Real Engagement for Real Improvement Resources to Engage



















 A")





 HOW")










![Assess Site Relationships • What is your current level of [family/partner] engagement? • What](https://slidetodoc.com/presentation_image_h/77c639f8f1504e6e093f1f97b4cfce3d/image-38.jpg "Assess Site Relationships • What is your current level of [family/partner] engagement? • What")




























! The WVP fosters trust and respect and creates")


- Slides: 69
Real Engagement for Real Improvement: Resources to Engage Families and Community Partners to Improve Services to Promote Health of Young Children and Families: A Case Study Christina Bethell, Ph. D, MBA, from Help Me Grow! MPH Kathleen Powers, MPH
Association of Maternal and Child Health Programs Annual Meeting 2018 The presenters document that they have no financial relationships to disclose or conflicts of interest to resolve. Child and Adolescent Health Measurement Initiative
Session Objectives Objective 1: Introduce the Well Visit Planner as tool and ASPIRE project to advance outcomesbased, integrated and family-centered systems of care goals Objective 2: Illustrate the use of the Well Visit Planner within Help Me Grow sites as a model to advance community based integrated systems of care Objective 3: Consider the adaptation of the Well Visit Planner implementation resources and model for Title V goals. The goal of this session is to engage participants in considering the use of IT based family engagement tools like the Well Visit Planner to advance state performance in improving MCH outcomes and systems performance in partnership with community organizations, families, and children’s health services providers.
Cross Cutting Relevance of Well Child Care to Title V NPMs and NOMs? • Prevention and Health Promotion are critical in a child’s healthy development • Vital services, such as screenings and immunizations are provided • Early Identification of potential issues • Education of the parents/guardians about the child’s developmental milestones and associated age-appropriate behaviors • Clarification of needs for additional psychosocial and developmental screenings Well child visits present an essential leverage point for: • • Engaging parents in the health and well being of their child Early identification of physical, social, emotional and behavioral issues Provision of critical anticipatory guidance and education for parents Promoting positive child and family health, resilience, social and emotional skills
Title V NPMs – How many are related? NPM 1: Well-Woman Visit NPM 2: Low-Risk Cesarean Delivery NPM 3: Risk-Appropriate Perinatal Care NPM 4: Breastfeeding NPM 5: Safe Sleep NPM 6: Developmental Screening NPM 7: Injury Hospitalization NPM 8: Physical Activity NPM 9: Bullying NPM 10: Adolescent Well-Visit NPM 11: Medical Home NPM 12: Transition NPM 13: Preventive Dental Visit
Implementing sciences of healthy development and thriving Advances in the sciences of human development create unprecedented opportunities to proactively advance child well -being. Breakthrough findings across disciplines point to a new science of thriving that illuminate often untapped capacities for the promotion of healthy development and healing despite adversity. Given high rates of adversity, healing is prevention. Key to this possibility are policies and practices that enable and support families and communities to recognize and learn to heal and flourish in the face of stress and adversity. Child and Adolescent Health Measurement Initiative (CAHMI)
The non-negotiable and science-based mandate to fully engage and empower children, youth and families to promote early and lifelong health Child and Adolescent Health Measurement Initiative
Online and Mobile Optimized Tool for Families www. wellvisitplanner. org www. cahmi. org
WVP Website Step 1 Step 2 Step 3
The Well Visit Planner produces a Summary Visit Guide that includes information about the parent’s priorities for the visit and issues abut the child and family identified in the questions. The parent can download, print, save and/or email the Summary Visit Guide to their provider or others as they wish
Produces population-based, provider, clinic or community level data on child and parent strengths, concerns, developmental milestones, psychosocial issues, priorities and status of developmental screening and more. Relevance for meaningful use, MOC, medical home and value based payment efforts, etc. Emerging tool for CSHCN/CMC 12
