Neurological Emergencies Stephen Deputy MD Acute Ischemic Stroke








, urinary incontinence.")









 Location of Hemorrhage Intraventricular Hemorrhage Intraparenchymal Hemorrhage Subarachnoid Hemorrhage Subdural Hematoma")














 Aneurysmal rupture accounts for 80% of cases Risk Factors Advancing age,")












 No precipitating event, pt is neurologically and developmentally normal")
 Subarachnoid Hemorrhage Hypoxic Ischemic")



 Long-Acting AED Therapy (10 to 30")

")






 Forced Vital Capacity: (want > 15 ml/kg) Negative")




 Dropped DTR’s")
")


 Vasculitis (SLE)")



 Electrophysiology")

 Immunosupression Steroids IVIg Plasmapharesis Thymectomy")



- Slides: 80
Neurological Emergencies Stephen Deputy, MD Acute Ischemic Stroke Intracranial Hemorrhage Status Epilepticus Guillan-Barre Syndrome Acute Myelopathy Myasthenic Crisis
Acute Ischemic Stroke AIS is caused by the sudden loss of blood circulation to an area of the brain resulting in ischemia and corresponding loss of neurological function. Within seconds to minutes of loss of perfusion, an ischemic cascade is unleashed resulting in a central area of irreversible infarction surrounded by an area of potentially reversible ischemic penumbra. The goal of treatment for AIS is to preserve the area of oligemia in the ischemic penumbra. This is done by limiting the severity of injury (neuronal protection) and by restoring blood flow to the penumbra.
Acute Ischemic Stroke Ischemic Cascade Loss of O 2 and Glucose delivery to the neuron results in cellular depolarization as ATP is depleted and the Na-K ATP-as pump fails. The resulting Ca influx results in the release of many excitatory neurotransmitters including glutamate which binds to the NMDA receptor resulting in further Ca influx and further depolarization and release of glutamate. Massive Ca influx results in activation of various degrative enzymes which damage cellular membranes. The release of free radicals, arachadonic acid and nitric oxide further damage neurons.
Acute Ischemic Stroke Ischemic Cascade Within hours to days, activation of apoptotic and other genes results in the release of cytokines and further inflammatory molecules, resulting in further inflammation and microcirculatory compromise. Ultimately, the ischemic penumbra is consumed by these progressive insults, coalescing within the ischemic core, often within hours of the onset of the AIS.
Acute Ischemic Stroke Clinical Presentation No clinical feature reliably distinguishes AIS from hemorrhagic stroke, though headache, N/V, and altered mental status make hemorrhagic stroke more likely. Common symptoms of AIS include the abrupt onset of hemiparesis, monocular visual loss, ataxia, vertigo, aphasia, or sudden depressed level of consciousness. Establishing the onset of symptoms is essential when considering possible thrombolytic therapy.
Acute Ischemic Stroke Transient Ischemic Attack TIA’s are defined as a transient ischemic neurological deficit that resolves within 24 hours 80% resolve within 60 minutes TIA’s precede 30% of AIS Left untreated, 30% of TIA’s progress to AIS (20% within the first month and 50% within the first year)
Acute Ischemic Stroke Physical Examination Goal of PE is to look for extra cranial causes of AIS and to distinguish AIS from stroke mimics (seizures, tumors, toxicmetabolic disturbances, positional vertigo, etc). HEENT: Look for trauma signs and nuchal rigidity, listen for cranial or cervical bruits, evaluate pulse strength. Fundoscopy to look for emboli, hemorrhage, papilledema. C/V: Signs of CHF, Atrial fibrillation, arrhythmias. Ext: Signs of venous thrombosis and arterial emboli.
