant with the clinical picture during F/U (7 in control were + and 8 in CLS were -) – 24 HUTTs (62%) -22 CLS arm and two syncope-free in the DDI arm had a positive response with hypotensive presyncopal symptoms, but without asystole. q The mean time-to-syncope/presyncope was 19. 7± 3. 8 min at 1 year, compared with 13. 9± 4. 2 min at recruitment, a median increase of 42% (P=0. 001).
ISSUE 2 Trial
• 392 patients with recurrent Syncope in the preceding 2 years were recruited. • ILR was put to all patients • After a median of 9 months 103 had syncope recurrence. • Total 53 patient had asystole during syncope most subsequently received dual chamber pacemaker.
• On comparison of Pacemaker group with non pacemaker group, Pacemaker group was associated with relative reduction of 80%. This shows that pacing guided by ILR findings was both safe and efficacious
ISSUE 3 TRIAL
ISSUE 3 Trial design: Patients with neurally mediated syncope and documented asystole on implantable loop recording underwent permanent pacemaker (PPM) implantation and were randomized to PPM on or off. Patients were followed for 2 years. Results (p = 0. 039) 100 • % 57. 0 • Primary endpoint: Incidence of first syncope recurrence for PPM on vs. off: 25% vs. 57%, p = 0. 039 Lead dislodgement: four patients; subclavian vein thrombosis: one patient 50 Conclusions 25. 0 0 Primary endpoint PPM-on (n = 38) PPM-off (n = 39) • Dual-chamber permanent pacing was effective in reducing recurrence of syncope in patients ≥ 40 years with severe asystolic neurally mediated syncope • Highlights the utility of an implantable loop recorder in this subgroup of patients Circulation 2012
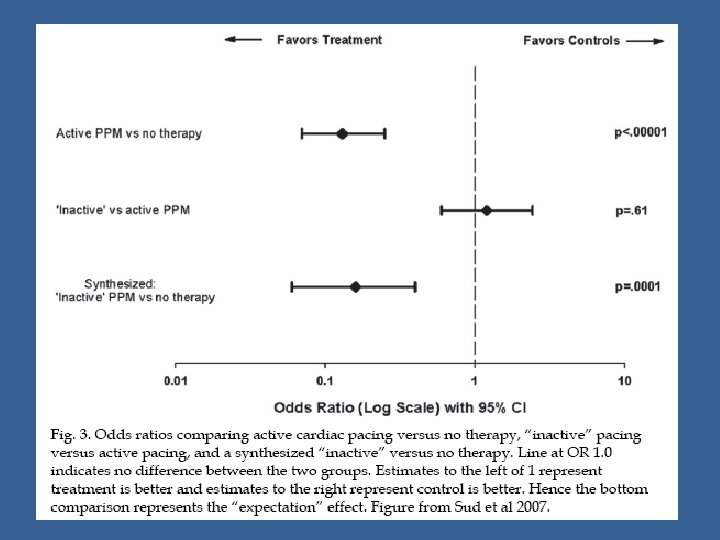
Meta-analysis Sud et al, 2007 • Blinded trials for pacing (in contrast to open label trials) in VVS do not show a benefit, even in patients with marked cardioinhibitory response on tilt table testing. • The benefits seen in open label, unblinded trials may be due to an expectation effect. • Synthesized a unique comparison between “inactive” pacing and no treatment and found that the expectation response alone reduces the odds of syncope by 84%.
Placebo effect in pacing for vasovagal syncope • The placebo effect can be powerful and may be due to expectation effects of patients and health care providers, conditioning effects in patients, along with biases in patient assessment and reporting. • The vasodepressor and cardioinhibitory components may vary in each patient, with different episodes and 50% -83% of syncopal episodes may not have a cardioinhibitory component. • This also explain why pacing does not seem to be of benefit in vasovagal syncope.
