Week 2 outline Pharmacokinetics How drugs are handled



 how a drug is broken down or made into")

 and triazolam (Halcion) – pharmacokinetics � lorazepam – persists for at")










 – antianxiety drug")







 ◦ ◦ ◦ Intravenous Intramuscular Subcutaneous Intracranial Epidural Intraperitoneal")




 , nicotine")









![Concentration Gradient Drug goes from higher concentration to lower concentration [DRUG] receptors ≈ [DRUG]](https://slidetodoc.com/presentation_image/aa31c04e68a24f5aa0a496ff5b7bbe83/image-50.jpg "Concentration Gradient Drug goes from higher concentration to lower concentration [DRUG] receptors ≈ [DRUG]")










 chemical transformation of a drug into a")



 by 1. deactivating the molecule 2. ionize")


 stimulates a receptor")














")




- Slides: 96
Week 2 outline � Pharmacokinetics: ◦ How drugs are handled by the body ◦ Overview followed by details!!
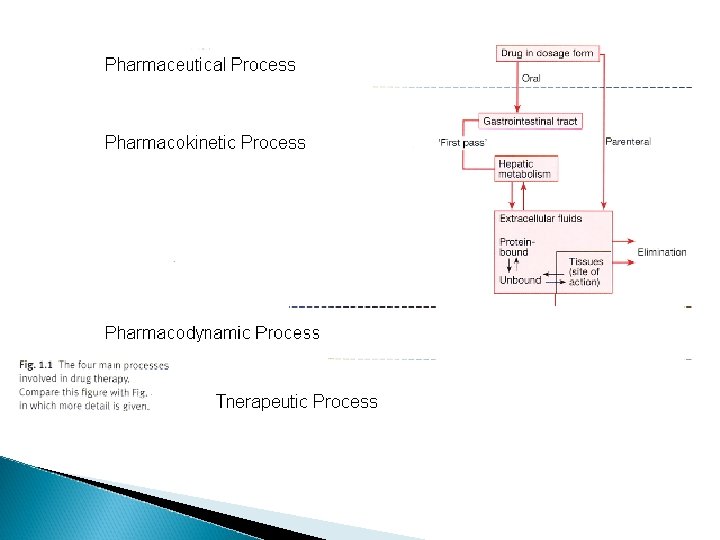
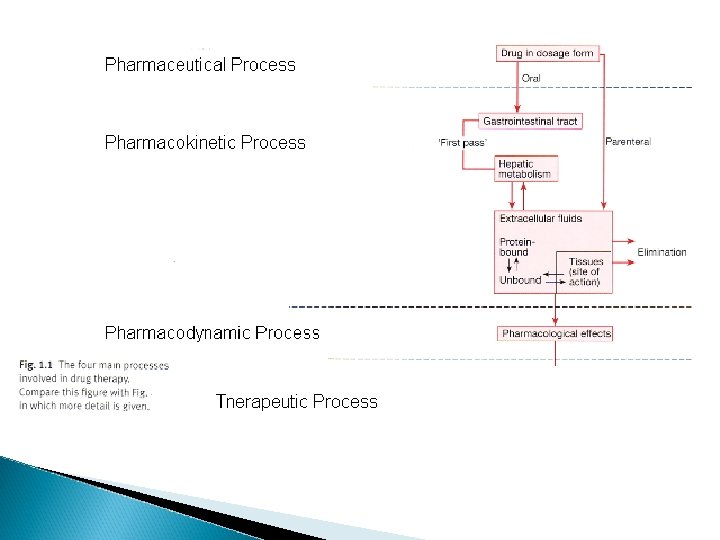
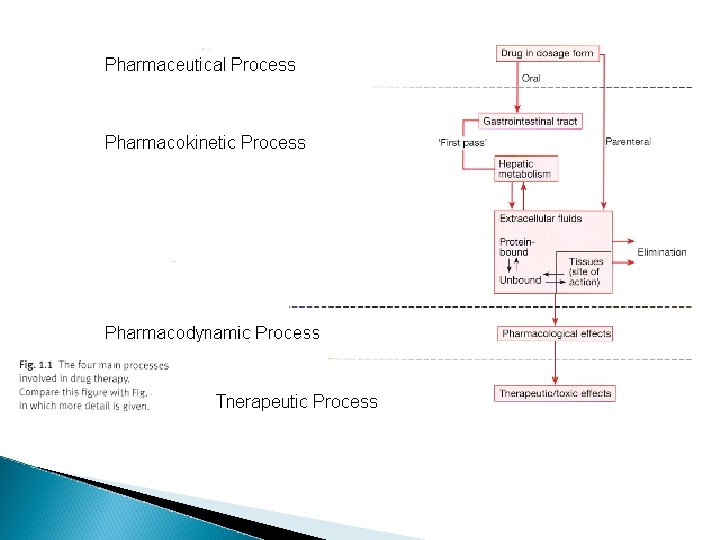
Lets say you have a really bad headache or an infection of some kind that needs antibiotics and you have to take some meds – This illustrates the basic processes in the branch of pharmacokinetics
pharmacokinetics. . . . 1. 2. the route of administration - how a drug is taken into the body absorption and distribution - factors affecting its absorption and how it gets distributed to the brain
3. metabolism (detoxification or breakdown) how a drug is broken down or made into inactive forms 4. excretion – (elimination) ◦ how the drug is eliminated
Knowing about pharmacokinetics tells us critical information about insight into the actions of a drug. Ex. benzodiazepenes ultra short acting, long acting
� lorazepam (Ativan) and triazolam (Halcion) – pharmacokinetics � lorazepam – persists for at least 24 hr � triazolam – 6 – 8 hours � midazolam – 1 – 2 hrs
