Interpretasi hasil pemeriksaan skrining hemostasis Departemen Patologi Klinik











 vacuolisation Toxic granulation Leucocytosis : netrophilia absolute")


 : Abnormal/Prolonged (a) PPT>,")
 PPT N, APTT > Acquired - Deficiency /")

 - Severe liver disease")



- Slides: 25
Interpretasi hasil pemeriksaan skrining hemostasis Departemen Patologi Klinik UNTAD
LABORATORY RESULTS INTERPRETATION OF BLEEDING DISORDERS. Types of tests a. Screening tests for vascular & platelet disorders: Formation of initial platelet plugs 1. Platelet count 2. Bleeding Time 3. Examination of peripheral blood film 4. Tourniquet test
b. Screening test for coagulation disorders : Formation of fibrin 1. Prothrombin Time 2. Partial Activated Thromboplastin Time 3. Thrombin Time c. Special Test → after : * the patient’s history * physical examination * screening tests (a and b)
Include 1. Specific coagulation factor assays 2. Platelet function tests 3. Assay for von Willebrand’s Factor 4. tests for circulating inhibitor 5. tests for Disseminated Intravascular Coagulation (DIC) 6. tests for pathological fibrinolysis
TEST RESULT 1. a. Prolonged Bleeding time Normal Platelet count Normal PPT & APTT Vascular defect Clot retraction time Platelet Functional defect Platelet aggregation b. Prolonged Bleeding Time - Von Willebrand’s disease Normal Platelet Count Prolonged APTT - Von willebrand’s factor antigen - Platelet Aggregation test with Ristocetin
Platelet count, BT prolonged, PPT & APTT normal A. Hipoproliferative / Failure of marrow production Peripheral blood examination / CBC: Pancytopenia - Anemia ( - Hb, RBC count, Hct) WBC count Blood smear : Erythr : macrooval (oval macrocyt) & hypersegmentation neutrophil BMP : - megaloblast (specific morphological changes) - Giant metamyelocyt Ineffective Thrombopoiesis
CBC : Pancytopenia Low % reticulocyte → < 0, 5 % Blood Smear : Eryth : normocytic normochr (macrocytic) Diff. count : - relative lymphocytosis - netropenia/granulositopenia BMP : megakaryocyt mass Hypocelluler granulopoiesis Erythropoiesis Marrow : Lymphocytosis Aplasia / Hypoplasia of bone marrow
