Vulvar Dermatoses ERIN MAHONY CNM 2515 Various Vulvovaginal





 � Marked epidermal atrophy evidenced by thin, wrinkled, “cigarette paper\" appearance.")
 of developing")




 �May taper to a midpotency corticosteroid over time. �Testosterone (old tx) Not")
 �Pt’s who fail to improve as expected should be evaluated for allergic")

 �Pre-pubertal girls with LS may have remission at puberty. Sx improve")

























 or Benadryl 10")








 n n n Deeply ingrained hygiene practices “No problems in the")
 n n n Causes Wet: Urine, feces, sweat, panty liners/pads Dry:")
 n Benzocaine (Vagisil)")
 Douches Medications – TCA, 5 FU Spermicides Yeast")

 n n n Sitz baths Topical steroid Ointments (not creams")






 �Broad age range �Remarkable diversity in")
 �Symptoms: pruritus and less often pain �Diagnosis: Cannot be recognized with certainty")
 �Etiology: One group a/w HPV, other not. �High risk HPV strains in")















 n n n Presents with: dyspareunia, pain with touch, pressure to vulva")
 n n Most women think they have chronic yeast or BV. May")



")


. All anecdotal, no clinical trials. n n Neurontin (gabapentin) 300 mg po")
 n n n n SSRI’s – Effexor XR 37. 5 mg to")


 �Brown to black �Smooth surfaced �Flat macules or elevated papules")





- Slides: 110
Vulvar Dermatoses ERIN MAHONY, CNM 2/5/15
Various Vulvovaginal disorders �Lichen Sclerosus �Lichen Planus �Lichen Simplex Chronicus �Contact Dermatitis/Folliculitus �Disorders of Pigmentation �Benign Neoplasms �VIN/SCC/Basal Cell/Paget's/Melanoma �Vulvodynia/Vestibulodynia
�Today – primarily focus on external vulvar conditions � Common symptoms, PE findings, diagnosis, treatment options, follow up and when to refer �Review vulvodynia/vestibulodynia
Lichen Sclerosus �Chronic inflammatory skin condition �Often but not always association with other autoimmune disease �Familial pattern �Bimodal age distribution: Prepubertal and peri/postmenopausal (hypo-estrogen states) � 3 -10 x more common in women �Prevalence ~10 -100/100, 000 (under-recognized? )
Clinical Presentation of LS � SYMPTOMS: � Pruritus, often severe. 80 -90% of pts � Dyspareunia: 60 -70% � Pain with defecation: 20% (esp children) � SIGNS: � Predilection for genital skin. Does not involve the vagina. � Flat, pearly white papules and plaques (hypopigmentation) extending from vestibule outward. � Perianal involvement is common - forming a “figure of 8” configuration
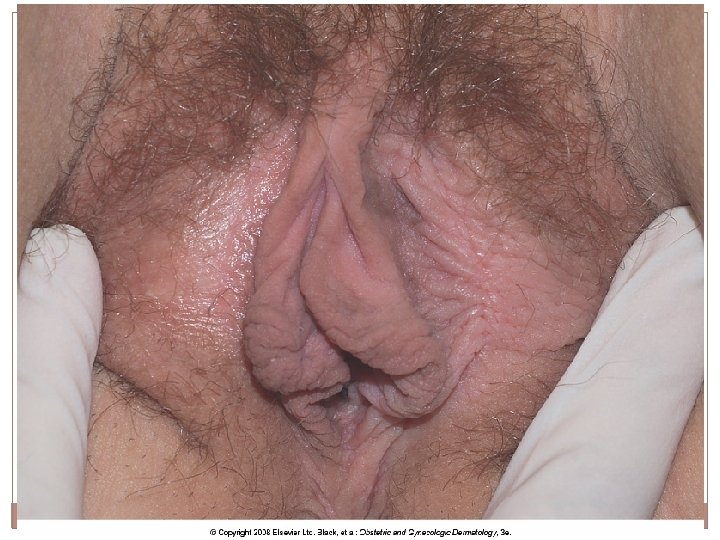
Lichen Sclerosus (cont) � Marked epidermal atrophy evidenced by thin, wrinkled, “cigarette paper" appearance. (old name Lichen Sclerosus et Atrophicus) � Epidermal fragility leads to areas of ecchymoses � Fissures and erosions occur with minor trauma (sex, speculum exam, exercise) � Architectural distortion – resorption of labia minora, clitoral hood agglutination, narrowing of introitus
Increased Risk of Neoplasia with LS � 3 -5% risk (above baseline) of developing SCC (squamous cell carcinoma) � Cannot be sure by visual appearance – biopsy to r/o or confirm neoplasia. �High potency topical steroid tx may ↓ risk of SCC? By controlling inflammatory response?