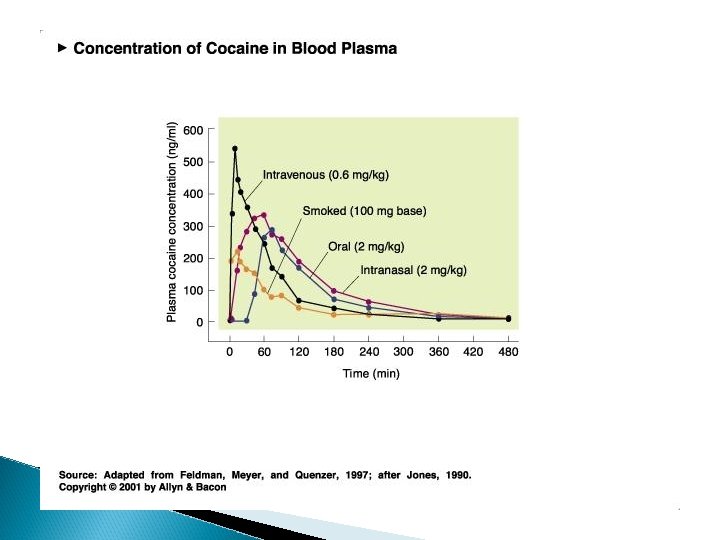
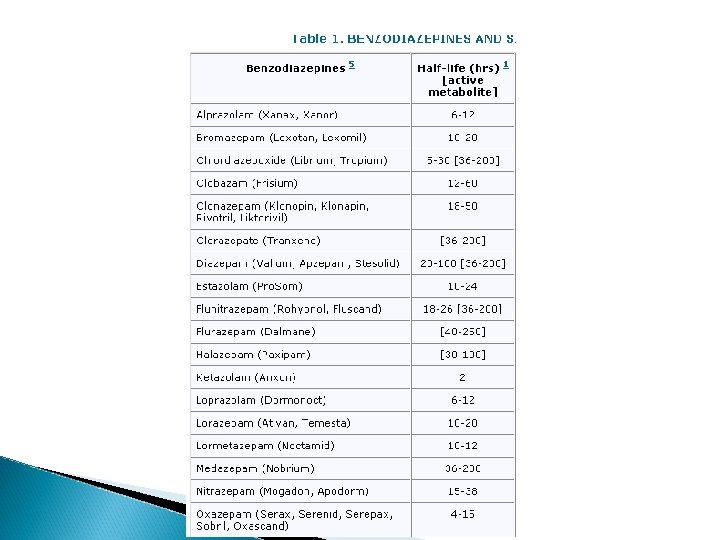
What are the routes of drug administration? � Oral � Parenteral � Buccal � Inhalation � Rectal � Nasal
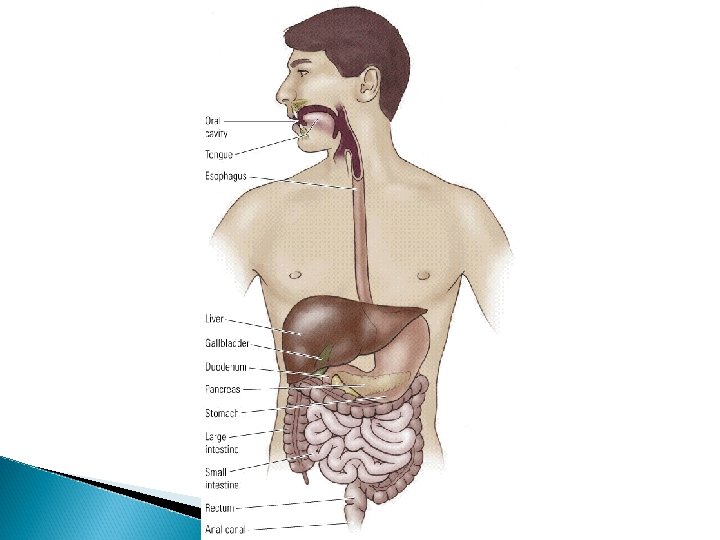
oral administration � most common, sometimes referred to as po � safe, self administered, economical BUT blood levels are often irregular (most complicated route of adm) � liquid more readily absorbed than solids
What are the qualities a drug needs to be absorbed orally? � soluble and stable in stomach (not destroyed by stomach enzymes more acidic) � enter intestine; penetrate lining of intestine, pass into bloodstream and reach site of action; intestine is more basic � absorption favored if the drug is nonionized and more lipophilic
What do orally administered drugs have to deal with? ◦ chemicals in stomach must deal with: ◦ stomach acids ◦ digestive enzymes ◦ first pass metabolism through liver ◦ other items in stomach �ex. tetracycline
� Find something about warning label for tetracycline and absorption
Advantages of oral administration ◦ Convenient - can be self- administered, pain free, easy to take ◦ Absorption - takes place along the whole length of the GI tract ◦ Inexpensive - compared to most other parenteral routes
oral administration � disadvantages ◦ ◦ ◦ of oral administration: vomiting/stomach distress variability in dose effect too slow for emergencies unpleasant taste of some drugs unable to use in unconscious patient first pass metabolism
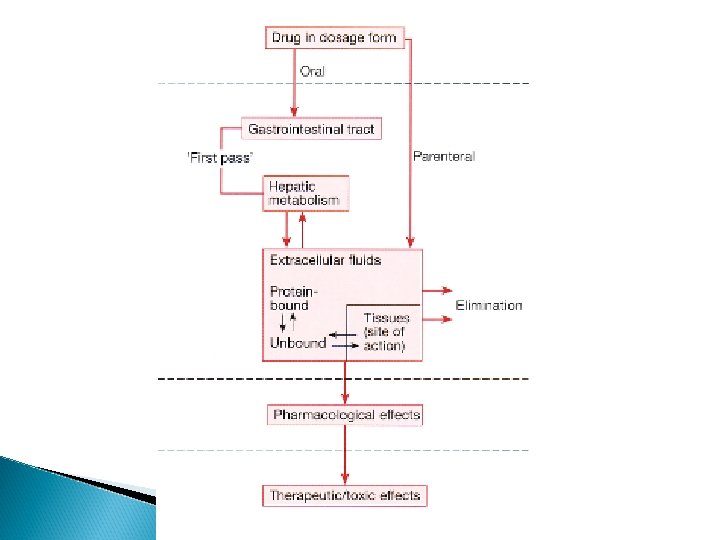
First-pass metabolism � First pass metabolism - term used for the hepatic metabolism of a drug when it is absorbed from the gut and delivered to the liver via the portal circulation. � The greater the first-pass effect, the less the agent will reach the systemic circulation when the agent is administered orally
