POSTURE AND POSTURAL ANALYSIS Each part of the










 Pectus karinatum (Pigeon breast) Barrel Chest Harrison")





 Cervical Vertebras: Normally, there is")
")

 Head: Frontward Cervical Vertebrae: Slightly extended Thoracic vertebrae: lower lumbar")
 Standard Posture: there is a complete balance")














 Genu Recurvatum (hyperextension) • b) Flexion in the")
 Anterior Pelvic Tilt • b) Posterior Pelvic Tilt")


 Lordosis • b) Kyphosis • c) Kypho-lordosis")
 Shoulders come to the front with rounding (protraction)")
 Hallux vagus, b) Hammer fingers Hallux")
 Tibial Torsion b) Genu Varum (0 leg) c) Genu Valgum (X")
 is evaluated on the")
: a) The collapsed chest, b) Funnel type chest, c) Barrel chest,")
 Collapsed Chest: It is the concave or flattened view of the")
 Height difference of both shoulders, b) Round shoulder The difference")
 lateral flexion of the head to the")
 Calcaneal tendon displacement to inside (pronation)")






 Neuropathic Scoliosis: 1. Scoliosis after lower motor neuron")








- Slides: 69
POSTURE AND POSTURAL ANALYSIS
• Each part of the body is placed in the most appropriate position relative to the whole body and adjacent segment. • It means the best posture achieved with the least effort.
The importance of posture • • • It affects respiratory, circulatory, nutritional and gastrointestinal system functions. Prevents overloading of muscles, tendons and bones. Gives an idea about the psychological state of the person. Familial and developmental characteristics Nutrition Length, body type sport activities Business conditions Personal and psychological features Leg Length Differences
• The body achieves a smooth posture as a result of the harmonious operation of many muscles to provide stability during the muscle activity or as a basis for a movement. • Muscle shortness tests, normal joint movements, anatomical positions, axes and planes • Body type • Body balance • Layout of the body parts • Leg length measurement forms the basis of posture analysis.
Posture can be divided into active and inactive posture. Inactive postures: Postures taken to rest or sleep. Active postures: In order to maintain these postures, many muscles need to work integrally. They are divided into static and dynamic postures. STATIC posture: Posture in sitting, standing and lying DYNAMIC posture: The position of the body during movements. As a result of the movement, it is an active posture that tries to adapt to the changing environment conditions. The muscle strength required for the formation of static and dynamic postures varies according to the type of posture and the physical characteristics of the person. Generally used muscle groups are the muscles that hold the body in an upright position by resisting the effect of gravity. They are called antigravity muscles and usually have an extention function. These muscles are fan-shaped and their function is to expose the force rather than speed.
POSTURAL REFLEX • Reflex is an efferent response given to an afferent impulse. • The efferent response in the posture is the motor response, and the antigravity muscles are the main effector organs. • - Muscles: The neuromuscular and neurotendinous spindle bodies in the muscle record tension changes in the muscle. An increase in tension leads to stimulation and a reflex contraction in the muscle (tension reflex). • -Visual: The senses of vision perceive the changes in body position according to the environment and inform the center. Eyes are the receptors of the correction reflex “that the body and head need to fit into the upright position. • - Ears: The movement of the fluid in the semicircular canals in the inner ear stimulates the vestibular nerve. Each of these semicircular channels is on a separate plane and perpendicular to each other. Any movement of the head moves the fluid in the channels. As a result of this stimulation, it is possible to recognize the movement and to know its direction.
• In addition to these, the importance of skin and joint mobility in posture is important. • Especially the feeling of pressure of the foot base is very important. • In situation of lack of mobility, the posture remains fixed, and it is not possible to make changes to the movements. • Muscles, eyes, ears, impulses from the skin are coordinated in the central nervous system. • The main centers providing coordination are the cerebral cortex, cerebellum, nucleus ruber, vestibular system, reticulate formation and proprioceptive pathways.