DIAGNOSIS of Lichen Sclerosis �Can be made clinically in “classic cases” by experienced provider. �Histologic confirmation is preferred. �Even “fully developed” LS can be inapparent on bx and diagnosis vague. Several bx may be required. �Bx to confirm your diagnosis and r/o neoplasia
PROGNOSIS �Cannot reverse architectural damage that has already occurred. �Steroid treatment can prevent further/on-going destruction. �For example: clitoral hood agglutination will likely not regress, but may be surgically released. Will reagglutinate if fail to treat postop with potent topical steroids. �May develop post-inflammatory hyperpigmentation
TREATMENT � Improve the environment! Control of local irritants and treat infections. � Ultrapotent topical steroids: Clobetasol 0. 05% ointment once to twice daily x 1 - 3 months. � Freq visits at 2, 6 & 12 wks. Begin taper to QOD. Then taper to 2 -3 x/wk for long term maintenance. � Judicious use of steroids – More is NOT better. Studies confirm safety when used as directed.
�Follow for: 1. 2. 3. 4. 5. Steroid atrophy Control of sx On-going architectural destruction Concerning lesions needing bx Secondary infections.
Treatment (cont) �May taper to a midpotency corticosteroid over time. �Testosterone (old tx) Not useful. �Estrogen if concurrent urogenital atrophy (peri/postmenopausal) �Surgery: repair damaged tissue; use steroids concomitantly
Treatment (cont) �Pt’s who fail to improve as expected should be evaluated for allergic contact dermatitis to clobetasol or other topical substances. �Evaluate for secondary infections: yeast, bacterial, HSV, atrophic vaginitis, SCC �Consider presence of an additional or different primary cutaneous diagnosis.
FOLLOW UP �After LS is well controlled, see pt 1 -2 x/yr �Monitor for non-healing ulcers or persistent hyperkeratotic lesions suggestive of SCC. Biopsy prn. �Many women will d/c steroid because they are asx. LS generally recurs with gradual “silent”scarring.
Follow up (cont) �Pre-pubertal girls with LS may have remission at puberty. Sx improve as estrogen produces more resilient epithelium, but ongoing scarring can occur even in the absence of sx in untreated skin. Need to look/examine despite embarrassment! �Sx may recur at or around the time of menopause. �Long-term follow up is suggested to prevent morbidity including late SCC. Especially in elderly and/or debilitated women. Genital exam continues to be important! (even if she no longer “needs a pap”)
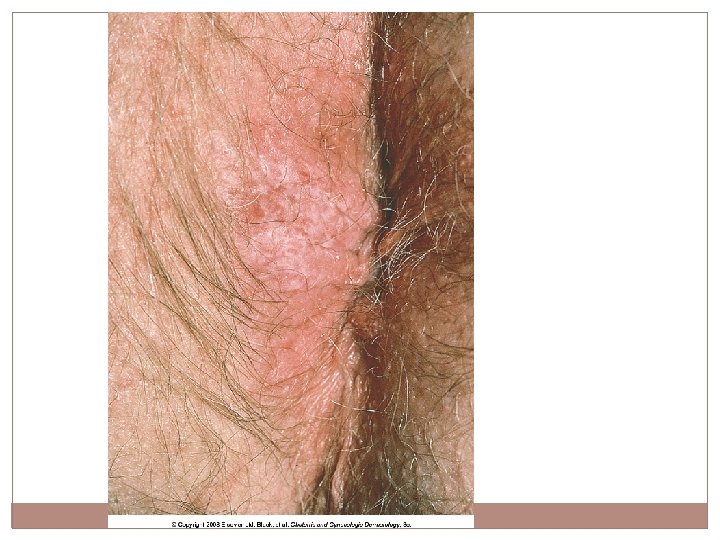
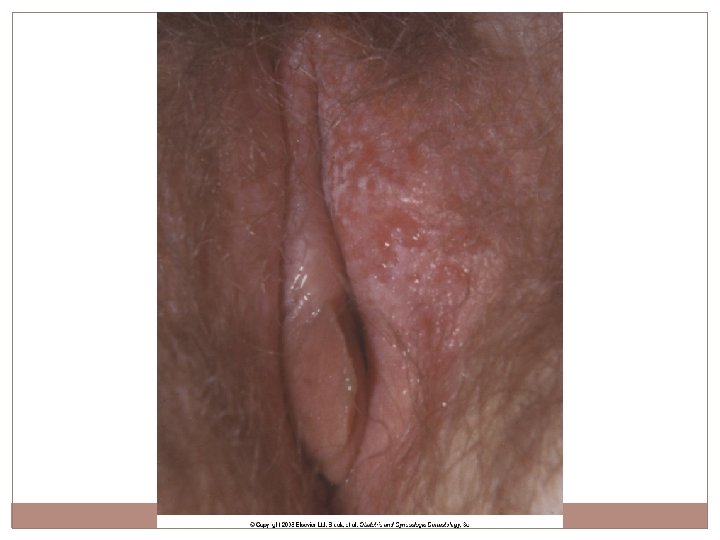
Classic LS manifested by white, sharply demarcated plaque. Skin is shiny and crinkled with loss of labia minora and partial agglutination of clitoral hood.