first pass metabolism
oral administration � disadvantages ◦ ◦ of oral administration: vomiting stomach distress variability in dose first pass metabolism �ex. buspirone (Bu. Spar) – antianxiety drug � 5% reaches central circulation and is distributed to brain
oral administration � disadvantages of oral administration: �ex. buspirone (Bu. Spar) – antianxiety drug � 5% reaches central circulation and is distributed to brain �metabolism can be blocked by drinking grapefruit juice (suppresses CYPp 450 enzyme)
Grapefruit Juice Increases Felodipine Oral Availability in Humans by Decreasing Intestinal CYP 3 A Protein Expression Hours J. Clin. Invest. 99: 10, p. 2545 -53, 1997
Some additional interesting points regarding oral adm � Drugs that are destroyed by gastric juice or cause gastric irritation can be administered in a coating that prevents dissolution in acidic gastric contents (however may also preclude dissolving in intestines) � Controlled – Release Preps -
Controlled release � Sustained Release � Controlled Release � Extended Release � Time or Timed Release � How is this achieved? ◦ Embed in a web of substance that the body is slow to dissolve ◦ drug to swell up to form a gel with a nearly impenetrable surface, wherein the drug slowly exits the semipermeable layer ◦ may have a coating over the active ingredient, ◦ may contain tiny time release beads, individually coated
Some abbreviations……. � DA: delayed absorption DR: delayed release EC: enteric coated ER: enteric release GC: granules within capsules SR: slow release SSR: sustained release
