Neonatal Hypoglycemia Alaa Al Nofal M D Assistant



























 l l l Newborn screen")
























- Slides: 54
Neonatal Hypoglycemia Alaa Al Nofal, M. D Assistant Professor of Pediatrics Pediatric Endocrinology University of South Dakota – Sanford School of Medicine
Objectives Ø Transitional Neonatal Hypoglycemia Ø Prolonged and Permanent Hypoglycemia Ø Causes of Permanent Hypoglycemia Ø Genetics Causes of Hyperinsulinemic Hypoglycemia Ø Other Causes of Hypoglycemia Ø Diazoxide
What is The Definition of Hypoglycemia in a Full Term Neonate <48 h Old? 1. Plasma glucose concentration less than 40 mg/dl 2. Capillary glucose concentration less than 35 mg/dl 3. Plasma glucose less than 47 mg/dl 4. Plasma glucose less than 60 mg/dl 5. Symptomatic neonate with glucose level less than 60 mg/dl 6. All/none of the above
Koh et al, Arch Dis Child 1988 Cornblath et al, Pediatrics 1990
WHO, hypoglycemia of the newborn 1997 Duvanel et al, JPeds 1999 Cornblath et al, Pediatrics 2000
Hay, JPeds 2009 Sweet et al, J pediatrics pharmacol ther. 2013 Rozance, Curr Opin Endocrinol Diabes Obes 2015
Al Nofal, SDPA conference 2018
Definition of Hypoglycemia in neonates Ø Ø No consensus exists as to the optimal definition of hypoglycemia in infants and children Some authors have suggested that the definition of hypoglycemia should be a blood glucose concentration of <40 mg/d. L Other investigators have suggested an even higher value of <47 mg/d. L Few other authors suggested raising the lower limit of normal to > 60 mg/dl as there is no evidence to prove that the newborn has a unique physiologic adaptation to Harris et al JPeds 2012 low blood glucose levels Cornblath et al Pediatrics 2000 Cole et al J Perinatol 1994 Sweet et al, J pediatrics pharmacol ther. 2013
It is known that plasma glucose concentration is lower in the first 1 -3 days of life in normal newborn infants than at later age
Ø Plasma glucose was checked fasting at 3 - 6 hour of age Ø Mean glucose level in term AGA infants was found to be 54 mg/dl – 126 newborn Pediatrics 1971
But why?
It All Starts in The Womb
Basics of Fetal Glucose Metabolism Fetal fuel metabolism is based primarily on oxidation of glucose Ø The fetus depends entirely on maternal supply and placental transfer of glucose Ø l l Ø There is no fetal glucose production under normal conditions In most cases, gluconeogenesis appears only after birth The fetal brain is exposed to circulating glucose concentrations only slightly below those of maternal plasma l ~9 mg/dl lower than mother’s glucose Stanley, Jpeds 2015 Hay Jpeds 2009
Basics of Fetal Glucose Metabolism Fetal insulin secretion is responsive to fetal plasma glucose concentrations Ø Fetal glucose concentrations are determined primarily by maternal glucose concentration Ø Fetal insulin primarily functions to regulate growth Ø Continuous fetal secretion of insulin would be important to maintain fetal growth Ø Stanley, Jpeds 2015 Hay Jpeds 2009
Basics of Fetal Glucose Metabolism Ø Pregnant women produce higher amount of ketones. l The generation of high plasma ketone levels would provide the fetus with an alternative fuel to protect the brain when plasma glucose is low Ø Making it unnecessary for the fetus to switch off insulin secretion and thereby avoid limiting growth Stanley, Jpeds 2015
Transitional Neonatal Hypoglycemia Ø In normal newborns, the mean plasma glucose drops immediately after birth Ø This is likely due to mild and transient form of hyperinsulinemia Ø The mean plasma glucose for suppression of insulin secretion is 55 -60 mg/dl shortly after birth l This is ~80 -85 mg/dl in older infants, children, and adults. Thornton, Jpeds 2015
Transitional Neonatal Hypoglycemia Ø As the glucose-stimulated insulin secretion mechanism matures, mean plasma glucose concentration in normal newborns increase. Ø It is similar to those of infants and children by 72 h of life l l The standard for normal neonates must never be extrapolated beyond 2 -3 days of life If possible, delay diagnostic evaluation for persistent hypoglycemia until 2 -3 days of life Thornton, Jpeds 2015
Basics of Fetal Glucose Metabolism Fetus needs glucose from the mother Fetus’ glucose level is ~9 mg/dl lower than mother’s Fetus needs insulin to grow Continuous fetal secretion of insulin would be important to maintain fetal growth Fetus has lower glucose threshold to turn off insulin secretion Stanley, Jpeds 2015 Hay Jpeds 2009