Body type Ectomorphic Tall and thin Endomorphic Short and fat Mesomorphic Athletic and muscular
Body balance Anteroposterior balance Body Weight to the front of the foot transfer to the posterior part of the foot Lateral balance Body weight Right Transfer to the left
Layout of the body parts Head From lateral: shoulder joint and auricle Anteriordan: Suprasternal notch with mandible Shoulders Shoulder height difference Scapula, acromial processes and clavicle Scapula Leaving from the middle line or chest wall
Chest Crashed Chest Pectus excavatum (Funnel chest) Pectus karinatum (Pigeon breast) Barrel Chest Harrison trough Abdomen Oil distribution, protrusion or precipitation Çökük göğüs Pektus ekskavatum (Huni göğüs) Pektus karinatum (Güvercin göğsü) Fıçı göğüs Harrison oluğu
Spine kyphosis Kypholordosis Scoliosis Increased lordosis Flattened back Hips SIAS and crista iliaka levels
Legs Genu valgum and varum Genu rekurvatum Tibial torsion Feet Pes varus and valgus Pes planus and kavus Metatarsal arc changes Hallux valgus, claw finger, hammer finger
The hip and knee joints are in full extension because they support other parts of the body in a relaxed (standing) position. In the last few degrees of extension movement of the knee joint, rotation is added to the motion and the joint is locked tightly. M. Gastrocnemius is the main muscle that provides stability in the ankle. Since this muscle is covered by two joints, when the high-heeled shoe is worn, the stabilization effect is reduced, because it becomes somewhat loose. In normal standing position, the body will prevent antigravity muscles from shaking, depending on gravity. If standing for a long time, the weight is transferred from one side to the other and usually asymmetrical, sometimes symmetrical positions are taken to prevent fatigue.
POSTURE TYPES FOR LATERAL POSTURE ANALYSIS
STANDARD POSTURE Head: Neutral position (no forward and backward) Cervical Vertebras: Normally, there is mild anterior convexity. Scapula: in straight position according to upper back Thoracic vertebrae: slightly convex to posterior. Lumbal vertebrae: slightly convex to the anterior. Pelvic: It is in neutral position and SIAS are in the same vertical plane with symphysis pubis. Hip Joint: In neutral position (no flexion-extention) Ankle: It is in neutral position.
KYPHO-LORDOTIC POSTURE Head: Frontward Cervical Vertebras: Hyperextention Scapula: Abduction Soil Vertebrae: Increased Flexion (kyphosis) Lumbal Vertebras: Hyperextension (lordosis) Pelvis: Anterior Pelvic Inclination Hip Joint: Flexion Knee joint: Slightly hyperextension Ankle: Slightly plantar flexion due to backward inclination of the foot.
FLAT BACK POSTURE Head: Frontward Cervical Vertebras: Slightly in extention Thoracic vertebrae: The flexion of the upper thoracic vertebrae is increased and the lower thoracic vertebrae are flattened. Lumbal Vertebrae: flexion (flat), decreased concavity. Pelvis: Posterior pelvic tendency Hip Joint: Extension Ankle: Slightly plantar flexion.
LOOSE POSTURE (ROUND BACK) Head: Frontward Cervical Vertebrae: Slightly extended Thoracic vertebrae: lower lumbar region flexion, concavity is reduced (flattened). Pelvis: Posterior pelvic tilt tendency Hip Joint: Hyperextension with pelvic displacement of the pelvis, Knee joint: hyperextension Ankle: It is in neutral position.
POSTURE TYPES FOR POSTERIOR POSTURE ANALYSIS a) Standard Posture: there is a complete balance between the body, pelvis and lower extremity muscles on the right and left sides of the body. b) the gravitational line to the left on the center line of the body, or c) The posture on which it is left
BAD POSTURE • It is an insufficient posture for individuals. Does not serve the purpose exactly. It also causes unnecessary muscle contraction of the muscles. Compensations can be seen. • For example; Due to the shortening of the hip flexors, the mobility of the hip is reduced, the lumbar region is brought to the hyperextension and the weight is tried to be transferred to the feet and the lordosis increases. • In this case, the muscles do not work more, but the muscles are shortened and the antagonist muscles are prolonged and weakened. In addition, tether strain and muscle cramps are seen.
• The appearance of the bad posture is not beautiful. Since the clothes are not good on the person, the psychology created by this will have negative effects on the posture. • Whether it is to move or to maintain a movement, more than necessary contractions will result in insufficient posture and unnecessary energy expenditure. • Factors that can cause bad posture: Muscle weakness, force imbalance between the muscles, localized stiffness, pain, fatigue and occupational stresses. • When the causes disappear, posture that does not persist, disappeared immediately falls outside the limit of bad posture.
