Antithrombotics Thrombolytics Antiplatelet drug Anticoagulants Thrombolytic Fibrinolytic drugs
 Antiplatelet drug Anticoagulants Thrombolytic/ Fibrinolytic drugs Gp IIb/IIIa inhibitors abciximab, eptifibatide, tirofiban")
Antithrombotics (Thrombolytics) Antiplatelet drug Anticoagulants Thrombolytic/ Fibrinolytic drugs Gp IIb/IIIa inhibitors abciximab, eptifibatide, tirofiban ADP receptor/P 2 y 12 inhibitors Thienopyridines : clopidogrel, prasugrel, ticlopidine Nucleotide/nucleoside analogue : Cangrelor, Ticagrelor Prostaglandin analogue beraprost, prostacyclin, iloprost, treprostinil Cox inhibitors aspirin, aloxiprin, indobufen, triflusal Thromboxane inhibitors dipyridamole, picotamide Phosphodisesterase inhibitors cilostazol, ditazole Vit K antagonist (inhibit II, VII, IX, X) Warfarin Factor Xa inhibitors Heparin group : heparin, LMWH Oligosaccharides : fondaparinux, idraparinux Heparinoid : danaparoid, sulodexide, dermatan sulfate Xa inhibitors : Apixaban, Rivaroxavan Direct thrombin inhibitors Bivalent : hirudin, lepirudin, desirudin Univalent : argatroban, dabigatran, melagatran Other antithrombin III, protein C, defibrotide Plasminogen activators alteplase, reteplase, tenecteplase, urokinase, streptokinase

2009 Scandinavian Society of Anaesthesiology and Intensive Care Medicine Guidelines

Levels of thromboembolism risk and recommended thromboprophylaxis in hospital patients 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline

Risk Factors of Stent Thrombosis Patient/Clinical factors Advanced age Acute coronary syndrome Reduced left ventricular ejection fraction Diabetes Renal failure Gene polymorphism/ Antiplatelet resistance Hypercoagulable states Prior brachytherapy MACE within 30 days of PCI Procedural/angiographic factors Suboptimal malapposition, underexpansion Overlapping/ long/ multiple stent Reidual dissection Side branch occlusion Coronary anatomical factors Small vessel Type C / Left main/ Bifurcation/ Bypass graft lesion Total occlusion Stent factors Drug eluting stent Hypersensitivity to polymer Antithrombotic and anticoagulation therapy Cessation of antiplatelets Inhibition of platelet aggregation

Risk Factors and Estimated Incidence for Spinal Hematoma and Central Neuraxial Anesthesia 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline
 • Warfarin : interfere the")
Anesthetic Management of the Patient Receiving Oral Anticoagulants (1) • Warfarin : interfere the synthesis of Vit-k dependent clotting factor Factor Half life Enhanced PT response to warfarin Factor VII 6 -8 Age > 65 yr Factor IX 24 Female gender Factor X 25 -60 Factor II 50 -80 Weight < 100 lb Excessive surgical blood loss Liver, cardiac, renal disease Oriental race CYP 2 C 9, VKORC 1 genetic variation, or both • US labeling of warfarin : CIx in spinal puncture and lumbar block 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline
 • Management of patients receiving")
Anesthetic Management of the Patient Receiving Oral Anticoagulants (2) • Management of patients receiving preop warfarin : controversial Recommendations Discontinue warfarin 4 -5 days before Against the concurrent use of aspirin, NSAIDs, ticlopidine, clopidogrel, UFH, LMWH Receiving low dose warfarin : daily INR monitoring Neurologic testing of sensory and motor function : routinely
 • Thromboprophylaxis in pts. with")
Anesthetic Management of the Patient Receiving Oral Anticoagulants (3) • Thromboprophylaxis in pts. with indwelling catheter Indwelling catheter Neurologic check INR < 1. 5 should be removed at least 24 hrs after removal 1. 5 < INR < 3 remove with caution Before catheter removal & until the prophylaxis INR level INR > 3 No definitive recommendations, Hold or reduce warfarin 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline

Anesthetic Management of the Patient Receiving Antiplatelet Medications Medication Recommendations NSAIDs, aspirin, Cox-2 inhibitors No specific concerns Against if the concurrent use of oral anticoagulat, UFH and LMWH is anticipated in the early post. OP. Ticlopidine After 14 days of discontinuation Clopidogel After 7 days of discontinuation (If neuraxial block is indicated 5 -7 days of discontinuation → normalization of platelet function should be documented) Gp IIb/IIIa inhibitors Abciximab : after 24 -48 hrs of discontinuation Eptifibatide/tirofiban : after 4 -8 hrs of discontinuation

Thromboprophylactic medication that should not be interrupted before surgery Patients treated with platelet inhibitors for secondary prevention of thromboembolic events ASA and clopidogrel (or ticlopidin) should be interrupted only during the day of surgery in patients with Myocardial infarction Coronary intervention: CABG Mechanical dilatation Coronary stents Stroke/TIA /intracranial intravascular stents 2009 Scandinavian Society of Anaesthesiology and Intensive Care Medicine Guidelines