LS preferentially affecting the periclitoral skin and perineal body.
Periclitoral area is often the first affected. Edema and smooth, shiny skin ar early skin changes of LS.
Cellophane paper crinkling of perianal skin is nearly pathognomonic for LS
Smooth, hypopigmented, nearly waxy skin occurs in some women with LS Noted here on the medial labia majora
More long-standing disease is likely to manifest as hyperkeratot or macerated skin. The perineal body is especially prone to thickened LS
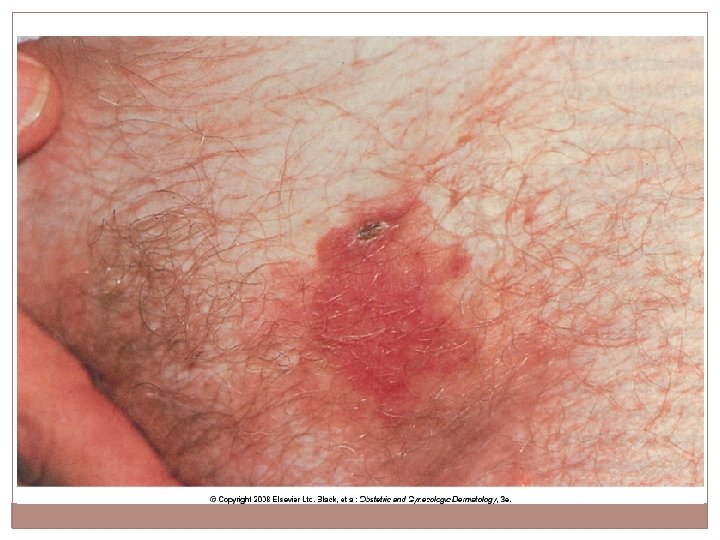
Superimposed thickening and purpura from rubbing
Purpura in setting of white, crinkled skin in a child
Fissure in natural skin folds
Thin, fragile skin is prone to fissuring, erosion and secondary infection from minor irritants.
Irregular erosions produced by scratching
Agglutination of labia minora. Partial agglutination of clitoral hood in advanced LS
Ongoing agglutination clearly evident on anterior vulva
Anterior midline agglutination of vulva has produced narrowing of introitus
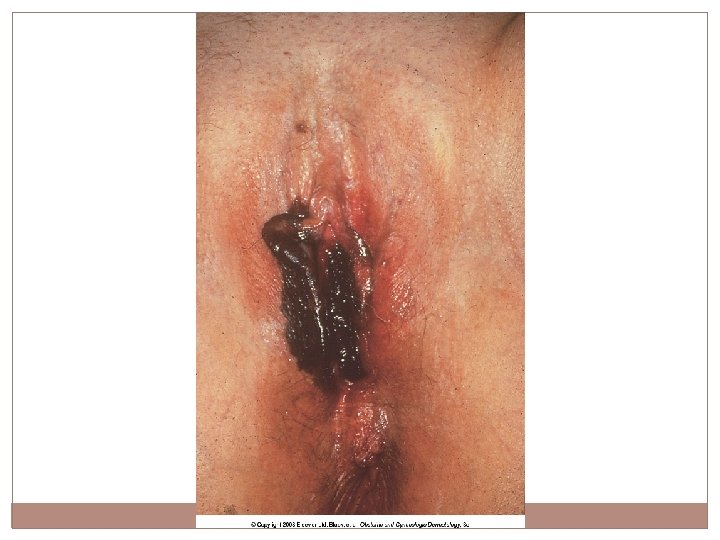
89 yo with excruciatingly pruritic undiagnosed LS presented with painful nodule. Bx confirmed SCC
Recalcitrant hyperkeratotic LS is the morphology most at risk for transformation into SCC
Hyperkeratotic lesion Should be treated aggressively Biopsy if recalcitrant due to tendency to evolve into SCC
Patchy hyperpigmentation is Very common in LS, most visible after therapy
Before treatment: typical white plaques
After treatment the skin exhibits normal color and texture
Lichen Simplex Chronicus �“The Scratch that Itches” – a vicious cycle �Often present for weeks/months/years! �Often misdiagnosed as “yeast infection” �Antifungals may decrease, but not eliminate sx �Remember: All that itches is not yeast! �Genital pruritus is the single most frequent presenting symptom in anogenital region �Often severe, intractable, awakes from sleep. Will scratch “till it hurts or bleeds” �Pruritus affects activities “All consuming”
LSC �Itch may develop into burning pain �Worse with heat, stress, menses, synthetic clothing, OTC products, pads �Must control night time scratching or it will undo almost all of the benefit of a daytime treatment program.