The mean plasma glucose at 8 hours of fasting after birth was 57+/-12 mg/dl Stanely et al Pediatrics 1979
The mean plasma glucose in normal newborn infants who fasted 24 h after birth was 57 -69 mg/dl. Murdina et al Jpeds 1954
Hypoglycemia After 2 Days of Life After the first 24 h of life, PG concentration does not differ at great extent with age Ø Mean PG in normal neonates after ~2 days of life is (70 -100 mg/dl) Ø Infants and children <4 years of age have limited fasting tolerance. Ø Thornton, Jpeds 2015
Etiology of neonatal hypoglycemia 1. Transient neonatal hypoglycemia Ø Day 1 of life: developmental immaturity of fasting adaptation First 2 days of life: transient hypoglycemia due to maternal factors - Maternal diabetes - Intravenous glucose administration during labor and delivery - Medications: oral hypoglycemics, terbutaline, propranolol Ø
Etiology of neonatal hypoglycemia 2. Prolonged neonatal hypoglycemia Perinatal stress-induced hyperinsulinism (low birth weight, birth asphyxia, maternal toxemia or preeclampsia, prematurity) Ø Beckwith–Wiedemann syndrome/Overgrowth syndromes Ø Hypopituitarism Ø
Etiology of neonatal hypoglycemia 3. Permanent neonatal hypoglycemia Ø Congenital hyperinsulinism - ATP-sensitive potassium channel hyperinsulinism - Glutamate dehydrogenase hyperinsulinism - Glucokinase hyperinsulinism - Short-chain 3 -hydroxyacyl-Co. A dehydrogenase hyperinsulinism - Congenital disorders of glycosylation Ø Counter-regulatory hormone deficiency - Hypopituitarism - Adrenal insufficiency Gluconeogenesis or glycogenolysis enzyme defects Ø Fatty acid oxidation disorders Ø
Workup for Neonatal Hypoglycemia Ø Thorough History and Chart Review l l l Gestational age Birth Weight Maternal History Family History Feeding History
Workup for Neonatal Hypoglycemia Ø Physical Exam l l l Macrosomia Signs of hypopituitarism (cleft palate, micropenis) Hepatomegaly Signs of Adrenal Insufficiency (hyperpigmentation) Signs of Beckwith-Wiedemann syndrome (omphalocele, hemihypertrophy, macroglossia)
Workup for Neonatal Hypoglycemia Ø Laboratory Evaluation (critical sample) l l l Newborn screen Confirmatory plasma glucose HCo 3 BOHB Lactate FFA
Workup for Neonatal Hypoglycemia BOHB, HCO 3, Lactate, FFA Adedmia Gluconeogenesis Elevated Lactate Elevated BOHB defect Prolonged fasting GSD GHD Adrenal insufficiency
Workup for Neonatal Hypoglycemia BOHB, HCO 3, Lactate, FFA No Adedmia Hyperinsulinism Hypopituitarism Perinatal stress Low BOHB Low FFA Low BOHB Elevated FFA FA oxidation defects
Hormonal Causes of Neonatal Hypoglycemia Hyperinsulinism Ø Adrenal Insufficiency Ø Growth Hormone Deficiency Ø
Congenital Hyperinsulinemia
Insulin secretion process Glucose SUR 1 Kir 6. 2 K+ GK VDCC ↑ATP/ADP Ca++ GLUT 2 Krebs cycle Leucin ADP + a-ketoglutarate GDH Glutamate Amino Acids Insulin
What is the most common form of congenital hyperinsulinemic hypoglycemia? ATP-sensitive potassium channel congenital hyperinsulinism
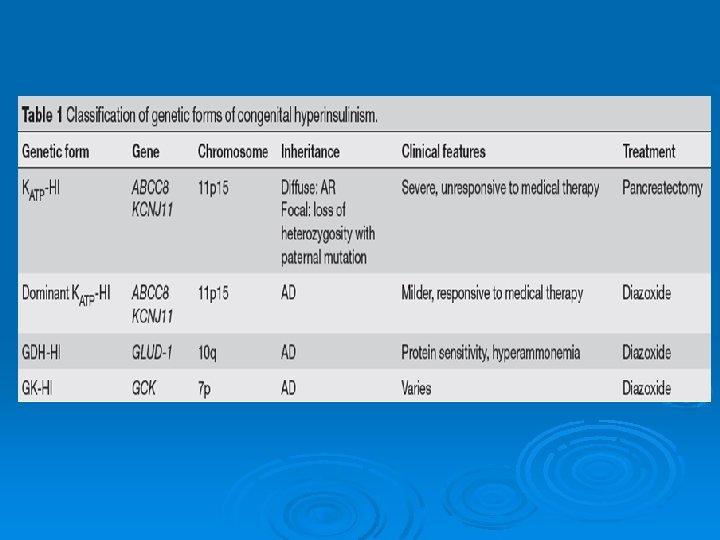
Genetic forms of Congenital Hyperinsulinemic Hypoglycemia “CHI” Ø Mutations in at least nine genes have been found to cause congenital hyperinsulinism. Most common are: Ø • • • The sulfonylurea receptor 1 (SUR-1, encoded by ABCC 8 - Chromosome 11) Kir 6. 2 (encoded by KCNJ 11 - Chromosome 11) Glutamate dehydrogenase (GDH; encoded by GLUD-1 Chromosome 10) Glucokinase (encoded by GCK- Chromosome 7)
ATP-sensitive potassium channel congenital hyperinsulinism Glucose SUR 1 Kir 6. 2 K+ GK VDCC ↑ATP/ADP GLUT 2 Insulin Amino Acids
ATP-sensitive potassium channel congenital hyperinsulinism The most common and severe form of CHI Ø More than 100 mutations of ABCC 8 and 20 mutations of KCNJ 11 have been found Ø Most reported mutations of ABCC 8 and KCNJ 11 are recessive; however, a few dominantly expressed mutations of ABCC 8 and one of KCNJ 11 have been reported Ø The dominant defects retain responsiveness to diazoxide and tend to be milder Ø
ATP-sensitive potassium channel congenital hyperinsulinism Ø Two histologic forms present: - Focal - Diffuse Ø Large for gestational age Ø Neonatal onset hypoglycemia Ø Unresponsive to diazoxide (usually) Ø Usually require pancreatectomy to control hypoglycemia.
