Metabolic encephalopathy Hyperglycemia hypoglycemia Diagnosis of hypoglycemia o

Metabolic encephalopathy Hyperglycemia/ hypoglycemia

Diagnosis of hypoglycemia o Hypoglycemia was defined by the Third International Symposium on Hypoglycemia is a blood glucose value of less than 50 mg/dl. Whipple’s triad: o Symptoms consistent with hypoglycemia o A low plasma glucose concentration o Relief of those symptoms.
 symptoms: sweating, hungry, tingling, shaky/tremulous, heart pounding,")
Symptoms of hypoglycemia o Neurogenic ( Autonomic) symptoms: sweating, hungry, tingling, shaky/tremulous, heart pounding, nervous/anxious o Neuroglycopenic symptoms: Weak, difficulty thinking/confused, tired/drowsy, faint, dizzy, difficulty speaking, blur vision o The manifestations of hypoglycemia are nonspecific, vary among individuals and may change from time to time in the same individual.

Clinical Classification of Hypoglycemia Fasting Hypoglycemia Drugs Especially insulin, sulfonylureas, alcohol, Also pentamidine, quinine Rarely, salicylates, sulfonamides Critical illnesses Hepatic failure Cardiac failure Renal failure Sepsis Inanition Hormonal deficiencies Cortisol or growth hormone, or both Glucagon and epinephrine Non-beta cell tumors Endogenous hyperisulinism Pancreatic beta cell disorders Tumor(insulinoma) Nontumor Beta cell secretagogue Autoimmune hypoglycemia Insulin antibodies Insulin receptor antibodies ?Bate cell antibodies ?Ectopic Insulin secretion Hypoglycemias of infancy and hildhood Reactive Hypoglycemia Congenital deficiencies of enzymes of carbohydrate metabolism Alimentary hypoglycemia Idiopathic(functional) postprandial hypoglycem
 Number/Mortality number 14/1 17. 95 % 4/3 7/0")
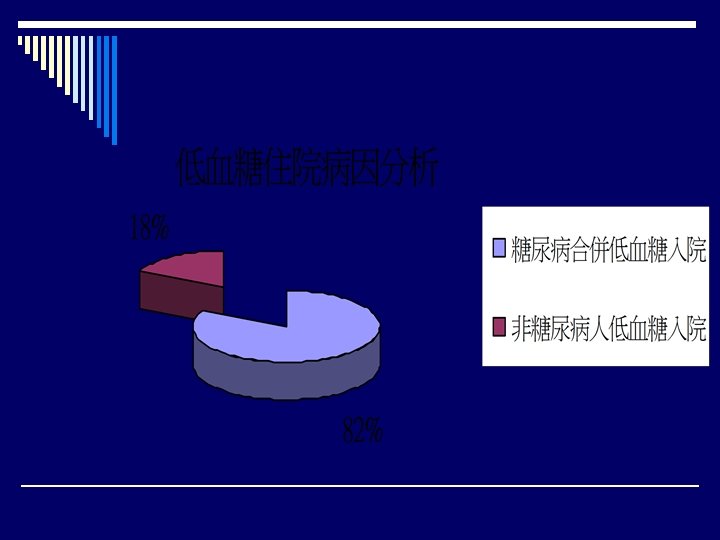
Classification of Hypoglycemia in Non-diabetes patients(1) Number/Mortality number 14/1 17. 95 % 4/3 7/0 1/0 6/6 12/1 3/3 12/0 5. 13 % 8. 97 % 1. 28 % 7. 69 % 15. 39 % 3. 85 % 15. 39 % Drugs Critical illnesses Hepatic failure Cardiac failure Renal failure Sepsis Inanition CPR Adrenal insufficiency
 Number/Mortality number Non-beta cell tumors HCC 7/7 Non-HCC")
Classification of Hypoglycemia in Non-diabetes patients(1) Number/Mortality number Non-beta cell tumors HCC 7/7 Non-HCC cancer 5/5 Pancreatic beta cell disorders Tumor(insulinoma) 1/0 Autoimmune hypoglycemia 2/0 Postprandial(Reactive) Hypoglycemia Functional postprandial hypoglycem 1/1 Unknown cause 3/0 Incidence(%) 8. 97 % 6. 4 1 % 1. 28 % 2. 56 % 1. 28 % 3. 85%
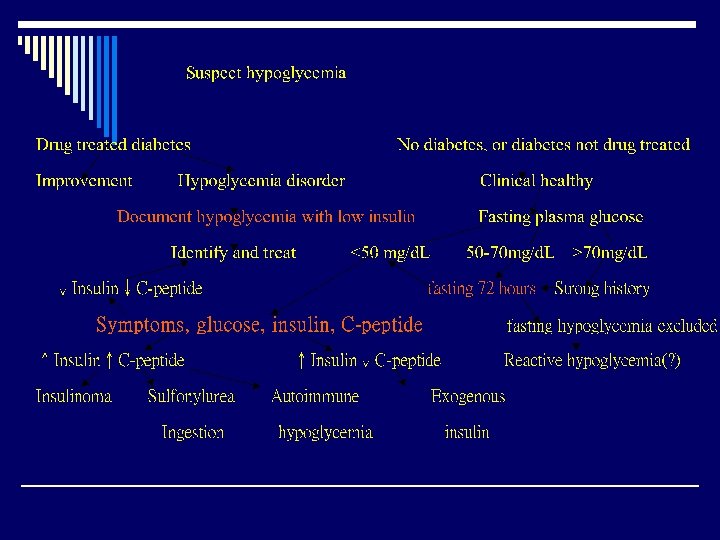