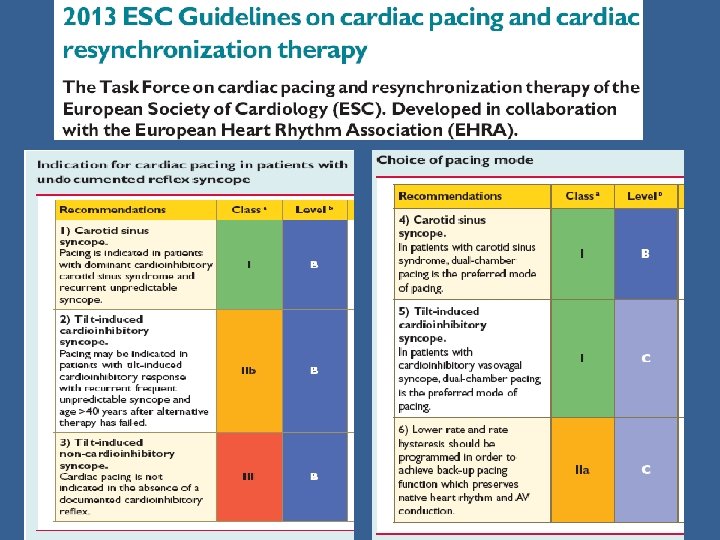
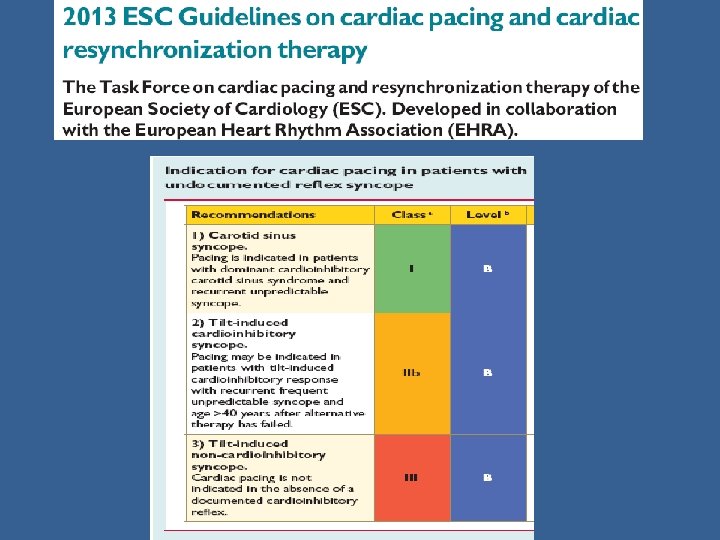
Guidelines for the diagnosis and management of syncope (ESC version 2009)
Clinical perspectives: • The decision to implant a pacemaker needs to be made in the context of a benign condition that also affects young pts. • So cardiac pacing should be limited, as a last resort choice, to a highly selected small proportion of patients affected by severe reflex syncope. • Suitable pts are those >60 years with a history of recurrent syncope beginning in middle or older ages and with frequent injuries, probably due to presentation without warning. ESC Guidelines 2013
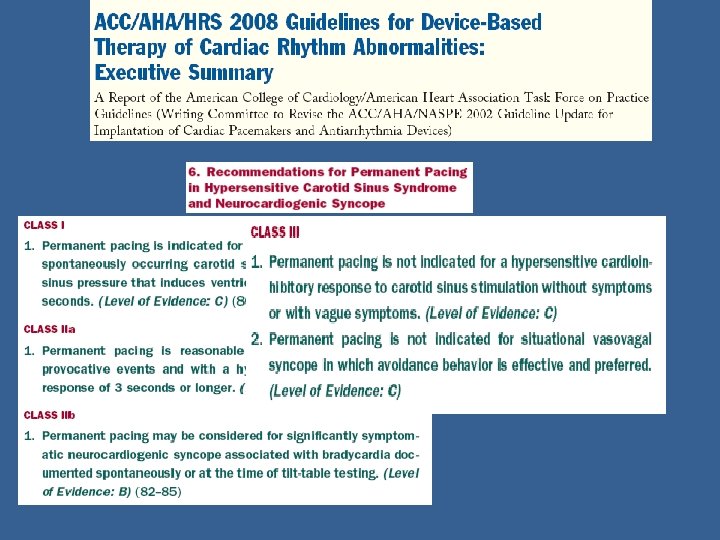
Evidence review CAROTID SINUS SYNDROME
Questions to be answered…. • • How to identify a person with CSS? Role, reproducibility of CSM? Do you have to pace them? Pace mode selection?
Age distribution • CSH is an age-related phenomenon – Rarely diagnosed in patients with syncope < 50 years – Prevalence increases with advancing age Unexplained syncope—is screening for carotid sinus hypersensitivity indicated in all patients aged > 40 years? J Neurol Neurosurg Psychiatry 2006; 77: 1267– 1270
Carotid sinus massage • A ventricular pause lasting >3 s and/or a fall in systolic BP of >50 mm. Hg defines carotid sinus hypersensitivity (CSH). • When associated with spontaneous syncope, CSH defines CSS.