LSC �Up to 75% have personal or FH of atopic disease �Full skin exam �Consider secondary infection – yeast/bacterial �Bx generally not necessary except to r/o other conditions
LSC - Treatment �Vulvar care measures: Stop the Itch-Scratch-Itch cycle �R/O infection as precipitating or driving factor �Steroids �Sedation �Pt education re: chronicity. Recurrence is expected and does not represent a treatment failure.
LSC – Treatment - Steroids �Systemic vs Topical �Clobetasol oint 0. 05% BID x 2 wks, then daily for 2 wks, then 3 x/wk for 2 wks. Then prn. �Oral corticosteroids may be necessary (short term). Medrol dose pack vs Prednisone (40 mg Q am x 5, then 20 mg po Q am x 10) �Intralesional steroids if severe (rarely req. ) �IM steroids – Triamcinolone (Kenalog) 80 mg deep into buttock
LSC – Treatment - Sedation �Nighttime Itching: � Hydroxyzine (Atarax, Vistaril) or Benadryl 10 -25 mg QHS 2 hrs prior to bedtime Increase by 10 -25 mg each week until scratching ceases or SE’s prevent further increase. Max benefit usually btw 50 -75 mg. Do not exceed 150 mg. Doxepin if fails hydroxyzine (same dosing) TCA (amitriptyline) 10 mg with gradual increase to 50 mg QHS 2 hrs prior to bedtime.
LSC – Treatment – Sedation �Daytime Itching �If nighttime therapy is insufficient to control daytime itch/scratch �SSRI – Prozac (20 mg Q am), Paxil, Zoloft �Celexa 10 -20 mg Q am, increase weekly to max of 60 mg. �Quite effective – mechanism of action poorly understood.
Red, lichenified, poorly demarcated plaques classic for LSC
Thickened from rubbing. Irregular erosions from scratching Redness less well appreciated in dark skinned pts
Erythema Exaggeration of skin lines Scale Fissuring
Licenification Erosions
Hair has been rubbed off from chronic rubbing/scratching
Note thick, rough skin Hyperpigmentatio In dark skin Activation of melanocytes from inflammation and rubbing
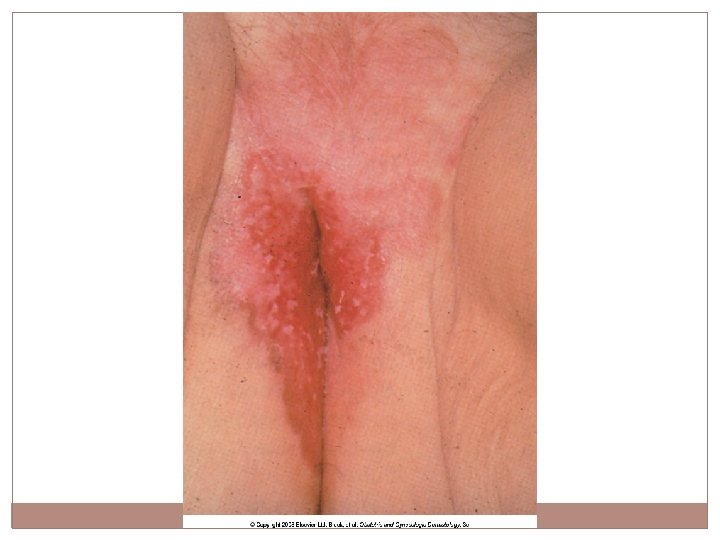
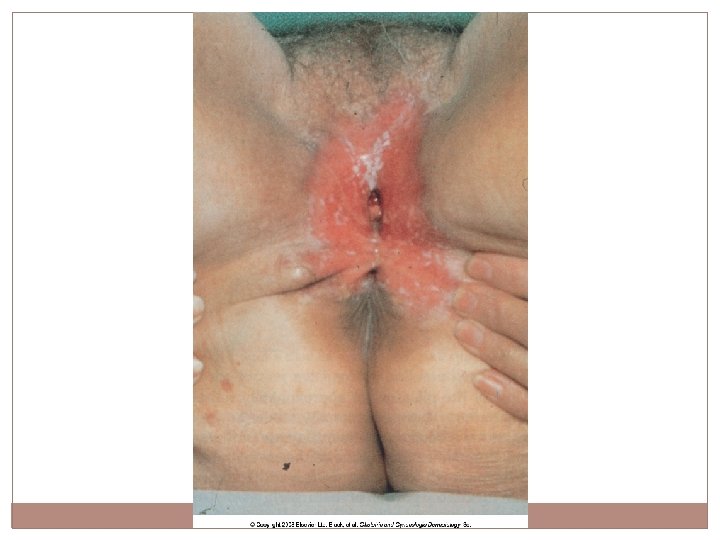
Contact Dermatitis Caused by Irritants, Allergens or Both n Sx: Vulvar Burning, Irritation, Pain, n Signs: n Acute – Erythema, Edema, Erosions n Chronic – “dusky” or “violaceous” hues, cracks, fissures, dry or chapped skin EVERY woman (and most providers) think she has yeast! n
Contact Dermatitis (cont) n n n Deeply ingrained hygiene practices “No problems in the past” “Used this same product for years”. The same product can cause sx after long use without problems. Correct dx based on hx. Pts forgetful, reticent or ashamed to admit to practices. Sometimes iatrogenic (TCA, Aldara, Podophyllin etc) Never underestimate what products women might apply to the vulva when desperate!