Peripheral Blood Cell measurement: - Anemia - WBC > Peripheral Blood Smear morphology: - normocytic normochromic anemia - Leucoerythroblastic blood picture → myelofibrosis & infiltr by other neoplasm/metastatic - Leukemia / Lymphoma/Myeloma cell - BMP examination : - Hipercelluler -Wide spectrum of BM morph abnormalities Bone Marrow Replacement disorder
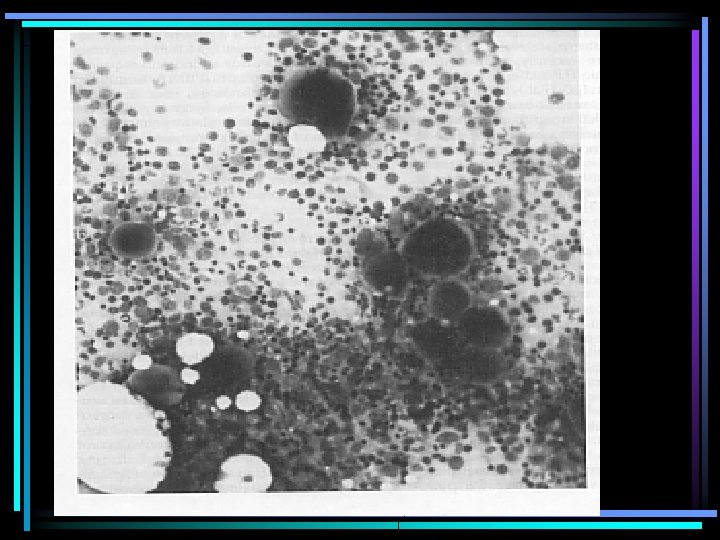
B. Increased Platelet Destruction A. Immune Thrombocytopenia Purpura Periph Blood Cell measurement / CBC - Anemia - WBC : depends on the causal Blood smear morphology : - ↓ platelet count (< 3 / HPF) -Abnormality of morph & size → Giant platelet (> 10 µm) - viral : atypical lymphocyte - Bacterial : left shifted of myeloid cells & features of neutrophil toxicity (granulation, vacuolization) Immune Thrombocy topenia
Sitoplasma basofilik LIMFOSIT PLASMA BIRU Sitoplasma basofilik
Limfosit Plasma Biru
Qualitative abnormality White blood cell (blood smear) vacuolisation Toxic granulation Leucocytosis : netrophilia absolute with toxic granulation & vacuolisation Bacterial infection
BMP : Normal or increased immature megakaryocytes characterized by : -Non budding / intact cytoplasm -More basophilic cytoplasm & decreased granularity -Hypoploidy of nuclei marrow normoblast : compensation of bleeding B. Non immun thrombocytopenia: DIC, HUS, TTP Screening test: detection of consumptive coagulation Confirmative test: detection of secondary fibrinolysis Peripheral blood examination: Erythrocyt fragmentation (helmet, trianguler, schistocyt)
Thrombocytopenia: Distribution abnormality • Peripheral blood examination: • Pancytopenia • splenic pooling/ • Reticulocytosis hypersplenism • BMP: normal/ hipercelluler
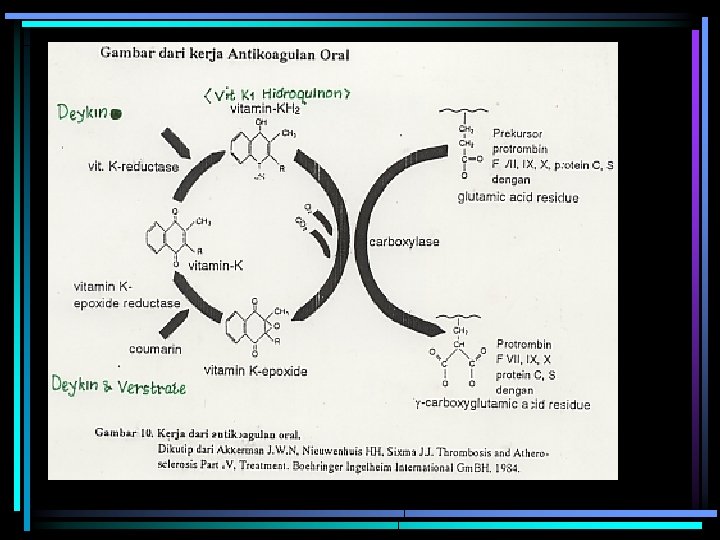
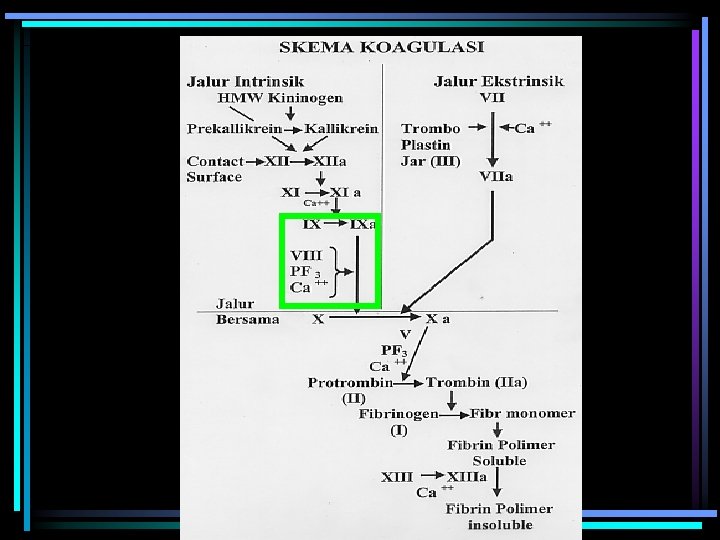