Correction of posture disorders Detecting the problem Education; teaching correct posture Correction of ergonomic conditions Stretching and strengthening exercises biofeedback Periodic control
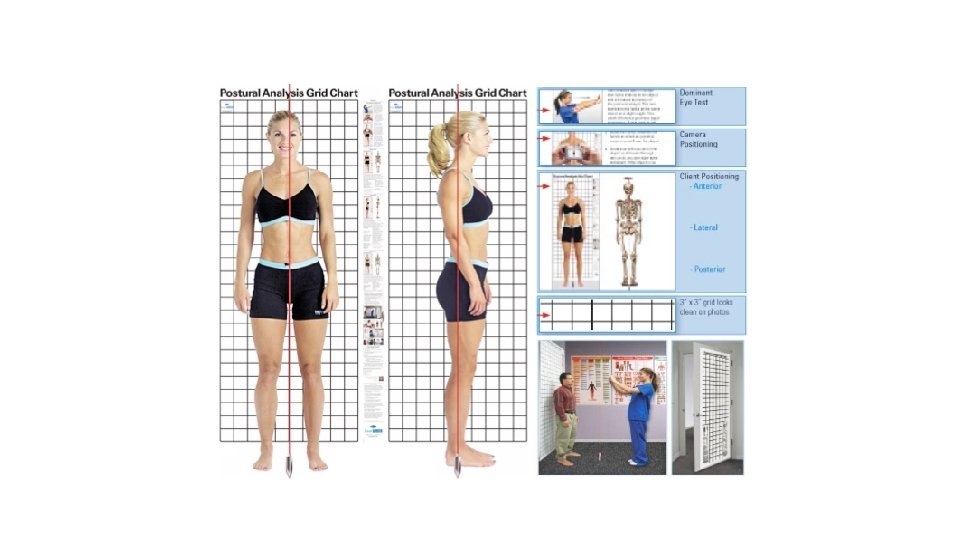
POSITION OF THE PATIENT IN POSTURAL ANALYSIS Posture analysis is performed while standing upright. There are some points that should not be ignored when analyzing this position. Person gains good or bad posture as a result of some factors. Structural changes or physical adaptations occur due to pain in the neck, lower extremity or limb vertebral. For example, as a result of lower back pain, a person makes a number of changes in his posture to find a position in which the pain decreases. This position is free from the symptoms and constitutes the normal posture of the patient. When doing posture analysis, the patient should be told to stand in the position where he feels comfortable. If a person provides standing posture by creating a posture disorder, there is a posture error and this is the person's normal posture. When the person is told to stand upright, the symptoms are revealed. There will be a difference between posture analysis performed in this position and comfortable standing posture.
• Standard good posture; There is no real postural difference between standing up in a position where people feel comfortable and standing upright. • It is very important for a person to be aware of his / her stance or to perceive this stance. Because the degree of perception of a person's normalness is related to the formation of a normal, correct posture. Posture analyzes performed at certain hours of the day differ according to external factors and internal factors. If the perception of posture is good and the person is aware of his normal posture, there will be no change in the evaluations made at different times.
Ideal Standing Posture Center of gravity from lateral view Lateral malleol Knee joint in the middle In front of the sacroiliac joint From the big trochanter Lumbar vertebrae Shoulder joint Cervical vertebrae Through earlobes
Center of gravity from Anterior Between heels Pelvis Spine Sternum Skull passes through midpoints. SIAS and shoulders are at the same level in the horizontal plane.
Viewed from the posterior Knees Hips Krista iliakalar Scapula levels Shoulders Ears Occipital protrusions are at the same level in the horizontal plane.
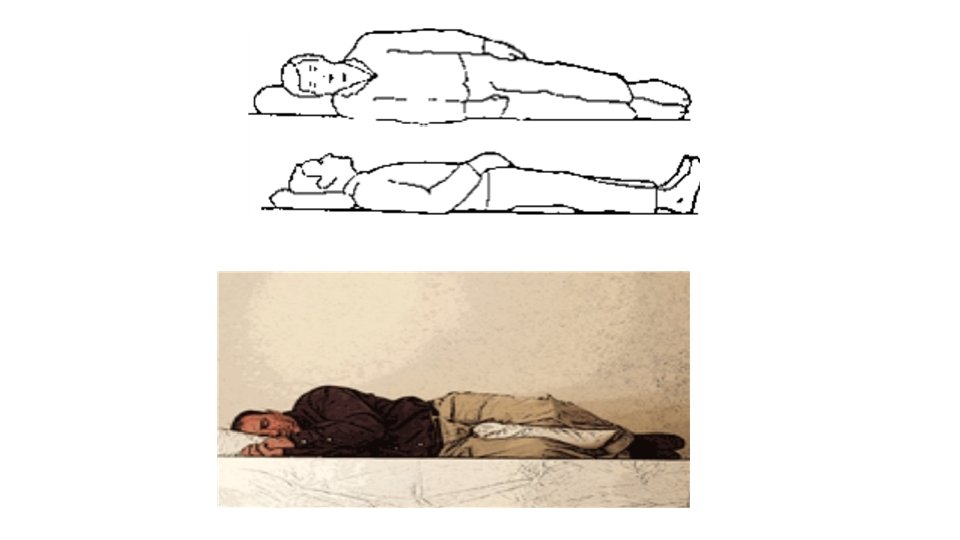
Ideal lying position • The normal axis of the spine should be protected. • Pillow head should support. • The high pillow forces the head to flexion and lateral flexion to the side lying in supine position. • The bed should not disturb the hard parts of the body and should be soft enough to support the other segments. • Lying is the least energy spent position.