Acute Ischemic Stroke Neurological Exam Goal is to establish baseline for monitoring response to therapy and to determine size and location of AIS MS, CN, Motor, Coordination, Sensory and Gait need to be covered, however speed is of the essence! MCA: Contralateral : Hemiparesis, Hemianopsia and Sensory loss Ipsilateral: Gaze preference. Dominant Hemisphere: Aphasia Non-Dominant Hemisphere: Hemi-neglect and cortical sensory deficits
Acute Ischemic Stroke Neurological Exam ACA: Disinhibition, primitive reflexes, contralateral hemiparesis (legs>arms), urinary incontinence. PCA: Contralateral hemianopsia, cortical blindness, altered mental status, impaired memory. Vertebrobasilar: Vertigo, nystagmus, ataxia. Crossed findings (ipsilateral cranial nerve deficits along with contralateral long track signs). Lacunar Infarcts: Pure motor, pure sensory, ataxia/hemiparesis.
Acute Ischemic Stroke Work Up Labs: CBC with platelets, CMP, PTT, cardiac biomarkers, EKG. Imaging: Emergent non-contrast CT Distinguishes hemorrhagic from ischemic stroke Defines age and anatomic distribution of stroke Large hypodense area seen within 3 hours brings into question of timing of AIS and may predict poor outcome Hyperdense MCA sign, insular ribbon sign, obscuration of lentiform nucleus, loss of gray-white junction
Hyperdense MCA Sign
Large Cortical Hypodensity
Acute Ischemic Stroke Other Imaging Studies CT Angiography MRI: Diffusion-Perfusion mismatch (correlates to the core area of infarction and surrounding area of the ischemic penumbra) More sensitive than CT to early ischemic changes MR Angiography Conventional Cerebral Angiography Echocardiography: (CHF, akinetic wall, vegetation/clots, septal defects, PFO) Carotid Doppler Ultrasound: Carotid stenosis evaluation
Acute Ischemic Stroke Treatment ABCD’s Airway: Intubation for GCS < 9 or lack of airway protective reflexes Breathing: O 2 if hypoxic. Keep PCO 2 32 -36 mm. Hg Circulation: Maintain adequate CPP (MAP-ICP). Do not treat HTN unless > 200/120 D = Dextrose. Maintain normoglycemia (even if insulin is needed) as hyperglycemia worsens neurological outcome
Acute Ischemic Stroke Treatment Fever: Hyperthermia worsens ischemic injury Cerebral edema: Peaks 72 -96 hours. Hyperventilation can decrease CPP. Mannitol may leak across compromised BBB. No evidence of benefit for steroids. Decompressive craniectomy and resection of necrotic tissue may be indicated, especially in the setting of hemorrhagic transformation. Seizure control: Prophylactic AED is not indicated unless malignant elevated ICP is present
Acute Ischemic Stroke Acute Thrombolysis Balance restoration of blood flow and hemorrhage risk No evidence of hemorrhage on CT Hypodensity on CT < 1/3 of hemisphere Onset of symptoms within 3 hours of r. TPA use SBP < 185 DBP < 110 INR < 1. 7, Platelets > 100, 000, No ASA or anticoagulation, No trauma or recent surgery r. TPA: 0. 9 mg/kg IV over 60 minutes with 10% of dose given over the 1 st minute
Acute Ischemic Stroke Strategies for Reducing Future Strokes Anti-Platelet Therapy Warfarin: (Atrial Fibrillation, Arterial Dissection) Carotid Endarterctomy / Stent Placement PFO Closure Reducing Stroke Risk Factors (Hypercholesterolemia, Hypertension, Diabetes, Obesity, Lack of Exercise, Smoking, OCP’s)
Intracranial Hemorrhage (non-traumatic) Location of Hemorrhage Intraventricular Hemorrhage Intraparenchymal Hemorrhage Subarachnoid Hemorrhage Subdural Hematoma Epidural Hematoma