Three Continuous Cycles of Work Research • Need and Design: Family and • • provider interest in and design using qualitative, JAM and User-X methods Measures and Methods: Measurement science to translate guidelines for parents and ways to ask parents about key topics and to develop and validate parent reported quality metrics Standardization and stakeholders: Process to engage AAP, family leaders, NQF, etc to “endorse” methods Evaluation: Feasibility and acceptability for practices and families Validation/RCT: Effectiveness and Development • Simple: Building simple, short, cost • • effective IT tool Flexible: Enabling use via public use website with account registration (no PHI), EHR integrated and “My Chart” enabled High Value: Align with NQF measures, meeting ABP Maintenance of Certification requirements and Meaningful Use Part 4 Accessible and Customizable: Free online site registration, customization and back end population based data capture and automated feedback reports Evolving Applications…. Field Testing & Implementation • Quasi-experimental, mixed • • methods (26 clinicians; 3 practices rural, urban, suburban); N=3800 Age: 0 -3, English FQHC’s Randomized Control Trial: Focus on 0 -2 years. Tumaini Coker’s PARENT Coach Model – used PHDS and WVP. Community Based Navigators and Families: Family Voices, Head Start/EHS, Help Me Grow, Home visiting, Healthy Steps, Other
Promoting to Families
FROM ONLINE TOOL ------- Into the EHR FORMS Parent completes tool online Well-Visit: MA/MD sign file, forms opened with data insereted HL-7 File Created of Parent’s Answers MEL Code use to insert parent responses INTO the EHR Forms American Academy of Pediatrics 2011 National Conference and Exhibition Completed HL 7 File Sent to Secure TCC IP Socket HL-7 File Pulled into EHR
How Does the WVP Help Parents? Engages parents to reflect and learn about issues they can and should address during well visits • about child’s developmental milestones and age-appropriate behaviors • Creates a pathway to discuss psychosocial and developmental screening (etc) • Importance of parent and family well being as central to child’s development and wellbeing. • Ensures parents know their own priorities for the well child visit Example Results From RCT Using the WVP in Federally Qualified Health Centers Doubling of psychosocial assessment and near 1005 on developmental screening. 50% decrease in emergency department visits for group using the WVP
Myths, Challenges, Facts and Feedback about Family Engagement Facts & Feedback Myths & Challenges • • • Parents won’t want to do this Parents don’t have time Tool is redundant, won’t work Language and literacy issues Cultural barriers No access to computer or printer Family connection & history with providers & staff • Perceived value • Provider fear of opening dialogue with no follow-up resources available • • • Feasibility: 92% were comfortable with time to complete (average 9 minutes or less) Value Added : • 92% would recommend the WVP to other parents. • 92% said the WVP increased the value of their visit. • 75% said the tool was very or extremely useful for focusing their time with their child’s health care provider on what was most important to the family. Promoting Patient Centered Care: WVP was helpful (79%) Supplemental Educational Materials were helpful (75%) Tool and supplemental materials are available in English and Spanish Tool is written at 8 th grade reading level Tool is optimized for mobile use
Relationships Matter! The WVP fosters trust and respect and creates time for relationship. New Findings from the 2016 National Survey of Children’s Health Family Often 3 or more of 5 Practices 4 Qualities Protective Family of Resilience When Routines & Habits Facing Problems Practiced How often providers spend enough time* Always 73. 1% 74. 7% Sometimes/Never 47. 9% 53. 6% How often providers listens carefully to parents* Among children with 2+ ACEs whose parents report that their child’s health care providers “always” listen, spend needed time and give needed information are over 1. 5 times more likely to live in families that practice four basic resilience skills when they face problems. Always Sometimes/Never Children whose parents report “always” having positive communication with their child’s health care providers are over 1. 5 times more likely to practice 3 or more (of 5) recommended protective family routines and habits. Always Sometimes/Never 71. 0% 46. 1% 72. 6% 56. 0% How often specific information needed is provided* 70. 7% 45. 9% 72. 5% 51. 9% *Odds ratios adjusted for income/FPL and race/ethnicity all significant: With “always” responses to each experience of health care factors, odds are 2. 68 -2. 79 greater that families often practice 4 resilience qualities than with “sometimes/never” (1. 46 -1. 54 for “usually”). Odds. 41 -. 50 less for practicing 2 or fewer (vs. 3 -5) protective family routines and habits with “always” responses compared to “sometimes/never” (“usually” responses did not differ from “sometimes/never”).