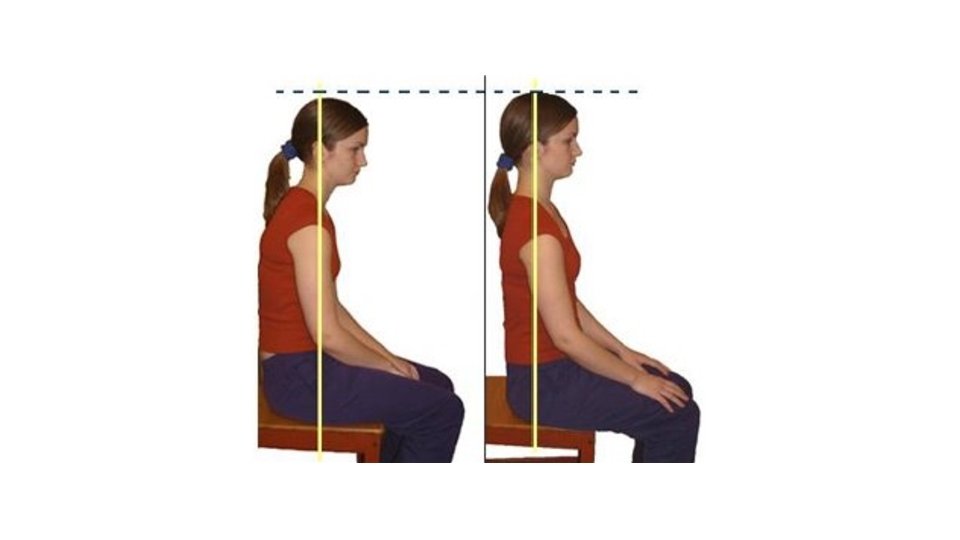
Ideal Sitting Posture • The support surface is wide. • Lower limbs may loosen. • The center of gravity should be located in front of the ischial tuberositas and the thoracic vertebra. • The lumbar spine should be in the midflexion, • Physiological curvatures should be maintained. • Legs weight supported by feet
The posture analysis is followed in the following order: • 1 Story • 2 -Body Type: It is possible to classify body types in various Shapes. One of them; ectomorphic, mesomorphic and endomorphic body shape. • a) Ectomorphic: The nervous system comes from the word ectoderm where the skin and special sensory organs are formed. Thin, long-type, light-skinned, forearms are long, weak and strong. • b) Mesomorphic: derives from the word mesoderm originating from muscle, bone, heart and blood vessels. The body is square type, and wide as a whole, the skin is thick. • c) Endomorphic: originates from the word endoderm originating from the digestive system. The body is in the form of a sphere. They are easily obese, their muscles are not too strong, the limbs are short and thin to the tip. The skin is thin and velvety. • When deciding on these, the person's bone structure is taken into consideration. Generally the type of body can be determined by examining the bone structure of the wrist.
• 3. Body Balance: It is normal if body weight is delivered by distributing training on both legs. If there is an abnormality in the anterior-posterior direction, it is called anterior or posterior balance, depending on whether the weight is given to the anterior part of the foot or to the heels. The weight is given to one of the right and left feet is called the lateral balance. It is called den right lateral or left lateral balance lateral according to the situation. • 4. the body; Right and left lateral, anterior and posterior analysis are performed.