Intracranial Hemorrhage Intraventricular Hemorrhage Accounts for 3% of all non-traumatic ICH Hypertension is the most common etiology Often results from an intraparenchymal hemorrhage that extends into the ventricular system S/S: Headache, N/V, Progressive deterioration of consciousness, raised ICP, Nuchal rigidity Survivors may develop post-hemorrhagic hydrocephalus
Intracranial Hemorrhage Intraparenchymal Hemorrhage Basal Ganglia Hemorrhage Contralateral hemiparesis, hemichorea, hemisensory loss, and hemi -neglect are common neurological deficits Putaminal Hemorrhage is the most common location of intraparenchymal hemorrhage secondary to HTN Putaminal Hemorrhage, if massive, will result in Uncal Herniation (Ipsilateral blown pupil, contralateral hemiparesis, depressed LOC Caudate Hemorrhage is most likely to rupture into ventricles
Basal Ganglia Intraparenchymal Hemorrhage
Intracranial Hemorrhage Intraparenchymal Hemorrhage Thalamic Hemorrhage Contralateral hemiparesis, hemisensory loss and depressed LOC (wake center) are common deficits Extension into ventricular system common resulting in obstructive hydrocephalus with 3 rd ventricular enlargement => Parinaud’s Syndrome (Paralysis of voluntary upward gaze, light-near dissociation, convergence-retraction nystagmus, eyelid retraction)
Thalamic Intraparenchymal Hemorrhage
Intracranial Hemorrhage Intraparenchymal Hemorrhage Pontine Hemorrhage Abrupt onset of coma, pinpoint pupils, autonomic instability, horizontal gaze paralysis, and quadriparesis The miotic pupils and depressed LOC may mimic opiate overdose
Pontine Intraparenchymal Hemorrhage
Intracranial Hemorrhage Cerebellar Hemorrhage Sudden onset of vertigo, severe N/V, and ataxia leading to altered mental status and coma over a few hours Obstructive hydrocephalus can contribute to brainstem herniation Urgent posterior fossa decompression is essential for survival
Intraparenchymal Cerebellar Hemorrhage
Intracranial Hemorrhage Lobar Intraparenchymal Hemorrhage This is often a clinically silent lesion S/S depend on location of hemorrhage, though hemiparesis, aphasia, hemianopsia, and hemisensory loss common Mimics lobar AIS
Lobar Intraparenchymal Hemorrhage
Intraparenchymal Hemorrhage Etiology Hypertension is the #1 cause in adults Hyalinization of small penetrating arteries (replacement of smooth muscle by collagen => increased friability of vessels Cerebral Amyloid Angiopathy Elderly with dementia and multiple bleeds Anticoagulation and Anti-Platelet Meds Systemic anticoagulated states (eg. DIC) Sympathomimetic Drugs Aneurysms, AVM’s, Cavernous Angiomas Brain Tumors Metastatic (renal cell CA, malignant melanoma, prostate, and lung CA) GBM and Hemangioblastoma
Intraparenchymal Hemorrhage Treatment ABCD’s Intubation Treat Hypertension to keep SBP < 160 mm. Hg Fluid and Electrolyte Management Use Normal Saline, avoid Dextrose Watch for SIADH and Cerebral Salt Wasting Prevent Hyperthermia Seizure Prophylaxis Correct Underlying Coagulopathy FFP, platelet Infusions, Vitamin K
Intraparenchymal Hemorrhage Treatment Recombinant Factor VII Dosing ranges between 40 and 160 micrograms Beneficial if given within 4 hours of onset Risk of myocardial infarction and AIS Management of ICP Hyperventilate to keep Pa. CO 2 around 30 mm. Hg Avoid Mannitol (can leak into hematoma) External Ventricular Drain (if hydrocep 0 halus present) Surgical Evacuation of Hematoma (controversial)
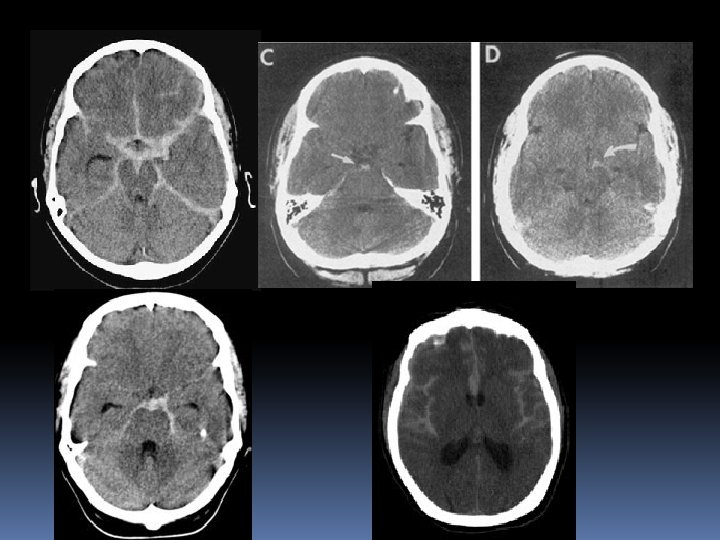