Factors that affect rate of absorption following PO route � GI motility- speed of gastric emptying affects rate of absorption ◦ ex. migraine and analgesics vs metoclopramide � Malabsorptive States - ◦ GI diseases, ex. Crohn’s disease can affect absorption
Factors that affect rate of absorption following PO route � Food - ◦ iron, milk alters tetracycline ◦ fats � first pass metabolism
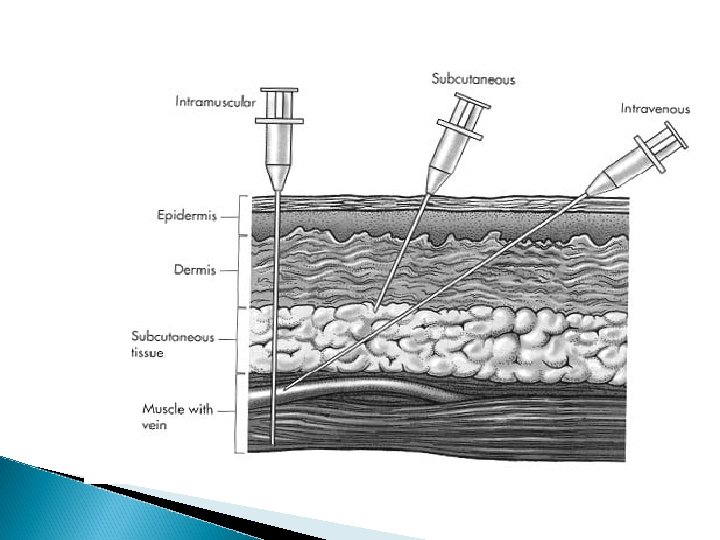
Parenteral or Injection � chemicals needle; delivered with a hypodermic ◦ most commonly - injected into vein, muscle or under the upper layers of skin, in rodents also intraperitoneal cavity � requirements for parenteral: �must be soluble in solution (so it can be injected)
B. Parenteral (Injection) ◦ ◦ ◦ Intravenous Intramuscular Subcutaneous Intracranial Epidural Intraperitoneal
Intramuscular � absorption more rapid than SC ◦ less chance of irritation; � ways to speed up or slow down absorption � depot injections -
Intravenous � extremely rapid rate of absorption � adv: useful when you need rapid response or for irritating substances � Disadv: rapid rate of absorption
Absorption for parenteral route �contingent on blood flow SO ◦ IV, intraperitoneal, IM, SC �increasing or decreasing blood flow affects drug absorption �Drugs leave bloodstream and are exchanged between blood capillaries and body tissues
What if a drug is injected in oil? � bolus or depot shots � related - drugs that accumulate in fat ◦ ex. THC
Mucosal membranes � nasal, oral, buccal � medications include: nitroglycerine, fentanyl –(1998) , nicotine gum, lozenges, buprenorphine � cocaine � snuff, – cigars
Advantages and Disadvantages of Buccal ◦ Advantages: �rapid absorption �avoid first-pass effect ◦ Disadvantages: �inconvenient �small doses �unpleasant taste of some drugs
transdermal or transcutaneous � 1990’s – several medications incorporated into transdermal patches: ◦ estrogen, nicotine, fentanyl, nitroglycerin, scopolamine � controlled of time � Novel slow release for extended periods approaches…. . Audra Stinchcomb