LATERAL POSTURE ANALYSIS • 1 -Foot long arc: Postural deviations may be observed in standing up, walking or running. • There a transverse and a longitidunal arc. The long arc in terms of posture is very important. This arc consists of the calcaneus talus, navicular and some bones. The deviation of the arc from normal can be in 2 ways: • a) Reduction of arc (pes planus) • b) Increase of arc (pes cavus)
• The person should stand on a hard floor with two feet of training weight. • Scaphoid tubercle of the navicular bone in a normal standing; falls on a line drawn to the center of the metatarsophalangeal joint of the medial malleolus and the thumb (feiss line) • The grades of the flat base are evaluated according to the scaphoid tubercle that is separated from this line and towards the ground. • If the tubercle has fallen by 1/3 of the distance between the Feiss line and the ground ıt is 1 st degree, 2 nd degree if dropped to 2/3, If it touches the ground completely, there is a 3 rd degree pes planus. If the tubercle remains above the Feiss line, the pes cavus is mentioned.
• 2. Knees: • a) Genu Recurvatum (hyperextension) • b) Flexion in the knees • When looking at hyperextension in the knees, bone structure should be taken into consideration not in the muscles. • If the femur line has a definite angle, facing the aperture with the tibia, there is a genu recurvatum. The definitive diagnosis is made by examining the bone structure (knee joint) with X-Ray.
• 3. Pelvis: • a) Anterior Pelvic Tilt • b) Posterior Pelvic Tilt • M. Rectus abdominis adheres to the pubis and pulls the pelvis towards the sternum. • M. Sartorius, M. Tensor fascia lata and M. Rectus femoris start from SIAS and pull the pelvis down. • While the pelvis is in neutral, there is mild scoliosis in the lumbar spine. Anterior or posterior pelvic tilt occurs when the balance deteriorates
In anterior pelvic tilt, the vertical position between the SIAS and the symphysis pubis is disrupted and the SIAS vertical line remains in front of the vertical line passing through the symphysis pubis. Since the angle between pelvis and femur decreases, hip flexion, hyperextension of lumbar vertebrae and lumbar lordosis increase occurs. In the posterior pelvic tilt, the SIAS and the symphysis pubis vertical line, the SIAS, remain ın posterior. The extension of the hip in the posterior pelvic tilt and the flexion of the lumbar vertebrae cause the lordos to decrease and the back to flatten. ● ● In lateral pelvic tilt, one of the SIAS is located higher. ●
The angle of the line connecting the SIAS and the SIPS with the horizantal plane is the pelvic inclination angle. This is normally 7 -8. 5º. The increase in pelvic inclination angle is anterior and the decrease is considered as posterior pelvic tilt. Before starting the exercise program for pelvic tilt, the causes of this condition should be determined and the level of the pelvis should be checked for symmetrical or asymmetric. Pelvic tilt is measured by electro-goniometer. If the pelvic inclination angle increases, this means anterior, if decreases that means posterior pelvic tilt. The goniometer is placed in SIAS and SIPS.
• 4. Columna Vertebralis: • a) Lordosis • b) Kyphosis • c) Kypho-lordosis • d) Round back • e) Flat back
• 5. Shoulders: • a) Shoulders come to the front with rounding (protraction) • b) Excessive withdrawal of the shoulders (retraction) • Rounding on the shoulders is analyzed. • 6. Head: • a) Is the bond prominent • b) Is the bond withdrawn • c) Has the mandible tilted upwards • d) Has the mandible tilted downwards
ANTERIOR POSTURE ANALYSIS • • 1. Toes: a) Hallux vagus, b) Hammer fingers Hallux Vagus: Deviation of the big toe from the metatorsophalangeal joint towards the center of the foot. It is usually with processus at the medial edge of the MTP joint or foot. Hammer Fingers: It is a curling appearance of the toes from the MF joint to hyperextension, from the interphalangeal joints to flexion. Both the long flexor and the long extensor muscles may be shortened. Depending on the shoe pressure, the dorsal faces of the fingers protrude. 2. Feet: a) Inversion b) Eversion
3. Knees: a) Tibial Torsion b) Genu Varum (0 leg) c) Genu Valgum (X leg) a) TIBIAL TORSION: Tibial torsion is inward twisting of the tibia (shinbone) and is the most common cause of intoeing. It is usually seen at age 2 years. Males and females are affected equally, and about two thirds of patients are affected bilaterally. Patelas look at each other like ”squint eyes. If a person is told to stand flat with the patellas facing upwards, then the feet take an outward position. • b) GENU VARUM: The patient stands while the medial malleols are touching each other. The knees should be loose and not compensating for hyperextension. In this case, if the distance between the knees exceeds 1 -2 cm and if the knees do not join, there is genu varum. • c) GENU VALGUM: The patellas face up and the medial edges of the knees stand slightly touching each other. In this case, if there is more than 1 -2 cm distance between the medial malleols, there is genu valgum. One side may be more than the other. In such a case, shortening of the related leg will also occur. • • •
• 4. Hips: • Height difference (lower extremity shortness) is evaluated on the right and left sides. • The right or left hip may be higher. The distance of the SIAS to the ground or the medial malleolus is measured. • • 5. Abdominal Area: a) Abdominal muscles weakness b) The transverse groove is evaluated in the upper abdominal wall. If the abdominal muscles are weak and loose, the abdominal wall will protrude forward. The palpation is used to examine the muscular limb, but for a healthy evaluation a muscle test should be performed. If there is weakness, anterior pelvic tilt, hip flexor shortening, lordosis may increase. In small children, a protrusion in the abdominal wall and a concave concussion in the lumbar region are seen. Just below the umbilicus, women have more fat mass than men.