What we hear! Parents: “I didn’t get my email!” Providers: “I can’t live without my CAHMI visits” American Academy of Pediatrics 2011 National Conference and Exhibition
Advancing Support in Promoting Family Engagement and Referral Linkages through Technological Innovations (ASPIRE) A Coordinated Effort between the Child and Adolescent Health Measurement Christina Bethell, Ph. D, MBA, MPH Paul Dworkin, MD Initiative (CAHMI) and the Help Me Grow (HMG) National Center The Child and Adolescent Health Measurement Initiative Executive Vice President for Community Johns Hopkins Bloomberg School of Public Health Founding Director, Help Me Grow National Center Department of Population, Family and Reproductive Health Connecticut Children’s Medical Center Professor of Pediatrics ASPIRE Advisory Committee Call January 26 th, 2018
Rationale of Project Implement and assess the impact of an innovation that will enhance core components of the HMG Model to support the optimal development of children.
Project Goals “Help education families; be able to integrate WVP into current system of referrals” “Help encourage families going into a well child visit” “Help with partnerships for developmental monitoring- with parents and providers” “Push for normalizing HMG” “Decrease the percentage of families who had no primary care provider for their child”
Milestones and Progress to Date AKA: Successes! § Site Specific Branding and Data Collection for the WVP: Established WVP online tailored registration and tracking features § Toolkits: Tailor pre-implementation guide, implementation toolkit, readiness checklist, and promotional materials § Real-Time Design Based Coaching: Developed coaching process for HMG sites § Community of Practice: Conducted 4 site-wide webinars to train, support and track learnings
Primary Developmental Requirements AKA: Challenges! § Workflow Adaptations and Changing Habits: HMG site adaptations to their workflow and capacity to advance the use of the WVP. § A New Conversation with Families: Novelty and nuances for engaging parents and normalizing the use of engagement tools. § Pediatrics Integration: Engagement with pediatric practices is new and evolving. Use of the WVP has value even as integration evolves. § Growth Mindsets and Meaning Making: Tendency to label normal/expected barriers as a “problem” vs. what is meant to be overcome by innovation. § Cultural Fluency: Language barriers for sites with populations who speak language other than English or Spanish
Finishing Phase: Design. Based Coaching and Goal 2: Evaluation Goal 1: Set, track and iteratively revise goals and think ahead on issues that could arise during WVP implementation at a HMG site Develop an empowered relationship to “barriers” and be prepared to develop strategies for engaging families & parents, staff, and child health providers. Facilitate cross-site learning. Goal 3: Incorporate sustainable system changes based on lasting collaborative practices.