Rectal Administration � usually suppository form � for unconscious, vomiting or unable to swallow � disadv: not very well regulated dose; absorbed plus irritation (yikes)
Inhalation � not really used for psychotropics
Route for administration -Time until effect�intravenous 30 -60 seconds �inhalation 2 -3 minutes �sublingual 3 -5 minutes �intramuscular 10 -20 minutes �subcutaneous 15 -30 minutes �rectal 5 -30 minutes �ingestion 30 -90 minutes �transdermal (topical) variable (minutes to hours)
Drug Absorption � The rate at which a drug reaches it site of action depends on: ◦ Absorption - involves the passage of the drug from its site of administration into the blood ◦ Distribution - involves the delivery of the drug to the tissues
Drug Absorption � Factors which influence the rate of absorption ◦ ◦ routes of administration dosage forms the physicochemical properties of the drug protein binding
Drug Absorption � Factors which influence the rate of absorption ◦ ◦ ◦ routes of administration dosage forms the physicochemical properties of the drug protein binding circulation at the site of absorption concentration of the drug
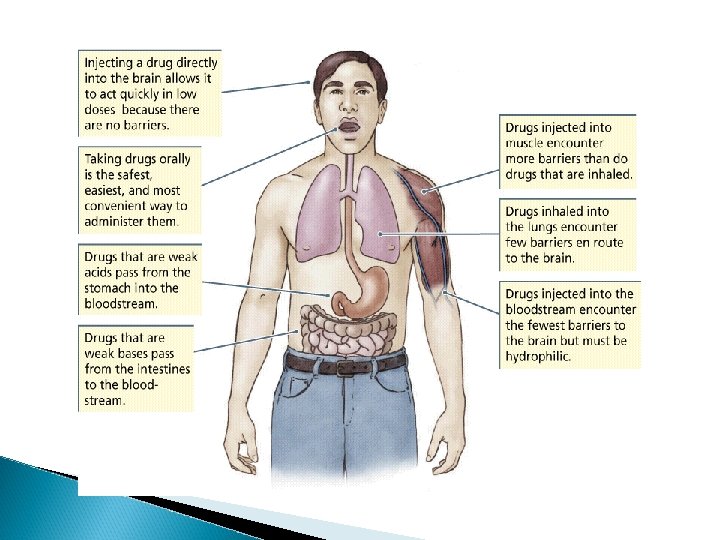
Absorption � Mostly a passive process - ◦ from higher conc to lower (in blood)
Concentration Gradient Drug goes from higher concentration to lower concentration [DRUG] receptors ≈ [DRUG] circulation
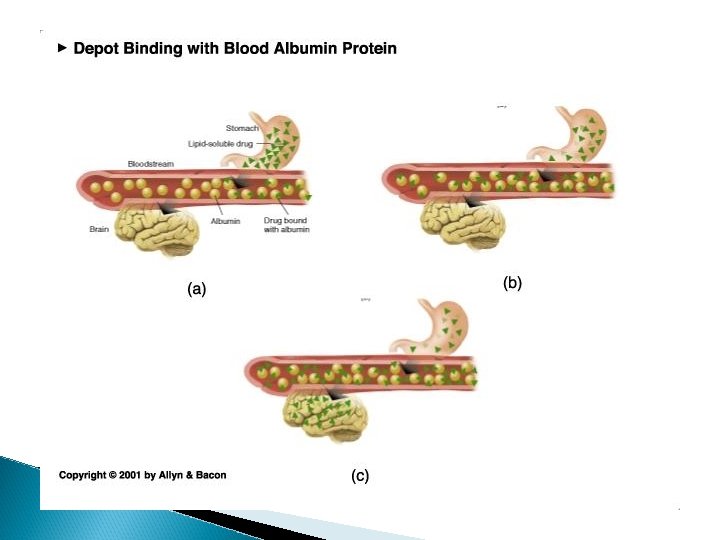
Pharmacokinetics � Distribution Drug molecules may be found in different places in the blood. 1. Plasma–more likely with water soluble drugs 2. Platelets–more likely with lipid soluble drugs 3. Attached to proteins (e. g. , albumin)–bound vs. free