Contact Dermatitis (cont) n n n Causes Wet: Urine, feces, sweat, panty liners/pads Dry: Over energetic hygiene – perceived odor, “dirty”. Hot water, harsh detergents, harsh towels. “Normal” soap and water too frequently.
Common Vulvar Allergens/Irritants ALLERGENS (initial sensitization to antigen 7 -10 d) n Benzocaine (Vagisil) – The most common offender! n Preservatives n Neomycin / Bacitracin / Sulfa products n Latex condoms n Chlorhexadine (K-Y) n Lanolin n Perfume n Nail polish n Nickel (piercing) n Semen n Yeast as an allergen?
IRRITANTS Soaps/Cleaners Sweat/Urine/feces Rx Creams (alcohol) Douches Medications – TCA, 5 FU Spermicides Yeast creams (Monistat) Estrogen creams Panty liners/pads
Contact Dermatitis Treatment n n STOP offending agent or behavior! Easier said than done. Educate re hygiene practices. Warm H 20 only. No soap. No daily panty liners. Shaving/waxing? Products a/w these practices? Skin protection (plain zinc oxide ointment or paste keeps moisture away from skin) Lubrication/moisturizer - vegetable oil, Crisco, petrolatum
Contact Dermatitis Treatment (cont) n n n Sitz baths Topical steroid Ointments (not creams – which have ETOH, preservatives, stabilizers) Mid-High potency – Triamcinolone 0. 1% or Fluocinonide 0. 05% BID for 1 -2 wks.
n Immunological memory lasts a very long time. Subsequent contact with an allergen will lead to redevelopment of allergic contact dermatitis even after years with no exposure to the offending agent. Pts can be remarkably sensitive to very small amounts of antigen, requiring great care to insure complete avoidance.
Harsh disinfectants produce an exudative, vesicular, edematous acute irritant dermatitis
Allergic contact dermatitis. Pt applied topical neomycin, to which she was allergic.
Candidiasis Edema, scale and fissuring
Shaving folliculitis is an irritant condition produced by short, stiff, sharp hair curling back into the skin.
Folliculitis on The buttocks. Red papules and pustules
Premalignant and Malignant Neoplasms �VIN (vulvar intraepithelial neoplasia) �Broad age range �Remarkable diversity in appearance �Color highly variable: White, brown-black, pink, red �Surface may be scaling, crusted or eroded �Most appear de novo on background of normal skin. May be superimposed on lichenified skin or other skin lesions – LS/LP (Lichen Sclerosus/Lichen Planus)
VIN (cont) �Symptoms: pruritus and less often pain �Diagnosis: Cannot be recognized with certainty based on clinical exam. BIOPSY! �Differential Dx: EGW, seborrheic keratoses, psoriasis, LSC, LS, LP or others? �Call pathologist to clarify bx results if non- specific!