Advancing Support in Promoting Family Engagement and Referral Linkages through Technological Innovations (ASPIRE) HOW IT WORKS
Project Participants • Help Me Grow National Staff • CAHMI/JHU Staff • 6 Help Me Grow Affiliate Sites: • Alabama • San Francisco • South Carolina • Brevard County (FL) • Heart of Florida • Palm Beach/Treasure Coast
Project Activities 01 12 -Month Participation 04 The current project formally began with recruitment in April 2017 and will conclude March 2018 02 Technical Assistance and Peer Learning Through provider outreach strategies, sites will partner with local primary care practices in their adoption and utilization of the WVP 05 Sites will receive support through a variety of technical assistance formats, such as calls, webinars and peer learning opportunities 03 Support to Families Engage Practices Data Tracking and Reporting Sites will collect and report data relevant to WVP implementation 06 Care coordinators will support families in utilizing the WVP to prepare for wellchild visits and become a partner with their child’s provider 04
Overview of Project Phases 1. Create Leadership Team & Champions 3. Sites Plan their Implementation Strategy and Receive Coaching and Cross. Site Learning Webinars 5. Continue to coach and support sites to innovate in building capacity, relationships and processes 2. Conduct Readiness Assessment and Support Staff to Implement the WVP 4. Develop Registration Portal and Ensure Each Site Registers and Begin Implementation 6. Real Time Tracking and Final Evaluation and Report on Lessons and Opportunities for Next Steps
Key Factors for Implementation Internet/technology access Engaging pediatric health care providers Time involved for staff and parents Engaging other community organizations Staff training and buyin Monitoring and evaluation Well-visit scheduling Educating parents on using the WVP Maintaining consent and confidentiality for families Different cultures and languages
Create Leadership Team and Champions Key personnel responsible for implementation at your site. May include: • Program/Executive Directors • Program Manager/Coordinators • Family Resource Specialists • Care-coordinators • Other supporters (e. g. board members, providers or other stakeholders for your HMG site) At a clinical site: • Office Manager • Front Desk Staff • Physicians/PAs/Nurse Practitioners • Nurses & Technicians • Care Coordinators • Medical-Legal Partnership Staff
Creating a Leadership Team Purpose: • Enthusiasm for and commitment to the project • “Train-the-trainer” for on-going staff support • Identify issues and collaborate on solutions Tasks/Challenges: • What types of positions would you consider? • Individual meetings with potential members • Introductory meeting for leadership team – what would you discuss? • Other challenges?
Example Agenda for an Introductory Meeting I. Introduction II. Project Overview I. Present an overview of the WVP and how it works on computers & mobile devices II. Visit the WVP site and try out the tool online or on their mobile device: (www. wellvisitplanner. org). III. Discussion I. Why the WVP will be a useful tool II. How the WVP can fit into your existing structure III. Available resources for implementation IV. How parents will feel about using the WVP V. Potential barriers to the WVP process
Plan Implementation Strategy • Site-specific goals • What will your site do? • Timeline for activities • Utilization of existing resources • Best ways to train staff?
Example Implementation Timeline
Assess Site Relationships Help Me Grow-specifics: • Call center-based activities • Co-location with providers and/or practices (e. g. hospital) • Organizations in surrounding community (e. g. WIC) Other potential partners: • Local Health Departments • Parenting Programs • Home Visiting Programs • Head Start/Early Head Start • Early Education Centers • Child Welfare
Assess Site Relationships • What is your current level of [family/partner] engagement? • What are current issues? • What are potential issues with the WVP for families? • Communicating value of the WVP • Access to required technology • Cultural and language barriers • What are potential issues with the WVP for providers? • Staff work flow & capacity • Technological challenges with intake and EHR • Changes in well-visit flow • What are potential issues with the WVP for community organizations? • Relevancy to different types of community organizations • Cultural considerations • Technology barriers