Absorption and Distribution � Mostly a passive process - ◦ from higher conc to lower (in blood) � Binding to plasma proteins ◦ results in a store of bound drug in plasma �examples - � 95 -99% - chlorpromazine, diazepam, imipramine � 90 - 95% - valproate, propanolol, phenytoin
Factors that can play a role in reducing the amount of drug bound to proteins � Renal insufficiency � last trimester of pregnancy � drug interactions (other drugs that bind to proteins) � diseases
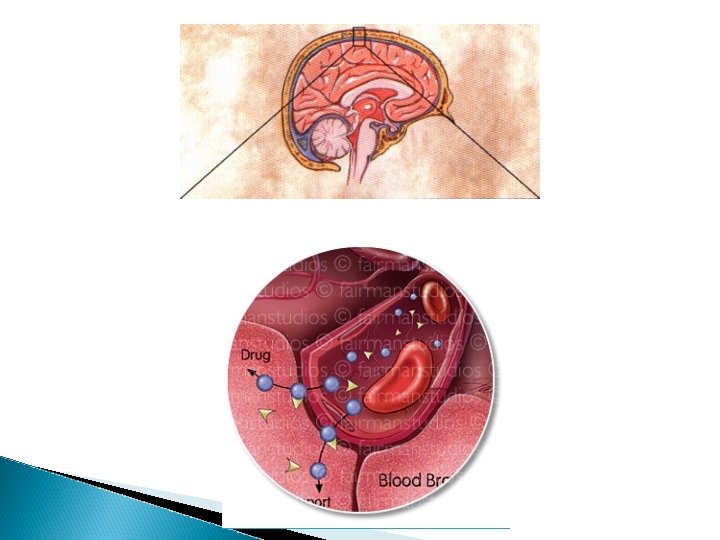
Additional issue for drugs to reach the CNS � Blood brain barrier- ◦ layer of thickly packed epithelial cells and astrocytes that restrict access of many toxins/drugs to the brain
3 Factors that affect how well a drug can cross the blood brain barrier (or placental barrier) � Lipid fats solubility – how soluble the drug is in ◦ cell membranes are lipid bilayers ◦ similar characteristics allow drugs to cross brain as to cross into cells
3 Factors that affect how well a drug can cross the blood brain barrier � Lipid � Size solubility of molecule � Ionization (+ or -) – whether the degree has a charge
� p. Ka – the p. H at which ½ of the molecules are ionized � most drugs are either weakly basic or weakly acidic Basic drugs are highly ionized in acidic environment � Acidic drugs are highly ionized in basic environment �
� p. Ka – the p. H at which ½ of the molecules are ionized the closer the p. Ka of the drug is to the local tissue p. H, the more unionized the drug is. ex. morphine – p. Ka of 8 stomach ~ p. H ~ 3 caffeine – p. H. 5
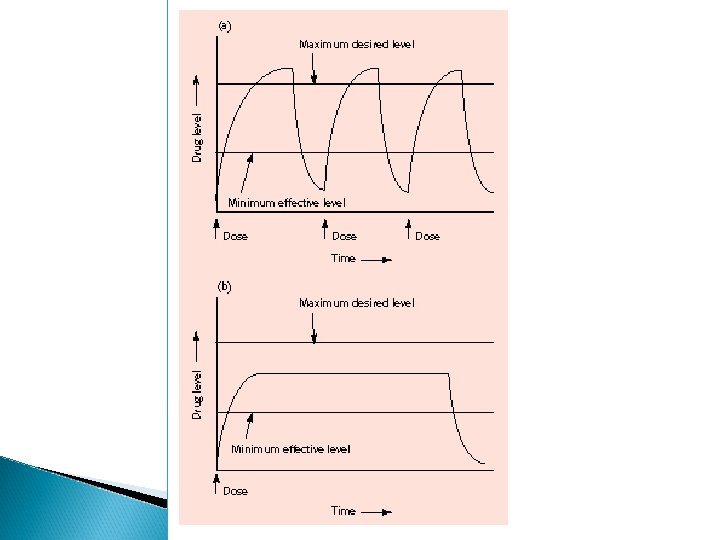
Distribution half-life and therapeutic levels ◦ Distribution half-life: the amount of time it takes for half of the drug to be distributed throughout the body ◦ Therapeutic level: the minimum amount of the distributed drug necessary for the main effect.