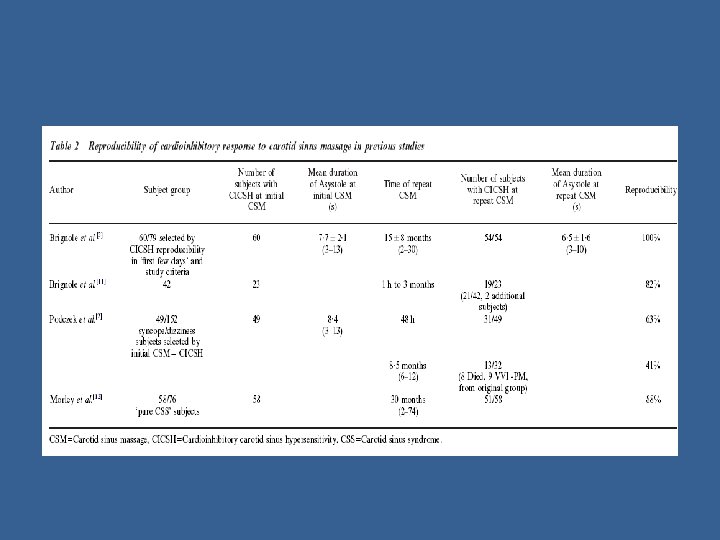
• Europace 2002 • 64 subjects with CICSH and unexplained or recurrent falls. (61% female, mean age 71· 8 years, median 2 falls in the previous year) completed 1 yr F/U and had CSM performed on 4 occasions (twice before randomization, at 6 months and 1 yr). Results • CICSH was demonstrated on 82% of occasions, 75% on right CSM and 77% whilst the subject was supine. • Before randomization, and at 6 months and 1 year, 91%, 67%, and 70% of subjects had reproducible CICSH respectively. • Half had CICSH on all 4 occasions. • Only 17% had a consistent response on the same side in the same position
Cardioinhibitory carotid sinus hypersensitivity predicts an asystolic mechanism of spontaneous neurally mediated syncope. Europace 2007, Maggi, Menozzi etal • Correlated CSH with that observed during a spontaneous syncopal relapse by means of ILR. • 18 CSM+ vs 36 CSM- pts, suspected recurrent neurally mediated reccurent syncope. • Asystole >3 s was observed at the time of the spontaneous syncope in 16 (89%) of CSH patients and in 18 (50%) of the control group (P = 0. 007). • Sinus arrest- 72 vs. 28%, P = 0. 003 • 14 CSH patients with asystole received DDI. • Syncope burden decreased from 1. 68 to 0. 04 episodes per yr person. (98% relative risk reduction).
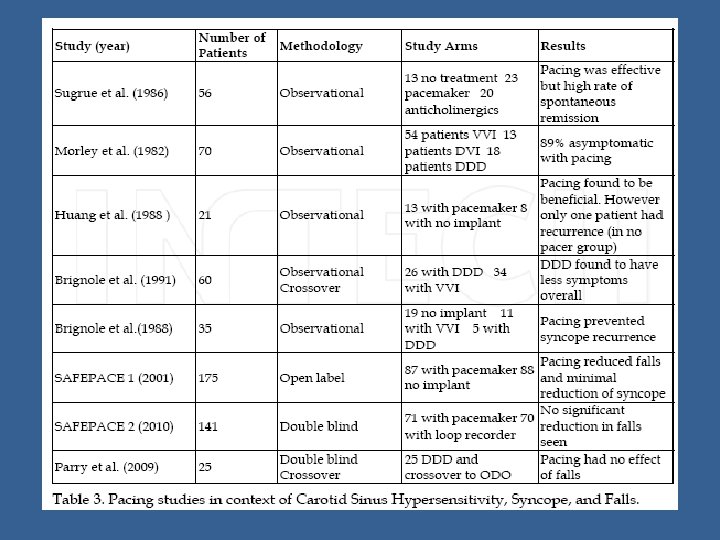
Role of pacing in CSS Permanent pacemaker is an effective treatment The role of pacemaker in hypersensitive carotid sinus syndrome Europace (2011) 13, 572– 575
JACC 2001 • The aim of the study was to determine whether cardiac pacing reduces falls in older adults with CICSH.
RESULTS • The primary outcome was the number of falls during one year of follow-up. • Falls (without LOC) were reduced by two-thirds: controls reported 669 falls (mean 9. 3; range 0 to 89), and paced patients 216 falls (mean 4. 1; range 0 to 29). Odds ratio 0. 42; 95% CI: 0. 23, 0. 75. • Syncopes were also reduced but there were much fewer syncopal events than falls— 28 episodes in paced patients and 47 in controls. • Injurious events were reduced by 70% (202 vs 61).
Heart 2010 • To assess the efficacy of dual-chamber pacing in older patients with CICSH and unexplained falls. • A multicentre, double blind, randomised controlled trial. • Patients aged >50 years, with two unexplained falls and/or one syncopal event in the previous 12 months for which no other cause is evident apart from CICSH. • 141 pts -randomized to rate responsive pacemaker or implantable loop recorder. • The primary outcome- the number falls after implantation.