Subarachnoid Hemorrhage (non-traumatic) Aneurysmal rupture accounts for 80% of cases Risk Factors Advancing age, Smoking, HTN, Cocaine use, Hypertension, Heavy Alcohol use, Connective Tissue Disorders, Sickle Cell Disease, First Degree Relatives with Aneurysms Fatality rate is 50% within 2 weeks 30% of survivors require lifelong care 15% of patients will have > 1 aneurysm Outcome largely dependent on clinical presentation and CT findings
Subarachnoid Hemorrhage
Subarachnoid Hemorrhage Clinical presenting signs Sudden-Onset “Thunderclap Headache” “Worst Headache of my life” CN III palsy (p. comm aneurysm) CN VI palsy (raised ICP) Retinal Hemorrhages Altered Mental Status Nuchal Rigidity
Subarachnoid Hemorrhage Diagnostic Work Up CT Imaging Will pick up > 90% SAH (get thin cuts through skull base) Sensitivity drops to < 50% after 2 weeks Carefully evaluate basilar cisterns for hemorrhage
Subarachnoid Hemorrhage Diagnostic Work Up Lumbar Puncture Perform if high index of suspicion and negative CT Elevated Opening Pressure Increased RBC count that does not “clear” between tubes one and tube four Xanthochromia (rule of 2’s) Starts at 2 hours, Peaks at 2 days, Clears by 2 weeks
Subarachnoid Hemorrhage Diagnostic Work Up Angiography Digital Subtraction Angiography is gold standard CT Angiography MR Angiography Look for Multiple Aneurysms
Conventional Angiogram
CT Angiogram
MR Angiogram
Subarachnoid Hemorrhage Treatment General Measures ABCD’s Intubation for GCS < 9 Treat HTN: SBP 90 -140 prior to aneurysm treatment, < 200 mm. Hg after Rx Glucose between 80 and 120 mg/dl Euvolemia (CVP 5 -8 mm. Hg unless vasospasm, then CVP 8 -12 mm. Hg) Temperature Quiet Room / Sedation GI (H 2 blocker, stool softener, NPO) Vasospasm Nimodipine 60 mg po q 4 hrs for 21 days Seizures (Phenobarbital or Lorazepam)
Subarachnoid Hemorrhage Treating the Aneurysm Surgical Intervention Endovascular Coiling
Status Epilepticus Definitions A single seizure or back-to-back seizures without return of consciousness lasting > 45 minutes (primate studies) >30 minutes (WHO definition) >10 minutes (working definition)
Status Epilepticus Epidemiology 10% of all individuals with epilepsy will have at least one episode of SE in their lifetime 10% of patients experiencing a first unprovoked seizure will present in SE Risk of recurrent SE: Greatest for those with remote symptomatic etiologies Not any higher in those with idiopathic or febrile etiologies
Status Epilepticus Etiologies Idiopathic (24%) No precipitating event, pt is neurologically and developmentally normal Febrile (24%) Includes “febrile seizures” and seizures in the setting of a febrile illness Remote Symptomatic (23%) Prior neurological insult or developmental brain malformation Acute symptomatic (23%) Progressive Degenerative (6%)
Status Epilepticus Acute Symptomatic Etiologies Vascular Stroke (Hemorrhagic > Ischemic) Subarachnoid Hemorrhage Hypoxic Ischemic Encephalopathy Toxic Cocaine and other sympathomimetics Alcohol withdrawal Various Medications (Isoniazid, TCA’s, various chemotherapy agents) AED non-compliance or withdrawal
Status Epilepticus Acute Symptomatic Etiologies Metabolic Hyper or Hypo-Natremia Hypoglycemia Hypocalcemia Liver or Renal failure Infectious Meningoencephalitis Brain Abscess Trauma Neoplastic
Status Epilepticus Treatment ABCD’s Airway: Risk of aspiration, suction to bedside Breathing: Give supplemental O 2 C/V: Initial tachycardia giving way to hypotension (especially when Benzos or Barbiturates are given) Dextrose: Symptomatic hypoglycemia is causing irreversible brain injury until corrected