Insulin secretion process SUR 1 Kir 6. 2 K+ Glucose GK Ca++ GLUT 2 Leucin ADP Krebs cycle + GTP Amino Acids VDCC ↑ATP/ADP a-ketoglutarate GDH Glutamate Insulin
Glutamate dehydrogenase hyperinsulinism a-ketoglutarate + NH 3 GDH Glutamate Liver cell
Glutamate dehydrogenase hyperinsulinism Normal glucose-stimulated insulin secretion. Ø Protein induced hypoglycemia Ø Fasting hypoglycemia Ø
Glutamate dehydrogenase hyperinsulinism The second-most-common form of CHI Ø Also known as the hyperinsulinism and hyperammonemia syndrome Ø
Glutamate dehydrogenase hyperinsulinism Ø Ø Ø Normal birth weight Hypoglycemia does not often manifest until later in infancy Recurrent episodes of fasting and postprandial hypoglycemia associated with persistent asymptomatic elevation of plasma ammonia levels Patients respond well to diazoxide Patients are instructed to avoid pure protein meals and to eat carbohydrates before protein
Glucokinase congenital hyperinsulinism Glucose SUR 1 Kir 6. 2 K+ GK VDCC ↑ATP/ADP Ca++ GLUT 2 Insulin Amino Acids
Glucokinase congenital hyperinsulinism Ø GK is expressed exclusively in the liver and pancreas Consider the B-Cell “glucosensor” Ø Activating mutations result in increased affinity of glucokinase for glucose and inappropriate secretion of insulin (Lower threshold for insulin secretion) Ø Diazoxide is usually effective Ø
OTHER FORMS OF HYPERINSULINISM IN NEONATES Perinatal stress-induced hyperinsulinism Birth asphyxia, maternal toxemia, prematurity, intrauterine growth retardation Ø Continuous feeding might be needed to maintain blood glucose Ø Usually resolve in 3 -4 months Ø
OTHER FORMS OF HYPERINSULINISM IN NEONATES Infant of the diabetic mother Ø Ø Ø Infant is exposed to hyperglycemia in utero Fetus up regulates insulin secretion macrosomia Glucagon deficiency may contribute to hypoglycemia in infant of a diabetic mother Hypoglycemia generally resolves within 2 days Responds to diazoxide, but generally not needed Usually treated with intravenous dextrose
OTHER FORMS OF HYPERINSULINISM IN NEONATES Beckwith–Wiedemann syndrome Characterized by somatic overgrowth, macroglossia, hemihypertrophy and transverse creases of the ear lobes, hypoglycemia, and predisposition to childhood tumors Ø Hypoglycemia occurs in up to 50% of patients with BWS Ø Diazoxide should be attempted Ø
Diazoxide Suppresses insulin secretion by maintaining the KATP channel in the open position Ø Dose 5 -15 mg/kg/day orally divided into 2 -3 doses Ø Response is evident in 48 hours Ø Side effects are 1. Primarily cosmetic - Hypertrichosis - Coarsening of the face 2. DKA 3. Fluid retention- particularly in preterm infants 4. Rarely leukopenia and thrombocytopenia Ø
Other Treatment Options Therapy Dosage Side effect Diazoxide 5 -15 mg/kg/day PO divided Q 8 Fluid retention Hypertrichosis Hyperglycemia Coarse facial features Leukopenia Octreotide 5 -40 mcg/kg/day SQ divided Q 4 -6 Tolerance Abdominal distention Steatorrhea Suppression of other hormones Calcium Channel blockers Nifedipine 0. 25 -0. 7 Hypotension mg/kg/day PO divided Q 8 No long term data
Summary Ø Ø Ø No consensus exists as to the optimal definition of hypoglycemia in newborns Transitional Hypoglycemia most closely resembles congenital hyperinsulinism There are many Genetic forms of Congenital Hyperinsulinemic Hypoglycemia - Diazoxide is the main treatment for most of them Other causes of hyperinsulinemic hypoglycemia include, infants of diabetic mothers, Beckwith-Wiedemann syndrome, congenital disorders of glycosylation Surgical intervention may be needed in case of failure of medical treatment
THANK YOU QUESTIONS