6. Chest (thorax): a) The collapsed chest, b) Funnel type chest, c) Barrel chest, d) Pigeon chest, e) Harrison groove
• a) Collapsed Chest: It is the concave or flattened view of the front chest wall. costa, sternum, flattened and descended. It is similar to when the patient exhaled from the outside and emptied his / her breath. • In a fully collapsed chest, the elasticity of the thorax was reduced and hardened. Often, shortening of the pectoral and intercostal muscles is a factor and stretching exercises should be given to these muscles to increase their mobility. • b) Funnel Type Chest: It is usually congenital. Both the sternum and adjacent cartilage ribs were pulled inward. • c) Barrel Chest: Rounding and enlargement in thorax. The ribs and sternum were elevated as in the full inspiration. A normal thorax is not anterior, but a wide lateral diameter. On the barrel chest, expansion is observed in both diameters. This deformity is typical due to hyperventilation in asthmatics whose main problem is expiration. • d) Pigeon Chest: It is a deformity in which the anterior-posterior diameter in the thorax increases and the sternum is moved to the front. • e) Harrison Groove: It is a transverse depression in the lower thorax. Under this groove, the ribs expanded outwards. A collapse in soft tissue just below the thorax should not be confused with the Harrison groove.
7. The Shoulders: a) Height difference of both shoulders, b) Round shoulder The difference must be noticeable in order to note that one of the shoulders is lower or higher. When the muscle tension is not equal, it carries a long-term overload on one side and a shoulder in the scoliosis is higher. Scapula level should be checked for control. The patient rests his back against the wall, the shoulder levels are marked and measured by drawing the distance to the ground. The scapulas should be checked from the posterior, and the lower angles are viewed as higher or lower than each other. • Rounded shoulder; pectoral and anterior intercostal muscles are shortened and shoulders are pulled forward. If the rounded shoulder is caused by the habit, it is passively corrected because there are no hardened muscles. In the rigid round shoulder, the muscles are shortened and hardened, not passively corrected. • •
• • • 8. Head: a) lateral flexion of the head to the right and left, b) Rotation of the head to the right and left For lateral flexion, measure the distance between the right ear lobe and the upper part of the right trapezoid, the left earlobe and the upper part of the left trapeze. For rotation, the position of the jaw should be checked. 9. Arms: a) Normal transport angle at the bracket (cubital angle) b) Length difference The normal carrying angle in the elbow is 10 -15 degrees in males and 20 -25 degrees in females. Deviations from these values are recorded. The length of the arm is also measured by measuring the distance from the acromion to the tip of the third finger. 10. Waist: a) Is the concavity equal on both sides b) Is the waist level equal on both sides?