Laboratory tests in evaluation of hypoglycemia o Simultaneous measurement of fasting blood glucose and insulin levels during the occurrence of symptoms is the most laboratory tests. o Other potentially important tests include measurement of C-peptide, sulfonylurea levels, plasma cortisol, renal function, liver function and insulin antibody levels.

Comprehensive Risk Factors for Hypoglycemia in Diabetes Absolute or relative therapeutic agent excess a. Dose excessive, ill-timed, wrong type b. Decreased food intake c. Increased glucose utilization(e. g. , exercise) d. Decreased glucose production(e. g. , alcohol) e. Increased sensitivity to insulin(e. g. , after exercise, during the night, glycemic control, weight loss) f. Decreased insulin clearance(e. g. , renal failure) o Compromised glucose counterregulation Unawareness hypoglycemia o

Prevention of Recurrent Hypoglycemia in Non-diabetes o Offending drugs can be discontinues or their doses o o o reduced Underlying critical illnesses can be treated Cortisol can be replaced Surgical, radiotherapeutic, or chemotherapeutic reduction of a non-beta cell tumor, glucocorticoid administration may alleviate hypoglycemia in such patients. Surgical resection or medical therapy for insulinoma Failing these treatments=>frequent feedings or even overnight intragastic glucose infusion may be necessary

Hypoglycemia Risk Reduction in Diabetes o Addressing the issue of hypoglycemia in every contact with the patient o Applying the principles of aggressive glycemic therapy o Considering each of the comprehensive risk factors for hypoglycemia

病例一: history &PE o Past history: denied diabetes, hypertension, or other systemic disorder o Present illness: progressively dyspnea for 2 days, nausea and vomiting, epigastragia, poor appetite o P. E. : 上腹微微壓痛 o 接下來,你會怎麼想?
 o Arterial gas: PH: 7. 102, PCO 2:")
病例一: 分析並處置 o F/S: high (爆錶!) o Arterial gas: PH: 7. 102, PCO 2: 16 mm. Hg, PO 2: 98 mm. Hg, HCO 3: 8. 4 Na: 128, K: 5. 7, urine ketone: 3+ 病人是什麼問題? 如何處置呢?
 o DKA is typically characterized by hyperglycemia over 300 mg/d.")
病例一: Diabetic ketoacidosis (DKA) o DKA is typically characterized by hyperglycemia over 300 mg/d. L, low bicarbonate (<15 m. Eq/L), and acidosis (p. H <7. 30) with ketonemia and ketonuria. o Counterregulatory hormones, such as glucagon, growth hormone, and catecholamines, enhance triglyceride breakdown into free fatty acids and gluconeogenesis

