Intravenous thrombolysis of acute ischemic stroke 2016 08

Intravenous thrombolysis of acute ischemic stroke 陳龍 臺北醫學大學-部立雙和醫院神經科 2016. 08. 14 1

2

TIME IS BRAIN 3 Lancet 2010


後續照顧 • • • 24小時內禁用heparin, coumadin, antiplatelet agents Complete bed rest for 24 hours Avoid folley Avoid A-line Avoid N-G Monitor V/S Q 15 min for 2 hours; Q 30 min for 6 hours; then Q 1 H for 16 hours • Record NE & NIHSS 2 hours and 24 hours after Tx

BRAIN IMAGE • Routine Brain CT/MRI 24 hours after Tx • Emergent image study: • NIHSS increase >4 • Highly suspect of ICH—同時check CBC/DC, PT/a. PTT, 準備 4 U PRBC, or 6 U cryoprecipitate, 2 -4 U FFP, and 12 U platelet,並知會NS

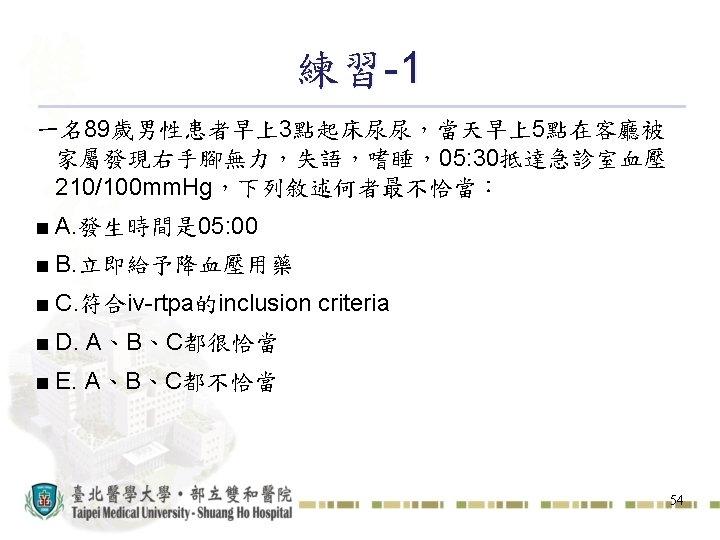
Initial Management-Conclusions • • BP-220/130 mm. Hg observation BP-below 180/105 mm. Hg for iv r-t. PA Prevent fever 血糖每增加 100 mg/dl時,復原機會減少 24%,出血性腦梗塞 24% 的機會也會增加,且容易引發電解質不平衡及其他的併發症 • 腦中風病人血糖在 200 mg/dl以上時,可以重覆注射低劑量的 以上 Insulin將血糖控制在 150 mg/dl以內。 • iv hydration with normal saline • IICP • Head elevation 30 • Osmotic agent • Hyperventilation with ET intubation- Pa. CO 2降低5 -10 mm Hg 可降低25 -30%的顱內壓 • Decompressive craniectomy • 3% normal saline

28

29

30

31

32

The evidence indicates that intravenous rt-PA increased the proportion of patients who were alive with favourable outcome and alive and independent at final follow-up. The data strengthen previous evidence to treat patients as early as possible after acute ischaemic stroke, although some patients might benefit up to 6 h after stroke. LANCET 2012 33
-Stroke 2000")
For Better Outcome ■ m. RS 0 -1 ✓OR 1. 3 (p=0. 56)-Stroke 2000 ✓ 44% vs 32% (p=0. 18)-ACTA Scand 2012 ■ m. RS 0 -2 ✓ 40% vs 25. 9% (p=0. 0001)-JNNP 2006 ✓OR 0. 49 in 80+y/o -JNNP 2010 ✓ 90+y/o 9%-Mayo 2010 ✓Thrombolysis vs non=20% vs 17. 1% (p=0. 75)-Eur Neurol 2011 34
-Stroke 2000")
For ICH ■ 80 - vs 80+ ✓ 9% vs 7% (p=0. 99)-Stroke 2000 ✓ 10. 8% vs 14. 4% (p=0. 1)-JNNP 2006 ✓ 5. 1% vs 4. 3% (p=0. 33)-Age 2012 ✓ 0% vs 5. 2% (p=0. 09)-ACTA Scand 2012 ■ 14% in 80+ -Mayo 2010 ■ 80+ increase 2. 87 x -AJEM 2010 ■ OR 1. 31 -JNNP 2010 • Thrombolysis vs non=16. 7% vs 2. 4% (p=0. 08) -Eur Neurol 2011 35
-Stroke 2000")
For Mortality ■ 80 - vs 80+ ✓ 8% vs 20% (p=0. 04)-Stroke 2000 ✓ 18. 2% vs 35. 3% (p=0. 001)-JNNP 2006 ✓ 36. 1% vs 70. 6% (p=0. 005)-Age 2012 ✓ 10% vs 18% (p=0. 17)-ACTA Scand 2012 ■ 80+ OR 2. 77 -JNNP 2010 ■ 81 -90 y/o OR 1. 34; 90+ OR 2. 7 • Thrombolysis vs non=3. 3% vs 7. 3% (p=0. 63) -Eur Neurol 2011 36

Effect of rt-PA on alive and independent at the end of follow-up, subgrouped by age and time to treatment 40
 3: 00 3 -4:")
Extending the time-window All Studies ECASS III (RCT 3 b) 3: 00 3 -4: 30 h SITS-MOST (PMS 4) <3 h ECASS 2 4: 30

45

46

Distribution of Scores on the m. RS 47

48


Patients presenting with acute stroke while on NOACs Acute haemorrhagic stroke Discontinue NOACs. Limited data to support use of a specific procoagulants e. g. PCC, a. PCC and a. FVII. Use PCC or fresh frozen plasma as discussed in slides about measures in case of major bleeding. Same poor prognosis as for warfarin. 1 1. Hart et al. Stroke 2012; 43: 1511 -7 www. escardio. org/EHRA 54

Patients presenting with acute stroke while on NOACs Acute ischaemic stroke Assess the time window since last intake of NOAC: thrombolytic therapy is associated with increased bleeding risk within 48 h of last NOAC dose. In case of uncertainty regarding last dose, prolonged a. PTT (dabigatran) or PT (FXa inhibitors) indicates that thrombolysis should not be given. If NOACs have been given within 48 h and coagulation tests not available or abnormal, consider recanalization of occluded vessels. www. escardio. org/EHRA 55
- Slides: 60