Results • 141 patients were recruited from 22 centres. • Mean age was 78 years and mean follow-up 24 months. • The overall relative risk of falling after device implantation compared with before was 0. 23 (0. 15 to 0. 32). • No significant reduction in falls was seen between paced and loop recorder groups (RR=0. 79; 95% CI 0. 41 to 1. 50).
• These results question the use of pacing in CICSH. • The study was underpowered • Patient characteristics differed from those in Safepace-1 (participants were physically and cognitively frailer)
• • Europace 2011 To assess the outcome of patients with CSS treated with pacemaker and to determine predictors of symptom recurrence. A retrospective analysis of 138 patients in whom pacemaker was implanted for CSS. Mean age was 69± 10. 7 yrs an 75. 4% were men. Mean follow-up period was 4. 9± 4. 4 yrs. 21 (15. 2%) pts presented mixed CSS and 117 (84. 8%) CICSS. • After PPI, 115 (83. 3%) pts had no further symptoms, 8 (5. 8%) presented minor symptoms and in 15 (10. 9%) the symptoms remained unchanged. • Among pts with symptoms recurrence, 8 (38. 1%) had mixed CSS and 15 (12. 8%) cardioinhibitory CSS. • Mixed CSS was the only independent predictor of symptoms recurrence in total population {hazard ratio (HR) 2. 84 [95% CI 1. 20– 6. 71]; P= 0. 017.
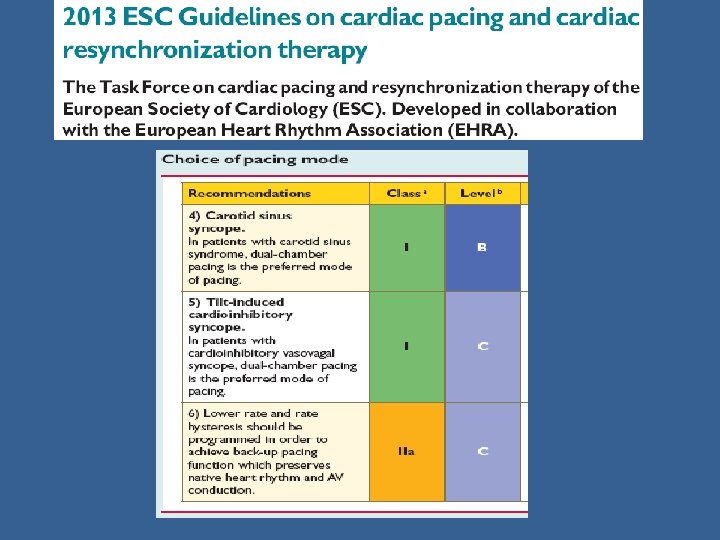
MODE OF PACING
Is DDD Superior to VVI Pacing in Mixed Carotid Sinus Syndrome? An Acute and Medium-Term Study • • Pacing and Clinical Electrophysiology 1988; brignole et al 23 pts affected by symptomatic mixed carotid sinus syndrome- received a DDD pacemaker and entered a 2 month two period single-blind, randomized, crossover study on DVI/DDD versus VVI mode. During the DVI/DDD period, no syncope occurred in any pts, minor symptoms persisted in 11 (48%) of them. During VVI period syncopes recurred in 3 pts, symptoms requiring the withdrawal of VVI pacing and premature DVI/DDD reprogramming in 8 pts, minor symptoms in 17 (74%). A comparison between 14 pts who preferred DVI/DDD period (Group A), and the remaining 9 who noted no preference between DVI/DDD and VVI period (Group B). Group A patients had a greater pacemaker effect (-34 ± 16 mm. Hg vs -16 ± 14 mm. Hg) and a higher prevalence of symptomatic pacemaker effect (50% vs 0%)of ventriculo-atrial conduction (78% vs 44%) and of orthostatic hypotension (50% vs 11%) DVI/DDD pacing is more effective than VVI in 61% of patients.
A study comparing VVI and DDI pacing in elderly patients with carotid sinus syndrome Shona J Mc. Intosh et al; Heart 1997 • Prospective double blind randomised cross over study. • 30 consecutive pts >60 years with CSS referred for cardiac pacing. • Patients underwent dual chamber PPI and randomised to 2 three month periods of VVI and DDI pacing. • Main outcome measures-Responses to cardiovascular tests (vasodepression during CSM, pacemaker effect, postural BP measurements and response to head up tilt) and symptoms.
Results • 11 pts were unable to tolerate VVI pacing and had to be withdrawn early from this limb of the study (group A). • 14 pts had no preference (group B). • No patient preferred VVI. • Elderly patients with carotid sinus syndrome are likely to develop symptomatic hypotension following single chamber ventricular pacing.
Thank you