VIN (cont) �Etiology: One group a/w HPV, other not. �High risk HPV strains in 75% of VIN (younger women) � 80 -90% of these contain HPV 16 (encourage HPV vaccine) �May have multifocal dz. 50% have CIN, Va. IN or anal intraepithelial neoplasia �Other risk factors: HIV, immonosuppression smoking, persistent HPV
�Non-HPV VIN: �Older �Unifocal �A/W Lichen Sclerosus, Lichen Planus �Gene mutation
VIN – Take home points �May be asx �Have high index of suspicion esp with LS/LP �Avg time from sx to bx is 2 yrs! �Bx if NEW, Raised, Pigmented lesion �Consider other hx: Abn pap, Va. IN �Spontaneous regression is uncommon
VIN Irregular red surface with white, keratotic, flat-topped papules. Immunosuppressed kidney transplant pt with HPV infection
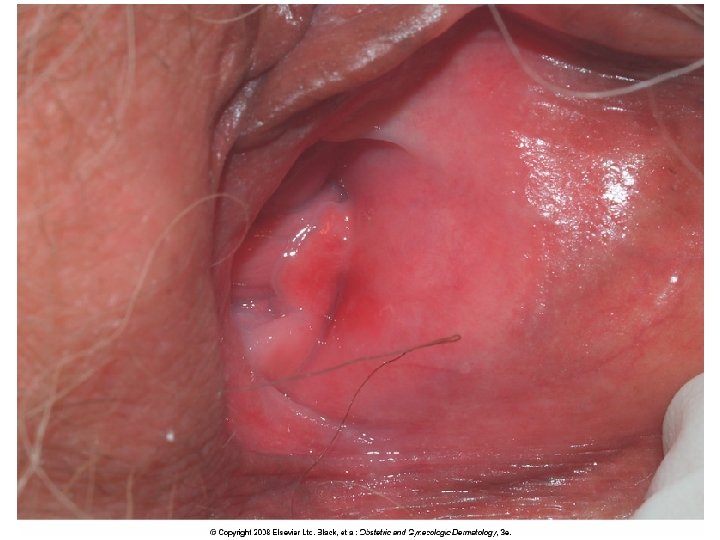
VIN in background of Lichen Sclerosus Appears erosive
VIN Appears inflammatory or erosive. Mimicking plasma cell Vulvitis and lichen planus This pt has LS and hx of SCC – removed by vulvectomy. Now with VIN 3
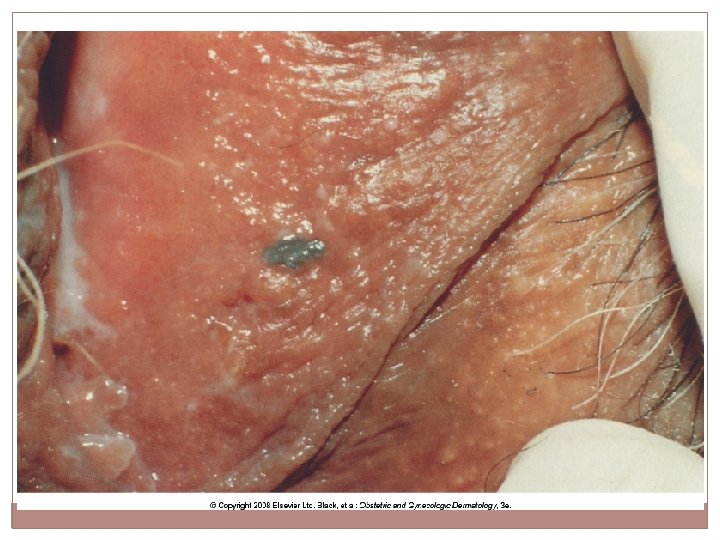
On keratinized skin, VIN appears rough and scaly
Perianal intraepithelial Neoplasia in pt with Lichen Sclerosus
Erythema and hyperpigmente plaque and papules of multifocal VIN
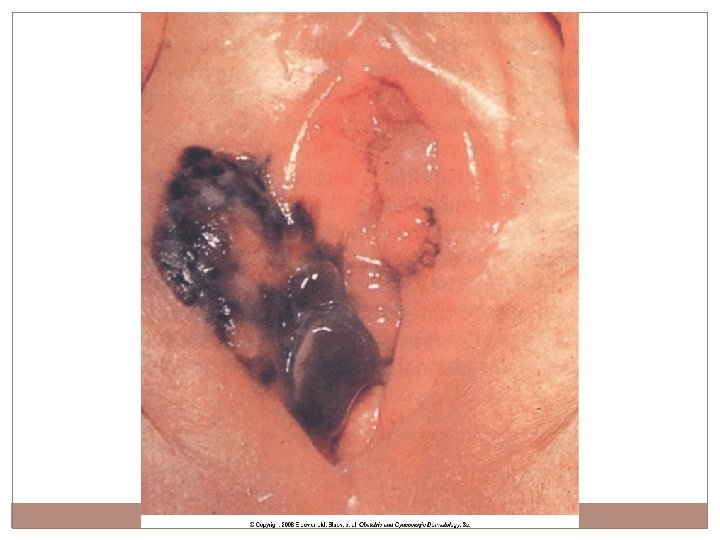
Squamous cell carcinoma
Invasive SCC Arising in the setting of classic Lichen Sclerosus
Extramammary Paget’s 1 -3% of vulvar cancers �Appears only on apocrine gland bearing skin (labia majora) �Typically older, white women �Median age 70. Range 50 -80 �Mixed areas of scale, crust, erosions. White “islands” of tissue scattered throughout widely eroded areas. Sx: Pruritus, pain, discharge Failure to respond to steroids and/or antifungal agents A/W breast, Urologic and GI adenocarcinoma
Melanoma � 3 -5% of vulvar malignancy �White women, age 50 -80 �A few reports in children with Lichen Sclerosus �Asymptomatic but can be pruritic, painful, bleed or have discharge. �Predilection for clitoris, labia minora and inner aspect of labia majora �Tx: Wide excision, sentinel node biopsy
Vulvodynia and Vestibulodynia n n Vulvodynia: chronic burning, stinging, irritation, soreness, rawness, stabbing or other painful sensation of the vulva in the absence of any clinical or laboratory abnormalities. Itching is not a typical symptom Subsets: Generalized, Localized Provoked, Unprovoked, Mixed
Vulvodynia (cont) n n n Presents with: dyspareunia, pain with touch, pressure to vulva including tight clothes, wiping, tampons. May be independent of touch or pressure and is chronic, daily and unprovoked Pain ranges from mild/annoying to severe pain that precludes ADL including exercise, walking, sexual activity or even sitting.
Vulvodynia (cont) n n Most women think they have chronic yeast or BV. May be coincidental, not causal. Sx may decrease but rarely resolve with tx Convinced they have resistant infections, immune compromise or “systemic yeast” Co- morbidities: IC, constipation, IBS, fibromyalgia, H/A, TMJ, low back pain, depression, anxiety, PMS, multiple medication “allergies”/sensitivities PE unimpressive with no obvious cause for pain