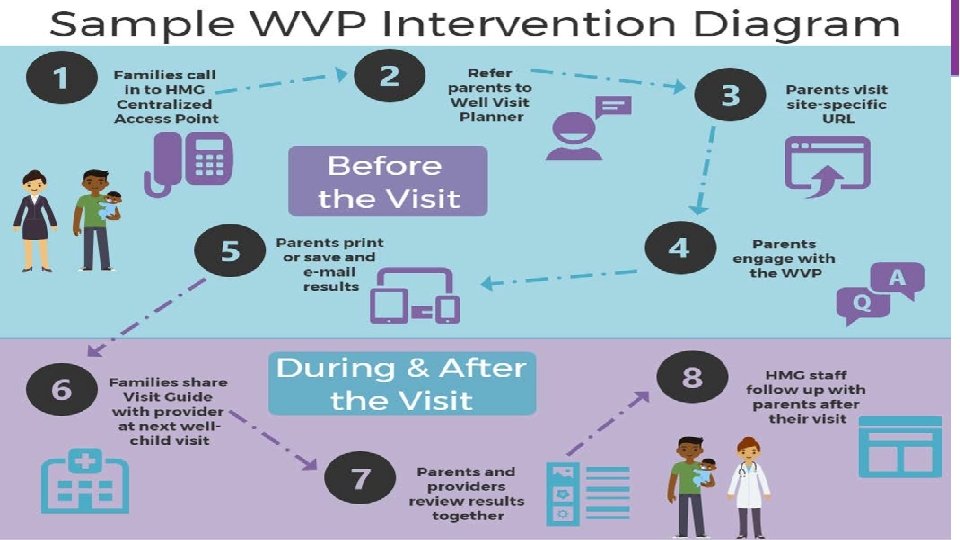
Prepare Staff to Implement the WVP Resources Available: • Pre-Implementation Guide • Training • Implementation Guide • Workflow (diagram) • Conduct a Readiness Assessment
Site Registration
Site Registration
Pilot Project Technical Assistance • Community of Practice among 6 affiliate sites participating • Webinars with all sites present throughout the project (every 1 -2 months) • One-on-one coaching calls with individual sites to help
Evaluation Process Impact Outcome • • Referral Form Family Participation Tracker Engagement in COP Feasibility • Family Participation Tracker • Degree of adoption • Satisfaction • Follow-up with families • Linkages from families use of WVP to well-child visit • Sustainability
Family Engagement Tracker
Tips for Maximizing the Impact of the WVP • Build trust with parents, and be sure to follow up • Plan in advance and work together • Ensure your team has adequate information and resources for parents • Anticipate potential barriers
Promote the WVP to Families
Relevance and Adaptation for Title V?
ASPIRE to Move Toward Engagement 3. 0: • • Engagement is required to meet goals for child health and well-visits Engagement is an experience, process, intervention and an outcome Medical decision making— engage to decide Setting health goals – engage to set goals and make plans to meet them Self-care and behavior change— engage to motivate action & change Problem solving- engage to navigate, notice & address problems Advocacy to create supportive community, work and living environments – engage to advocate and get help Engagement to design, assess and improve systems and services – 3. 0
Title V NPMs – How many are related? NPM 1: Well-Woman Visit NPM 2: Low-Risk Cesarean Delivery NPM 3: Risk-Appropriate Perinatal Care NPM 4: Breastfeeding NPM 5: Safe Sleep NPM 6: Developmental Screening NPM 7: Injury Hospitalization NPM 8: Physical Activity NPM 9: Bullying NPM 10: Adolescent Well-Visit NPM 11: Medical Home NPM 12: Transition NPM 13: Preventive Dental Visit
Key Questions to Consider 1 2 3 4 5 Could the implementation of the WVP within Title V efforts build capacity to strengthen child health services and engage partnerships with communitybased programs like HMG that are external to the child health services sector? What is the relative desirability of implementing innovations like the WVP external to pediatric practice to support pediatric providers meet recommendations for well child care? How might adoption of the WVP serve as an opportunity to advance coordination and partnership with families, community-based services, and pediatric providers? How will we know if engagement and care has improved? What kind of feedback and evaluation is most useful? Assuming we agree the work to date has laid the groundwork for change, what are the strategies for scaling and sustaining the WVP and similar family engagement tools within Title V efforts?
Cross-Cutting Relevance of the ASPIRE Project Implement and assess the impact of an innovation that will enhance core components of the HMG Model to support the optimal development of children.
WVP Site Branded Registration 1. Go to: http: //www. wellvisitplanner. org/helpmegrow/register (can be used by other sites as well, not just Help Me Grow) 2. Have specific URL in mind 3. Have site logo ready to upload 4. Provide information about other tools your site would like to link to WVP
Several Implementation Toolkits 1. About the Well-Visit Planner 2. How the Well-Visit Planner Works 3. Implementing the WVP in a Help Me Grow Call Center (Head Start & provider versions available) 4. Implementing the WVP: Lessons from the Field 5. Tips for Maximizing the Impact of the WVP 6. Appendix A: Implementation Resources for the WVP 7. Appendix B: Suggested Parent Referral Information 8. How to Contact the CAHMI for Technical Assistance
Resources to Support a Continuous Improvement Plan Use the Pre. Implementation Guide and the checklist above to plan for WVP implementation. Implement changes or adaptations that may need to be made to better utilize what the WVP has to offer. Plan Do Act Stu dy Employ the materials in Appendix A and the guidance from the project webinars to implement the WVP. Evaluate the information on the Family Participation Tracker & the qualitative feedback from families.