病例一: Diabetic ketoacidosis o beta-oxidation of free fatty acids deplete extracellular and cellular acid buffers o hyperglycemia-induced osmotic diuresis depletes sodium, potassium, phosphates, and water as well as ketones and glucose

病例一: Diabetic ketoacidosis o Clinical manifestations; ü Thirst, polyuria, polydipsia, nocturia ü Generalized weakness, malaise/lethargy ü Nausea/vomiting ü Decreased perspiration ü Anorexia or increased appetite ü Confusion ü Fever ü Dysuria ü Chills ü Chest pain ü Abdominal pain ü Shortness of breath
, missed insulin treatments")
病例一: Diabetic ketoacidosis o 誘發因素: ü underlying or concomitant infection (40%), missed insulin treatments (25%), and newly diagnosed, previously unknown diabetes (15%). Other associated causes make up roughly 20% in the various series. ü AMI ü CVA ü Trauma ü Pregnancy ü Others

病例一: Diabetic ketoacidosis o Management: ü ü ü ABC stable Hydration Insulin 計算Na, K 的缺少和假象 Acidosis correct Monitor: ABG, sugar, Na, K, urine output

DKA management o Hydration: 1 -2 L normal saline /half saline challenge o Monitor urine output o NPO initially

DKA management o Insulin injection: ü ü ü Continuous infusion: 0. 1 u/kg/hr F/S sugar >600, injection insulin? 爭議 F/S sugar 多少時要注意?

Na 的計算 o Sodium: The osmotic effect of hyperglycemia moves extravascular water to the intravascular space. For each 100 mg/d. L of glucose over 100 mg/d. L, the serum sodium is lowered by approximately 1. 6 m. Eq/L. When glucose levels fall, the serum sodium will rise by a corresponding amount

K 的計算 o Potassium: This needs to be checked frequently, as values drop very rapidly with treatment. An ECG may be used to assess the cardiac effects of extremes in potassium levels

Na. HCO 3 的補充 o PH <7. 0 -7. 1 o HCO 3 < 10 meq/ml o Basis excess: negative, 補充一半 o Monitor

病例二: history and PE o DM history with oral hyperglycemic agents for 10 years o Malaise for 3 days o Fever was noted this morning o SOB without cough o P. E. : nothing special
 o Finger sting: high o BUN: 42, Cr: 1. 7,")
病例二: 檢查 (Lab data) o Finger sting: high o BUN: 42, Cr: 1. 7, Na: 120, K: 5. 2 o U/A: WBC >100/HPF o 你還想知道什麼?
 o Sugar control o Chest X-ray o ECG o Serum")
病例二: 檢查 (Lab data) o Sugar control o Chest X-ray o ECG o Serum WBC o Brain CT? o DM foot?
 o Definition: 一般sugar >250 mg/d. L, blood Osm.")
病例二: Hyperglycemic Hyperosmolar Nonketotic Coma (HHNK) o Definition: 一般sugar >250 mg/d. L, blood Osm. >320 o 你知道blood Osm. 如何算嗎? o 你知道coma的病人,如何快速找到原因嗎 ?
+sugar/18+BUN/2. 8 有何意義?")
病例二: HHNK o Calculated blood osm. : 2(Na+K)+sugar/18+BUN/2. 8 有何意義?

病例二: HHNK o Patient present with Conscious change ü 口訣: “AEIOU TIPS” ü 口訣: MODS ü 口訣: sugar-O 2 -opioate-thiamine (Tx: DONE-dextrose, O 2, naloxone, thiamine)

病例二: HHNK o Clinical manifestation ü ü Precipitating factors: vomiting with dehydration, AMI, infection… Neurologic deficits: drowsiness, delirium, coma, seizure, hemiparesis… tachycardia, tachypnea, hyponatremia, hyperkalemia… Hyperglycemia >600 mg/d. L

病例二: HHNK o Precipitating factors correct: infection, AMI… o Management: ü ü ü ABC 穩定 Hydration: 0. 5 -1 L Insulin infusion? Underlying disease treat Urine output monitor O 2, if necessary

Thank you for your attention!
- Slides: 39