Vestibulodynia n n n Specific and localized to the vulvar vestibule. Q-tip touch elicits severe pain Sx: insertional dyspareunia, pain or inability to use tampons, ride bike/horse, tight clothes Clitorodynia subset Primary vs Secondary PE: Normal with exception of erythema localized to the ostia of the vestibular glands
Both Vulvodynia and Vestibulodynia work up n HISTORY n Careful PE including cultures (yeast, CT/GC), wet mount. n Don’t do general vaginal cultures – yield coincidental trivial infection or colonization n Bx is nonspecific
n Neuropathic pain. Result of trauma/infection n Some – peripheral neuropathy Others – complex regional pain syndrome, injury or other insult that triggers the pain. Others – CNS processing disorder where normal touch is perceived centrally as painful (allodynia). Explains comorbid conditions? n n
n Pelvic Floor – increased resting tension and irritability, but overall weakness (poor Kegal) n Benefit from Pelvic Floor Physical Therapy
n n n Decreased estrogen receptors in the vulva Estrogen deficiency may result in an increase in local nerve density Improvement with topical estrogen? Depression and psychosexual dysfunction – as a cause or result of vulvar pain? Psychological factors play a striking role in some pts and a minor role in others.
Treatment – No FDA approved treatments for vulvar pain syndromes n n Education and Counseling – Validate: real disease and not alone (National Vulvodynia Association www. NVA. org) Minimize irritants Lidocaine gel 2% or ointment 5% prn TCA’s: amitriptyline, nortriptyline, desipramine taper: 10 -25 mg po qhs x 1 wk, 2 po qhs x 1 wk, 3 po qhs, 4 po qhs. Max 100 mg. Start low, go slow. Do not stop abruptly, taper.
Treatment (cont). All anecdotal, no clinical trials. n n Neurontin (gabapentin) 300 mg po qd x 3 d, then bid x 3 d, then tid. Stay x 1 month, increase gradually prn. Do not exceed 2700 to 3600 mg/day. No more than 1200 mg in a single dose. Lyrica (pregabalin) 50 mg qd x 4 d, then 50 mg bid x 4 d, then 50 mg tid. Can gradually increase up to 100 mg tid. Doses up to 300 mg bid have been used for pain control
Treatment (cont) n n n n SSRI’s – Effexor XR 37. 5 mg to 150 mg SSNRI’s – Cymbalta 20 mg to 60 mg Intralesional injections – steroid + anesthetic Interferon - ? No better than placebo? Botulinum toxin 20 -40 units into levator ani muscle, vestibule, perineal body Surgery: Vestibulectomy 60 -85% success Pelvic Floor PT/ Biofeedback Couples Counseling and Sex Therapy
Topicals n n n Gabapentin ointment 2 -6%, 7. 5%, 10% (compounded in aqueous base with or without lidocaine 5%) Apply to AA bid-tid Disp: 30 -60 gm Amitryptyline 2% + Baclofen 2% in aqueous base. Apply qd-tid. Disp: 30 -60 gm Doxepin 5% cream Apply qd-qid. Disp: 30 gm Topical nitroglycerin? Estrogen cream (if atrophic)
MORE PICTURES IF WE HAVE TIME?