Implementation Resources for the WVP Overview Materials Implementation & Evaluation • One Page Overview of the Well-Visit Resources Planner tool • Pre-Implementation Guide • History of the WVP • Sample Implementation Timeline • Guide to Topics and Questions • Family Participation Tracker Asked, the complete list of • Sample Script, for offering the WVP questions asked at each age group to families in the WVP • Sample Questions for Family Engagement Materials Feedback Provider Engagement • Family Posters Materials • Family Postcards • Provider FAQs • Family Media Toolkit, developed in partnership • Video Tutorials with Family Voices • Provider-specific • Child Stickers Implementation • AAP Bright Futures Guidelines, 4 th Edition: the Well Toolkit -Visit Planner is based on the AAP’s Bright • Supplemental Futures Guidelines for the delivery of well-child Implementation care. The CAHMI has developed parent handouts Resources
Implementation Readiness Checklist Internet/Technology Access All CAP staff have access to WVP on a computer or mobile device All CAP staff are comfortable with walking parents through the tool online There is a plan in place for what to do if a parent cannot complete the tool online (e. g. suggestions for accessing public computers, offering to fill out the tool online and mail parents the Visit Guide) If on-site CAP assistance is available, there is a computer/mobile device available for parents to use Length of Time for Staff and Parents All CAP staff are prepared for the amount of time it will take to go through the tool with parents All CAP staff can discuss benefits of tool with parents if they have concerns about time Staff Training All CAP staff have reviewed Pre-Implementation Protocol & Implementation Toolkit
Implementation Readiness Checklist Well-Visit Scheduling All CAP staff have been trained to ask parents about their child’s next scheduled wellvisit There is a list of pediatric providers/practices to refer parents to if they don’t already have one The list of Bright Futures recommended well-visits is readily available All CAP staff are comfortable with working with parents to schedule well-visits for their child There is a procedure for reminders and follow-up around well-visit scheduling Maintaining Confidentiality There is a plan in place for maintaining confidentiality of parents and children The Family Participation Tracker & any other data collection systems will be kept secure All CAP staff have been trained to get consent from parents for any data sharing and follow-up All CAP staff know what information is and is not stored in the WVP database, and are comfortable relaying that information to parents
Implementation Readiness Checklist Engaging Pediatric Healthcare Providers are informed about the WVP and where to get resources All CAP staff know where to find provider-specific resources If feasible, there is a plan in place for telling providers about families who may be coming into the visit having used the WVP Engaging Other Community Organizations For other community organizations where there is already a relationship, they have been informed about the WVP and where to get resources For other community organizations where there is not already a relationship, there is a plan in place to reach out to community organizations with information on the WVP Promotional materials have been distributed to community organizations Monitoring and Evaluation All CAP staff have been trained on the use of the Family Participation Tracker There is a plan in place for following up with families after their use of the WVP and documenting their responses All CAP staff understand the metrics that they are required to report on for this project
Implementation Readiness Checklist Educating Parents on the Well Visit Planner All CAP have been trained on how to introduce the WVP to parents All CAP staff feel comfortable explaining and discussing the WVP with parents Primary Language All CAP staff know how to access the tool in both English and Spanish There is at least one staff member who feels comfortable explaining the tool in Spanish and walking parents through it Community of Practice All CAP staff have been trained on how to access the Community of Practice discussion board All CAP staff actively participate in webinars throughout the project Site Registration The affiliate has come up with an individual URL for their site A staff member has uploaded the affiliate logo and registered their site
Key Questions to Consider 1 2 3 4 5 Could the implementation of the WVP within Title V efforts build capacity to strengthen child health services and engage partnerships with communitybased programs like HMG that are external to the child health services sector? What is the relative desirability of implementing innovations like the WVP external to pediatric practice to support pediatric providers meet recommendations for well child care? How might adoption of the WVP serve as an opportunity to advance coordination and partnership with families, community-based services, and pediatric providers? How will we know if engagement and care has improved? What kind of feedback and evaluation is most useful? Assuming we agree the work to date has laid the groundwork for change, what are the strategies for scaling and sustaining the WVP and similar family engagement tools within Title V efforts?