Status Epilepticus History Fever, pre-existing epilepsy, trauma, baseline AED’s and their dosing Physical Exam Signs of trauma, nuchal rigidity, end organ injury Subtle signs of seizures (tachycardia, pupil dilation and hippus, nystagmus, irregular respirations) Work Up Lytes, glucose, AED levels, CPK, LFT’s, ABG, NH 3 CT of brain LP (when stable) if indicated. Empiric antibiotics.
Status Epilepticus Anticonvulsant Therapy Benzodiazepine Therapy (10 minutes) Long-Acting AED Therapy (10 to 30 minutes) Refractory Status Therapy (>30 minutes)
Status Epilepticus Benzodiazepine Therapy Lorazepam 0. 1 mg/kg max: 4 mg/dose Has 8 hour effective t½ Diazepam 0. 3 to 0. 5 mg/kg max: 10 mg/dose Fat-soluble so pr dosing possible Diastat (Dosing about double that of IV)
Status Epilepticus Long-Acting Anticonvulsant Therapy Phenytoin 20 mg/kg over 20 minutes (regardless of weight) C/R monitor during load No dextrose in line Extravasation injuries are severe Cerebyx 20 mg. PE/kg over 8 minutes No precipitation in dextrose Less severe extravasation injury (more neutral p. H)
Status Epilepticus Long-Acting Anticonvulsant Therapy Phenobarbital 20 mg/kg over 20 minutes Watch for respiratory suppression (especially if the patient has received Benzodiazepines) Watch for hypotension Good for Febrile Status Epilepticus
Status Epilepticus Refractory Status Secure airway Transfer to ICU Extra lines for hypotension treatment EEG Monitoring (electrical-clinical dissociation) Medications Pentobarbital Other agents (Midazolam drip, Propofol, Lidocaine, inhalation anesthetics, other AED’s)
Guillan-Barre´Syndrome Definition Progressive ascending weakness along with various cranial neuropathies Areflexia Minimal sensory deficits (though radicular pain is common) Progression over days to 4 weeks Preceding infection or Immunization: 1 to 4 weeks prior to onset of weakness (C. jejuni, CMV, Mycoplasma, d. T, OPV, VZV)
Guillan-Barre´Syndrome GBS Variants Acute Inflammatory Demyelinating Polyneuropathy Acute Motor Axonal Neuropathy Acute Motor Sensory Axonal Neuropathy Miller Fisher Syndrome Chronic Inflammatory Demyelinating Polyneuropathy (> 4 weeks of progression or future relapses)
Guillan-Barre´Syndrome Physical Exam Look for the Tick! Bulbar and Respiratory Compromise Relatively Symmetric Ascending Weakness Diminished/Absent DTR’s No Sensory Level Radicular Pain/Paresthesias Autonomic Dysfunction: Increased or Decreased SNS or PNS Function (tachy-brady arrhythmias, hyper/hypotension, urinary retention, decreased GI mobility)
Guillan-Barre´Syndrome Laboratory Support CSF: Albuminocytological Dissociation Elevated Protein without Pleocytosis Nerve Conduction: Multifocal, asymmetrical demyelination with secondary axonal degeneration Slowing of Nerve Conduction Velocities Temporal Dispersion and Conduction Block
Guillan-Barre´Syndrome Treatment ABC’s Airway/Breathing: (Serial Examinations) Forced Vital Capacity: (want > 15 ml/kg) Negative Inspiratory Force (want > - 40 mm. Hg) ABG’s : Look for rising Pa CO 2 Clinical Exam (accessory muscles, SOB, diminished exhalation strength) Elective Intubation if Respiratory Insufficiency or significant Bulbar Weakness
Guillan-Barre´Syndrome Treatment ABC’s Cardiovascular C/R and BP Monitoring Careful when treating hypo or hypertension Excessive Vagal Response with GI pain, Intubation, Tracheal Suctioning and other Procedures ICU Monitoring Until Patient Reaches Nadir of Weakness
Guillan-Barre´Syndrome Treatment IVIG 5 day infusion of 0. 4 g/kg per day Plasmapharesis 5 exchanges (40 -50 ml/kg) given on alternate days using saline and albumin as replacement fluid No Role for Steroids