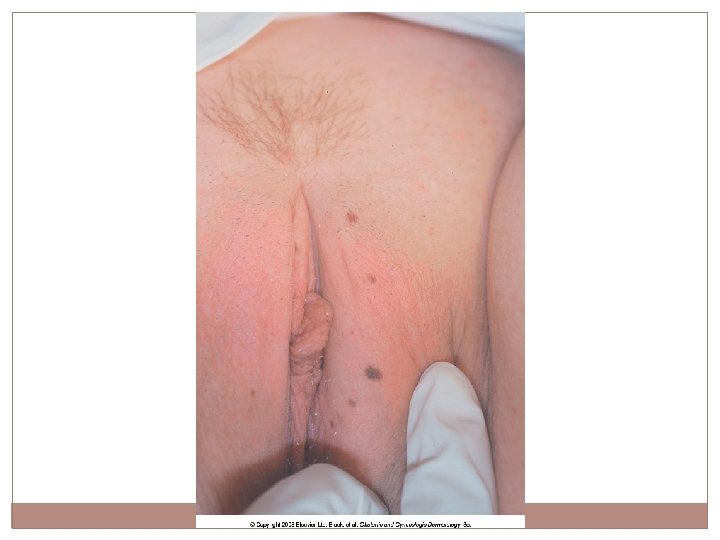
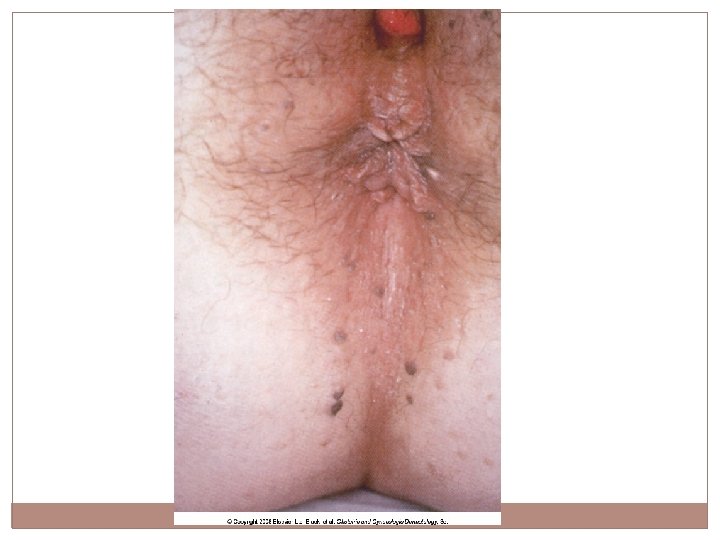
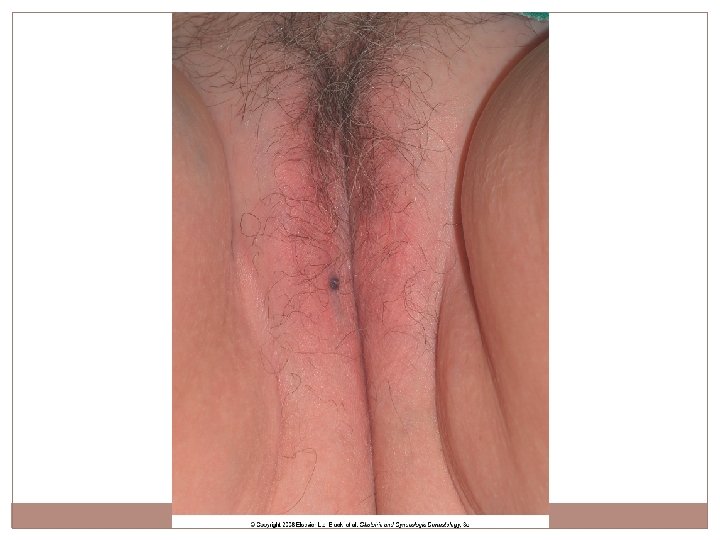
Benign Neoplasms Nevi (moles) �Brown to black �Smooth surfaced �Flat macules or elevated papules �Biopsy if not sure