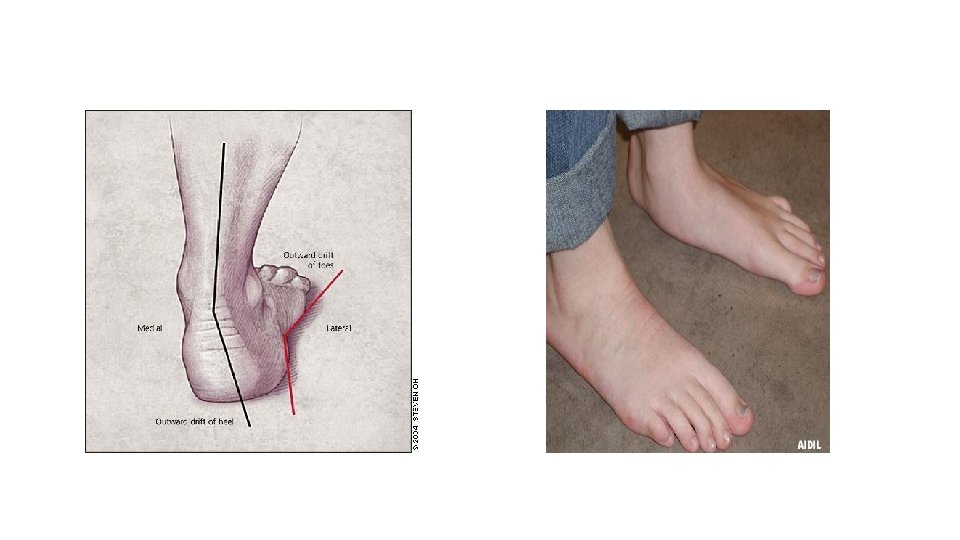
POSTERIOR POSTURE ANALYSIS • • 1. Feet: a) Calcaneal tendon displacement to inside (pronation) b) Displacement of the calcaneal tendon to outside (supination) It is better to have a slight supination in the feet. Because it saves the muscles that support the long arc from being forced. • 2. Knees: • Level of back-lines; check whether the lines in the back of the knee are equal on the right and left sides. • 3. Hips: • The level of the gluteal line; Is the bottom line of the gluteal mass at the same level on both sides • If there is a difference, one-leg shortness, scoliosis, pelvis or tilt at the base of the sacrum (lateral pelvic tilt) should be considered.
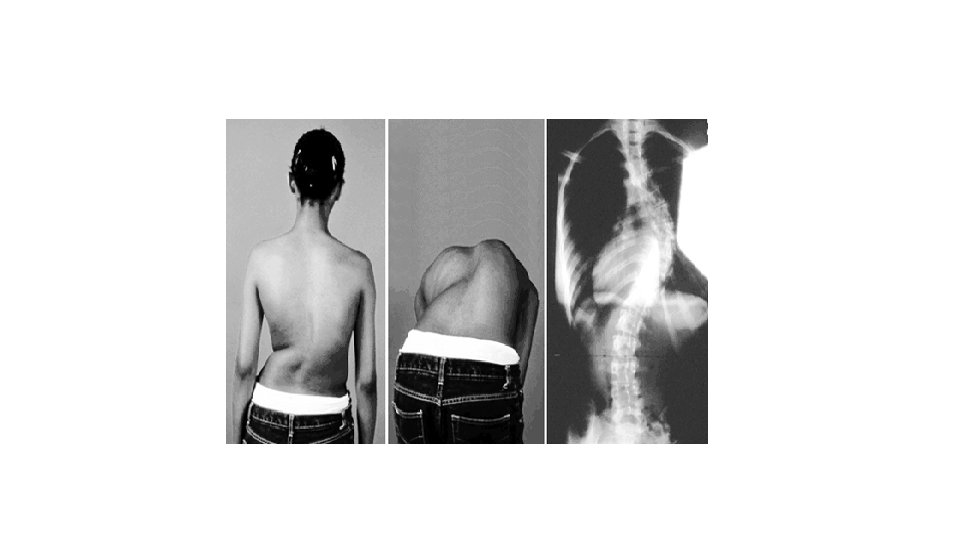
4. Columna Vertebralis: Scoliosis: It is a deformity characterized by lateral flexion of the vertebrae in the frontal plane and sagittal axis; and its rotation in the vertical axis and horizontal plane
CLASSIFICATION OF SCOLIOSIS According to the structure of scoliosis is generally examined in two groups: 1. Functional (non-structural) scoliosis: The lateral deviations in the vertebral column may have been developed or may be due to the habit to compensate for the disorder in one part of the body. Only lateral flexion is seen in the vertebrae and is not rigid. Therefore, it is seen that in some positions such as supine and prone. It is possible to correct the curvatures in vertebras by active and passive movements. Functional scoliosis is classified according to the cause: - Developed as a result of postural habits, - Depending on the length difference in the legs, - Nerve root irritations, - Compensatory mechanisms - Developing a contracture in the hip joint - inflammatory - Hysterical scoliosis
• 2. Structural Scoliosis: • Structural defects in muscle, bone, nerve and connective tissues have been developed in the area of vertebral curvature. In vertebrae, rotation with structural lateral flexion and consequent thoracic asymmetry occur. • When the corpus of vertebrae are rotating to the convex side, proc. Spinosus rotate toward the concave side. • Rotation is most common in the apex. • The bulge, which is called gibozite, is seen on the convex side in posterior and the on concave side in anterior.