Guillan-Barre´Syndrome Outcome 10% to 20% require mechanical ventilation Mortality 2% to 5% After nadir, plateau phase lasts 2 -4 weeks 70% complete recovery within 1 yr, 82% by 2 yrs 3% will go on to have relapse (CIDP)
Acute Myelopathy Clinical Findings The spinal cord contains closely approximated ascending and descending tracts that will result in multiple deficits in the setting of injury. Some of the more clinically important tracts include: Descending Corticospinal Tract Ascending Spinothalamic Tract Ascending Posterior Columns Descending Autonomic Nervous System
Acute Myelopathy Clinical Deficits Acute Flaccid Paralysis (Ipsilateral to side of lesion) Dropped DTR’s below the level of the lesion Anterior Horn Cell dysfunction at the level of the lesion Distinguish from dropped DTR’s due to GBS Plantar Responses will be Extensor Superficial Reflexes absent below the level of the lesion Superficial Abdominal Reflex Cremaster Reflex Bulbocavernosus Reflex
Acute Myelopathy Clinical Deficits Sensory Level Pain and Temperature (Contralateral to side of lesion) Spinothalamic Tract Vibration and Joint Position Sense (Ipsilateral) Posterior Columns
Acute Myelopathy Clinical Deficits Autonomic Nervous System Horner’s Sign Ptosis, Meiosis, Anhydrosis Ipsilateral Descending SNS (C 1 -T 2) Bladder Dysfunction Sphincter Dysynergy Spastic Bladder with Incontinence Bowel Dysfunction Constipation or Incontinence Diminished Rectal Tone
Acute Myelopathy Etiologies Trauma High-Dose Methylprednisolone Protocol Spontaneous Epidural or Subdural Hematoma Neoplastic Metastatic or Primary Tumors Vascular Ischemia (Aortic Surgery, Hypotension, Spinal Surgery) Hemorrhagic (Vascular Malformations, Coagulopathy)
Acute Myelopathy Etiologies Demyelinating Transverse Myelitis (Isolated or as part of MS) Vasculitis (SLE) Infectious Epidural/Subdural Abscess Osteomyelitis/Discitis
Acute Myelopathy Etiologies Acute Myelopathy should be considered to be caused by a mass lesion compressing the cord until proven otherwise! Emergent Imaging is warranted MRI of Spine is preferred CT Myelogram is second choice Emergent Neurosurgical Consultation Time is of the essence!
Myasthenic Crisis MG is an auto-immune disorder characterized by a humoral-mediated immune attack on Acetylcholine receptors on skeletal muscle
Myasthenic Crisis Clinical Features Opthalmoparesis and Ptosis Bulbar Weakness Respiratory Muscle Weakness Key Point: Weakness is Fatigable Progressive Weakness with Repetitive Testing
Myasthenic Crisis Diagnosis Clinical Fatigable weakness Preserved DTR’s Tensilon Test (Acetylcholine Esterase Inhibitor) Electrophysiology Decremental CMAP amplitudes with repetitive stim. Lab Acetylcholine Receptor Antibodies
Myasthenic Crisis
Myasthenic Crisis Treatment of MG Acetylcholine Esterase Inhibitors (Mestinon) Immunosupression Steroids IVIg Plasmapharesis Thymectomy
Myasthenic Crisis Treatment of Myasthenic Crisis ABC’s Secure the airway with intubation if there is any doubt Look for and Rx any underlying infection Remove medications which can exacerbate MG Gentamycin, steroids, anticholinergics Never increase Mestinon to try and get out of a myasthenic crisis It may be reasonable to D/C or lower Mestinon if one cannot exclude a cholinergic crisis (SLUDGE)
Myasthenic Crisis Treatment of Myasthenic Crisis High dose Methylprednisolone IVIg Plasmapharesis
Clinical Neurosciences Clerkship Now you are ready to go out there and confidently handle patients presenting with these various Neurological Emergencies!