To Beauty …. and the translation of the science and practice of promoting positive health and healing for children, youth and families.
Contact Information Christina Bethell, Ph. D. , MBA, MPH Child and Adolescent Health Measurement Initiative Johns Hopkins Bloomberg School of Public Health Department of Population, Family and Reproductive Health cbethell@jhu. edu www. cahmi. org www. wellvisitplanner. org
Issues Interfacing with CHILD HEALTH PRACTICES & PROVIDERS
The WVP is new and requires change. How does it benefit me or my patients?
1 What does the evidence say? • Made in collaboration with the AAP and based on Bright Futures Guidelines in a four year development and testing process funded by HRSA/MCHB • Initially tested with 12 pediatric providers in Oregon, 92% of parents would recommend the WVP to other parents • RO 1 demonstrated improvement in care for Federally Qualified Health Centers (especially screening, urgent care visits, meeting parent priorities and psychosocial • screening) 2 Family Centered Care • The WVP empowers families to engage in their child’s health, utilizing the well-visit as a key encounter for early detection
3 Quality Measurement • Regular monitoring of WVP use, via the Family Participation Tracker • Feedback gathered from parents, staff, and providers 4 Quality Improvement • Engage parents in the well-visit to improve satisfaction of both parents and providers • Receive population based reports to look at whole population using the WVP • Opportunity for Maintenance of Certification (MOC) and use of the Online PHDS quality tool formal metrics on Bright Futures implementation
Providers and Relationships Matter (a lot)! The WVP fosters trust and respect and creates time for relationship. New Findings from the 2016 National Survey of Children’s Health Among children with 2+ ACEs whose parents report that their child’s health care providers “always” listen, spend needed time and give needed information are over 1. 5 times more likely to live in families that practice four basic resilience skills when they face problems. Children whose parents report “always” having positive communication with their child’s health care providers are over 1. 5 times more likely to practice 3 or more (of 5) recommended protective family routines and habits. Family Often 3 or more of 5 Practices 4 Protective Family Qualities of Routines & Habits Resilience When Practiced Facing Problems How often providers spend enough time* Always 73. 1% 74. 7% Sometimes/Neve 47. 9% 53. 6% r How often providers listens carefully to parents* Always 71. 0% 72. 6% Sometimes/Neve 46. 1% 56. 0% r How often specific information needed is provided* Always Sometimes/Neve r 70. 7% 45. 9% 72. 5% 51. 9% *Odds ratios adjusted for income/FPL and race/ethnicity all significant: With “always” responses to each experience of health care factors, odds are 2. 68 -2. 79 greater that families often practice 4 resilience qualities than with “sometimes/never” (1. 46 -1. 54 for “usually”). Odds. 41 -. 50 less for practicing 2 or fewer (vs. 3 -5) protective family routines and habits with “always” responses compared to “sometimes/never” (“usually” responses did not differ from “sometimes/never”).
How do I know this tool is valid? 1 Bright Futures Guidelines • WVP content was developed by an expert Advisory Group, including editors of the BF Guidelines and in close collaboration with parent advisors using best practice user centered and survey design methods 2 Pilot studies • Providers expressed concerns of additional paperwork, which could be simplified if sites make use a habit (integrated into work flow improved office efficiency) and if they elect to use the EHR integration WVP model • Providers valued the WVP’s attention to parent priorities (“I sleep better at night), psychosocial issues (quality doubled each study), cues to follow up on/refer for issues not usually (but recommended to be) addressed in well-visits and support/cues to fill developmental screening gaps
I don’t have time to market or offer this to families. Resources can make it easy for providers! ü Automated site registration, unique URL and clinic branding üAge-specific Parent Handouts (videos would be easy to create) ü Promotional posters and postcards ü FAQs for Families (can create family to family teams) ü Example social media posts and newsletter or website articles