Until this time, drug movement has been mostly passive from regions of higher concentration to lower concentration. Elimination of drugs usually requires more of an active process (except gaseous drugs).
How are drugs eliminated? 1. Biotransformation (metabolism) chemical transformation of a drug into a different compound in the body (metabolite) Most biotransformation takes place in the liver
2. Excretion - removal of drug to outside world ***Drug elimination may be by both or either of these mechanisms
Biotransformation � role of liver ◦ most significant organ in biotransformation
Biotransformation � role of liver ◦ most significant organ in biotransformation ◦ largest organ in body ◦ serves many functions �transforms molecules via enzymes
Liver enzymes biotransform drugs (and other compounds) by 1. deactivating the molecule 2. ionize the molecule 3. make it less lipid soluble ** product of biotransformation is called a metabolite
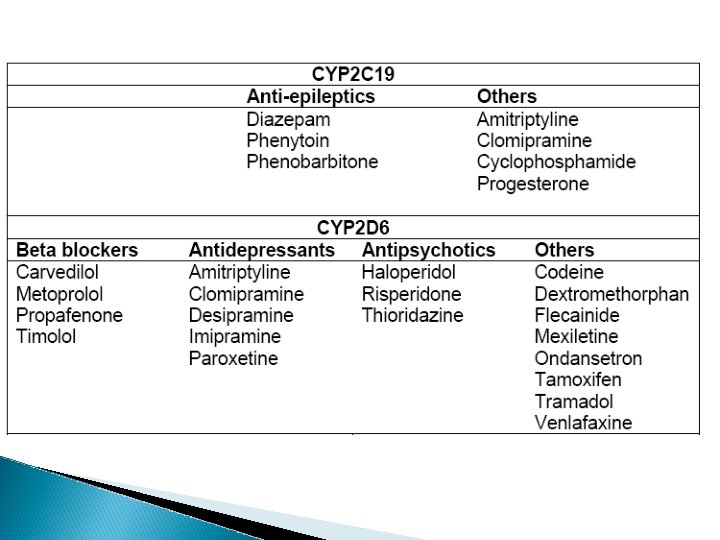
Cytochrome p 450 enzyme family � located primarily in hepatocytes � important for metabolism of alcohol, tranquilizers, barbiturates, antianxiety drugs, estrogens, androgens, PCBs and other agents � oxidative metabolism – makes drugs more water soluble (so more easily excreted) � There about 12 CYP families. ◦ CYP 1, 2, and 3 = most common for drug metabolism. ◦ CYP 2 D 6 and CYP 3 A (especially 3 A 4) metabolize over 50 percent of drugs.
Can metabolism rate be altered? � CYP enzymes - ◦ enzyme induction �liver produces extra enzyme to break down drug with continued exposure
Pharmacokinetics Examples and Consequences: St. John's Wort: (with active ingredient hyperforin) stimulates a receptor (SXR in humans, PXR in nonhumans) in the liver to induce CYP 3 A, CYP 3 A breaks down many other drugs: theophylline (asthma), warfarin (anticlotting), birth control pills, and immunosuppressant cyclosporin.