• Structural scoliosis is progressive and has no reversal. Although functional scoliosis can be corrected in a short period of time, it is often not possible to achieve a definite improvement in structural scoliosis, even if all treatment modalities are best practiced. In structural scoliosis, the curvatures are (rigid). With active movement or positioning, the curvature does not improve even temporarily. • Structural scoliosis is divided into classes as a result of idiopathic, congenital, neuromuscular, disease and traumas.
• Idiopathic scoliosis: • It may be congenital or acquired later. It constitutes 65 -75% of the structural scoliosis. It is divided into three titles: • a) Infantile: It occurs between 0 and 2 -3 years of age. The prognosis is usually poor. • b) Juvenile: A less common species between 2 and 10 years of age. if it starts at a young age, the deformity becomes more severe. • c) Adolescent: It is seen over the age of 10 years. An average of half of all scoliosis is included in this group.
congenital scoliosis anomaly develops due to two disorders: 1 - Defect during vertebra formation wedge vertebra: one side of the vertebrae does not develop as partial hemi vertebra: one side of the vertebrae not completely formed 2 - Defect during the development of segments It is characterized by curvatures and structural defects in one or more segments. May be uni or bilateral.
Neuromuscular Scoliosis: Divided into two: A) Neuropathic Scoliosis: 1. Scoliosis after lower motor neuron lesions, 2. Scoliosis after upper motor lesions B) Myopathic Scoliosis: ex. scoliosis seen in muscular dystrophy. Scoliosis as a result of diseases or traumas: Rheumatic diseases, metabolic diseases, tumors, bone infections and various traumas (after fracture) are some of the scoliosis and some of these are structural scoliosis.
According to the tissues of the scoliosis: - Osteoporotic - Neuropathic - Myopathic According to the shape of the curve: - C curve - S curve Scoliosis is defined according to the vertebrae where the curve is located and the direction in which it is convex.
Depending on the number of vertebrae involved in curvature and severity: Inclinatory Scoliosis: the number of vertebrae involved in the curve is more, the angle of the curve is less Collapse Scoliosis: the number of vertebrae involved in the curve is less, the angle of the curve more According to the place of the apex: Cervical (C 1 -6) scoliosis Lumbosacral (L 5 -S 1) scoliosis
• Physical, radiological and pulmonary functions should be evaluated in scoliosis. • If the scoliosis is not rigid but is functional, the scoliosis disappears or decreases when the trunk is tilted forward. • It does not improve in structural scoliosis and there is limitation in movement. • In severe scoliosis, redness or sores on the skin occur. Pain may be due to muscle spasm. Back pain should be considered as a symptom of scoliosis (pain may be a typical symptom in severe scoliosis). • Muscle shortness tests (especially for cervical, lumbar region mobility), hip, knee, ankle limitations should be reviewed, anthropometric measurements, chest circumference measurements should be made.
• In posterior posture analysis, scoliosis is named according to vertebra and convex side. • Ex. left thoracic scoliosis (convex sides on the left and scoliosis only in the thoracic region) • The posterior pendulum should pass vertically from the midpoint of the line connecting the SIPS. • Curve C or S should be decided. If the curve is C and on the right side, right shoulder and the left hip rises. If ıt is S, same side shoulder and hip rise. • While the patient is standing, the distance between the acromion and the ground is measured. • As the patient performs anterior-flexion, the asymmetric height on the back becomes apparent.
• Ferguson method is used mostly in radiological evaluation. In this method, the exact midpoints of the top and bottom vertebrae that do not participate in the curvature are taken. The angle between them is calculated.
• In the setting of spine trauma and assessing sagittal plane deformity, the Cobb angle method is defined as the angle formed between a line drawn parallel to the superior endplate of one vertebra above the fracture and a line drawn parallel to the inferior endplate of the vertebra one level below the fracture.
The primary treatment options are bracing with exercises and surgery • Bracing- a person with scoliosis may need to use a brace if: • They’re still growing and the curvature is more than 25 to 30 degrees. • They’re still growing and the curvature is between 20 and 29 degrees, but the curvature is getting worse. • The curvature is between 20 and 29 degrees and the person has at least two more years to grow (also applies to girls who haven’t begun menstruation). • Braces won’t straighten the spine, but they can prevent the curvature from increasing. This method of treatment is more effective for cases that are detected early.
• Surgery-is usually reserved for people with curves greater than 45 or 50 degrees. • Spinal fusion is the standard scoliosis surgery. • Some of the risks of spinal fusion surgery include: • excessive bleeding • failure to heal • infection • pain • nerve damage