III. Platelet Count : Normal Coagulation tests (PPT & APTT) : Abnormal/Prolonged (a) PPT>, APTT N - Early oral Anticoagulant therapy: warfarin, coumarin - Congenital & acquired deficiency of F II, V, X - Early cirrhosis / chronic liver disease : PPT is more sensitive due to the shortest half life of F VII - Vit K deficiency - Circulating Inhibitor of extrinsic coagulation/clotting factor
III. Platelet Count : Normal (b) PPT N, APTT > Acquired - Deficiency / defect of intrinsic coagulation factor - Hemophilia: F VIII, F IX, F XII (herediter) Hemophilia - von Willebrand’s disease - Heparin anticoagulant therapy - spesific circulating Inhibitor of F VIII, Lupus anticoagulant / Lupus inhibitor
c. PPT >, APTT> * Def iciency of multiple coagulation factors → acquired * Liver disease : cholestasis * Vit K def (Factor II, VII, IX, X) * Primary fibrinolysis → [fibrinogen] ↓↓ * Rapid stored blood transfusion
IV. Platelet Count , prolonged coagulation test (PPT & APTT) - Severe liver disease : liver cirrhosis with portal hypertension → ↓ platelet count due to excessive splenic pooling / hipersplenisme. Thrombin Time: the most sensitive test for dysfibrinogenemia detection - Disseminated Intravascular Coagulation/DIC (Secondary Fibrinolysis) • Rapid stored blood transfusion
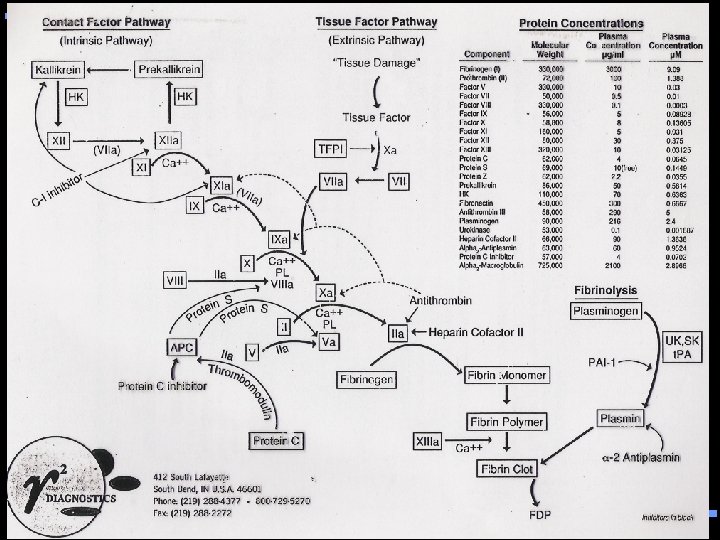
THROMBOTIC RISK FACTORS Genetic • Deficiency of protein C, protein S, and AT III • Activated protein C resistency (APC-R) • Serine proteinase inhibitor deficiency • Hyperfibrinogenemia, dysfibrinogenemia • Hyperhomocysteinemia • Fibrinolysis pathway abnormalities - Plasminogen - t. PA (Tissue Plasminogen Activator) deficiency- PAI-1 excess • Lipoprotein a / Lp(a)
• Acquired Anti-phospholipid antibody and lupus anticoagulant Hyperhomocysteinemia Lipid imbalance / Dyslipidemia
What Test to Perform • • • APC resistance Factor V Leiden mutation Protein C, S antigen and activity, free protein S Anti Thrombin III Thrombin time Serum homocystein Current thrombosis markers Test of fibrinolysis Profile of serum lipid