Perioperative Management of the Patients on Antiplatelet Therapy Patients with coronary stents Elective surgery postponed for the following durations if aspirin and thienopyridine (eg, clopidogrel) therapy must be discontinued Bare metal stents: 4~6 week Drug-eluting stents: 12 month If surgery cannot be postponed, continue aspirin throughout perioperative period Patients at high risk for cardiac events (exclusive of coronary stents) Continue aspirin throughout the perioperative period Discontinue clopidogrel at least 5 d (and preferably 10 d) before surgery Resume clopidogrel 24 hrs postoperatively Patients at low risk of cardiac events Discontinue antiplatelet therapy 7~10 d before surgery Resume antiplatelet therapy 24 hrs postoperatively

Algorithm of Perioperative Management of Patients with DES

Anesthetic Management of the Patient Receiving Unfractionated Heparin UFH Neuraxial Blockade Prophylaxis : 5000 U s. c. No contraindication > 10, 000 U of UFH daily, or ≥ twice-daily dosing Safety not established Receiving more than 4 days After platelet count test. Cardiac surgery & full dose Insufficient data Vascular surgery Acceptable with following recommendations 1) avoid in pts. with other coagulopathies 2) Delay heparin for 1 hr after needle 3) Remove indwelling catheters 2 -4 hrs after last heparin dose 4) Post. OP neurologic monitoring 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline
 • Anti-Xa level : not predictive")
Anesthetic Management of the Patient Receiving LMWH (1) • Anti-Xa level : not predictive of bleeding • Regardless of LMWH dosing, avoid concomitant - antiplatelet or oral anticoagulant, dextran • Preoperative LMWH Pre. OP LMWH Recommendation Prophylaxis doses Needle at least 10 -12 hrs after LMWH dose Higher doses Delay at least 24 hrs <2 hrs pre. OP Against a neuraxial technique 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline
 • Postoperative LMWH thromboprophylaxis : safely")
Anesthetic Management of the Patient Receiving LMWH (2) • Postoperative LMWH thromboprophylaxis : safely undergo single injection & continuous cath. Twice-daily dosing Single-daily dosing * risk of hematoma ↑ 1 st dose at least >24 hrs 2 nd dose Indwelling cath. 6 -8 hrs at least >24 hrs should be removed 10 -12 hrs of last dose 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline

Anesthetic Management of the Patient Receiving Thrombin Inhibitors/Others Medication Recommendations Thrombin inhibitors (Desirudin, Lepirudin, Bivalirudinm Argatroban) Against the performance of neuraxial techniques Fondaparinux Under conditions used in clinical trials 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline

Anesthetic Management of the Patient Receiving Thrombolytic Therapy Thrombolytic/Fibrinolytic Tx. Neuraxial technique recommendations Scheduled to receive 10 days after thrombolytic drugs Have received Against of spinal/epidural anesthesia Near the time of needle Neurologic monitoring : interval < 2 hrs 2010 American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideline

2010 European Society of Anaesthesiology Recommendations

2009 Scandinavian Society of Anaesthesiology and Intensive Care Medicine Guidelines
 of anticoagulants prior to (after) catheter insertion/removal UFH")
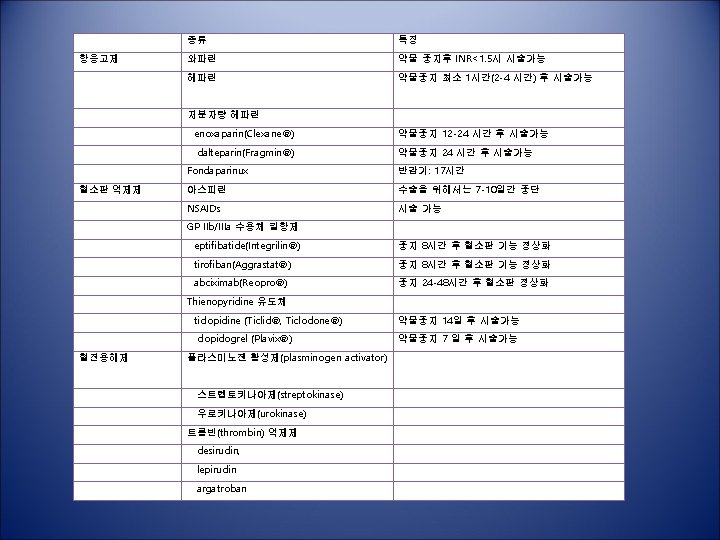
Respect time interval for cessation (initiation) of anticoagulants prior to (after) catheter insertion/removal UFH LMWH Fondaparinux Warfarin Antiplatelet Stop 4 h prior to catheter insertion/removal Restart at least 1 h after catheter insertion/removal Stop 12/24 h (prophylactic/therapeutic) prior to catheter insertion Restart at least 4 h after catheter insertion/removal Start 6– 8 h after catheter insertion Stop 36 h prior to catheter removal Restart 12 h after catheter removal Stop 4– 5 days prior to catheter insertion CNB perform If INR<1. 4 Aspirin Not contraindicated Clopidogrel Stop 7 days Ticlopidine Stop 14 days Abciximab Stop 48 hrs Tirofiban/ Eptifibatide Stop 8 hrs CNB : Central neuraxial block, UFH : unfractionated heparin, LMWH : low molecular heparin

Summary • Avoid multiple anticoagulant/antiplatelet therapies prior to CNB • Ensure normal haemostasis prior to catheter insertion/removal • Close neurological monitoring for signs of spinal epidural hematoma after CNB
- Slides: 23