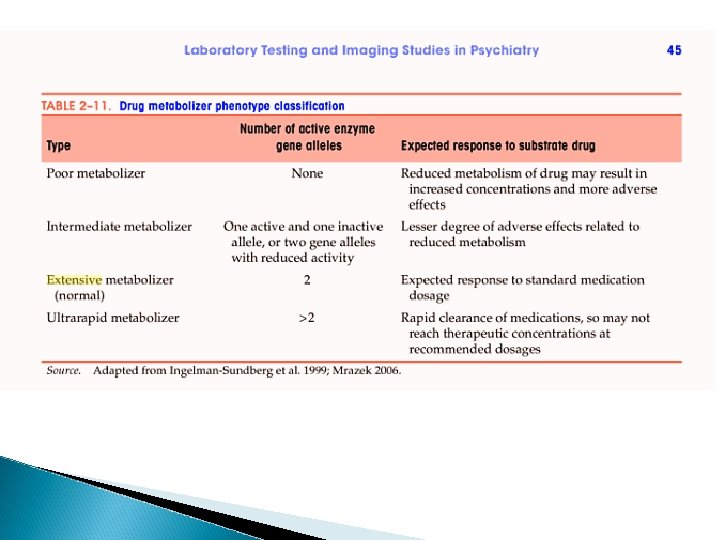
Can metabolism rate be altered? � CYP enzymes ◦ enzyme induction �liver produces extra enzyme to break down drug with continued exposure � Genetics
Pharmacokinetics
� Estimates that there is a 10 -year gap between medically relevant bio-technological advances and appropriate application, or translation into routine medical practice
Pharmacokinetics � Enzyme Inhibition ◦ Some drugs inhibit CYP enzymes and increase their own levels, as well as levels of any other drug metabolized by that enzyme. Can produce toxicities. ◦ Example: Inhibition of antipsychotic medication by SSRIs.
Can metabolism rate be altered? � CYP enzymes - ◦ enzyme induction - �liver produces extra enzyme to break down drug with continued exposure �Genetics �Liver disease
cirrhotic liver
In some cases, biotransformation can be to another psychoactive compound ex. benzodiazepenes diazepam nordiazepam oxazepam
Pharmacokinetics � Excretion ◦ Primarily accomplished by kidneys. Ø 2 organs (about the size of a fist) located on either side of the spine in the back. Ø Keep the right balance of water and salt in the body Ø Filter everything out of blood and then selectively reabsorb what is required. Ø Can be useful for eliminating certain drugs in overdose.
Routes of Excretion- fluid � all drugs not in gaseous state need to use fluid routes of excretion ◦ fluid routes include -sweat, tears, saliva, mucous, urine, bile, human milk ◦ amount of drug excreted in each of these fluids is in direct proportion to amount of fluid excreted SO…….
Pharmacokinetics � Sometimes drugs are not metabolized and are excreted intact. ◦ Lithium ◦ Mushroom amanita muscaria �In large doses it is toxic and lethal; small amounts are hallucinogenic. �Hallucinogenic ingredients are not greatly metabolized and are passed to the urine. Siberian tribespeople discovered this and recycled the drug by drinking their urine.
Pharmacokinetics � Sometimes drugs are not metabolized and are excreted intact. ◦ Lithium ◦ Mushroom amanita muscaria �In large doses it is toxic and lethal; small amounts are hallucinogenic. �Hallucinogenic ingredients are not greatly metabolized and are passed to the urine. Siberian tribespeople discovered this and recycled the drug by drinking their urine.
absorption, distribution and excretion do not occur independently
Other factors that affect drug pharmacokinetics 1. Body weight - smaller size • concentration of drug based on body fluid 2. Sex differences 3. Age
Other factors that affect drug pharmacokinetics 4. Interspecies differences rabbits – belladonna (deadly nightshade) 5. Intraspieces differences 6. Disease states 7. Nutrition 8. Biorhythm
� half-life - time takes for the blood concentration to fall to half its initial value after a single dose �½ life tells us critical information about how long the action of a drug will last
How long would it take for a drug to reach 12. 5% remaining in blood if its ½ life is 2 hours? How long would it take for a drug to reach 12. 5% remaining in blood if its ½ life is 100 hours?
first pass metabolism blood brain
Pharmacokinetics ADME