Inflammatory heart diseases in pediatrics Infective endocarditis rare






















 FIBRINOUS PERICARDITIS")




 • pericardiocenthesis +/ • purulent –")

")







 • systemic inflammatory")



- Slides: 45
Inflammatory heart diseases in pediatrics
Infective endocarditis • • rare disease affecting predominantly endocardium presence of vegetations incidence increases with age, rare in newborns most of cases in patients with aortic stenosis or cyanotic congenital heart defect vegetations on mitral valve vegetations on bicuspid aortic valve
Etiology • • • BAKTERIAL Staph. aureus Strep. viridans Strep. bovis Enteroc. faecalis HACEK Staph. epidermidis chlamydia, rickettsia Candida, Aspergillus
Clinical condition • non-specific symptoms – dominant - higher temperature, fatigue, loss of weight, night sweating, symptoms and signs of heart failure • valcular and immunologic signs (rare) - petechiae on skin and mucous membranes, splinter hemorrhages, Oslerov nodes, Janeway lesions, Roth spots, glomerulonephritis, arthralgias, myalgias • embolization - 30% of cases; qualitative and quantitative changes of mental state, abscesses of brain and spleen, kidney and lung infarction
painful Osler nodes non-painful Janeway lesions splinter hemorrhages
conjunctival petechiae spleen abscess Roth spots spleen abscess on MRI scan
kidney infarction ruptured brain vessel aneurysm brain abscess on CT brain vessel aneurysm
Diagnostics • clinical symptoms • laboratrory findings - anemia, leukocytosis, neutrofilia, elevated CRP, procalcitonin, AST, ALT, troponin and NTpro. BNP (elevated +/-), in severe heart failure increased amount of renal parameters • hemocultures – from peripheral vein; at least 2 -3 samples; don´t have to wait for temperature increase; before ATB treatment! aerobic (+/-anaerobic) cultivation • ECHO – vegetations, abcess, dehiscence of a prosthetic valve • modified Duke criteria – to set up a diagnosis of IE - 2 major clinical criteria, OR 1 major and 3 minor clinical criteria, OR 5 minor clinical criteria
Modified Duke criteria Major criteria Minor criteria • positive blood cultures for IE • – – Staphylococcus aureus Viridans streptococci Streptococcus gallolyticus HACEK group – intravenous drug use or presence of a predisposing heart condition • • fever vascular phenomena – major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, or Janeway lesions • echocardografic evidence of endocardial involvement – vegetation – abscess – new valvular regurgitation predisposition • immunologic phenomena – glomerulonephritis, Osler nodes, Roth spots, or rheumatoid factor • microbiologic evidence – positive blood cultures that do not meet major criteria
vegetations on aortic valve normal aortic valve
Treatment • conservative Ø ATB Ø baktericidal Ø strictly i. v. Ø longterm (4 -6 weeks) Ø different ATB protocols
Myocarditis a myopericarditis • • not so common mainly in adolescents and infants inflammation of 2 heart layers in many patients (but myocardial damage is more pronounced than pericardial) triphasic disease 1. infection and immune response 2. immune system tries to eliminate inf. agent (but because of molecular mimicry – viral and myocardial antigents are very similar - immune system destroys heart) 3. developement of dilated cardiomyopathy
Etiology • dominantly viral Ø enteroviruses – Coxackie B, echovirus Ø influenza, parainfluenza, adenovirus, parvovirus B 19 Ø CMV, EBV, VHC • bakterial Ø Borrelia
Clinical manifestation • from asymptomatic forms to symptoms of severe heart failure • commonly preceded by viral infection – GIT/respiratory (10 -14 days before) • chestpain • +/- symptoms of heart failure • arrhythmias
Diagnosis • clinical manifestation • laboratory findings– leukocytes and lymphocytes +/-, CRP low, procalcitonin negat. , elevation of AST, ALT, troponins, NTpro. BNP + direct (PCR) a indirect (serology) diagnostics of viruses • imaging techniques • biopsy ? ? ! – very rarely in children
infant with myocarditis and cardiomegaly
ECHOkg – dilation of heart chambers, bad function, low ejection fraction, hypokinesis, akinesis
MRI with gadolinium – signs of myocardial damage
low valtage, pathologically inverted T waves in II, III, a. VF, V 3 -6
Treatment • bed-rest • symptomatic treatment of acute and chronic heart failure • imunoglobulins +/-
Pericarditis • not so common • predominantely in adolescents
Etiology • dominantly viral – spectrum like in myocarditis • bacterial – purulent – most often secondary to hematogenous spread during other infections Ø S. aureus, H. influenzae Ø M. tuberculosis • postpericardiotomic syndrome – pericarditis due to open heart surgery (mechanical trauma)
Clinical manifestation • usually a sudden onset with a fever a. ) FIBRINOUS PERICARDITIS • retrosternal pain with radiation (shoulders, neck) • shortness of breath, cough (pleural involvement) • pericardial friction rub (disappers with increasing amount of pericardial effusion) b. ) EXSUDATIVE PERICARDITIS • Increasing shortness of breath • difficult palpation of heart apex beating • silent heart sounds • hepatomegaly, edemas
Cardiac tamponade • acute condition caused by rapidly increasing amount of pericardial effusion • limited diastolic filling of the heart • increased central venous pressure • decreased cardiac output and subsequent circulatory collapse Clinical manifestation • severe shortness of breath • jugular veins distension • tachycardia • hepatomegaly • pulsus paradoxus, hypotension with reduction in systolic-diastolic difference !!! • sudden death !!!
Diagnostics • clinical symptoms • laboratory findings - leukocytosis, neutrofilia, elevated CRP, only slightly AST, ALT, troponin and NTpro. BNP +/- direct and indirect dg. of viruses – not necessary in mild cases • imaging techniques
difuse ST elevation – I, III, a. VF, V 5 -6 ECG evolving in pericarditis
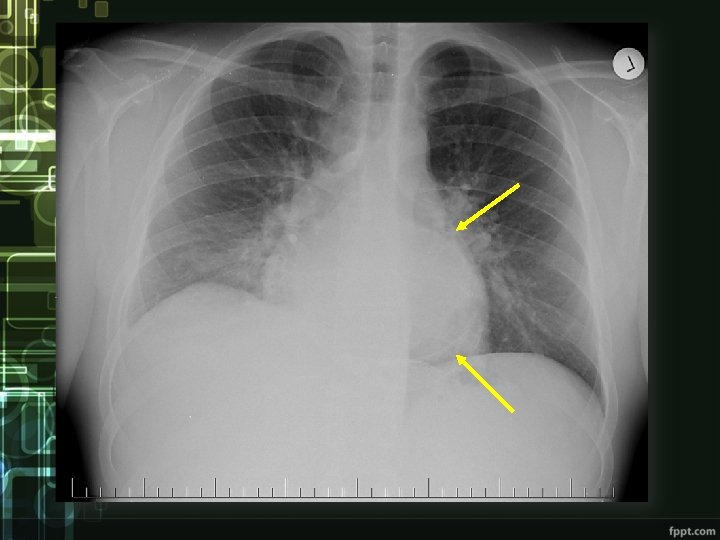
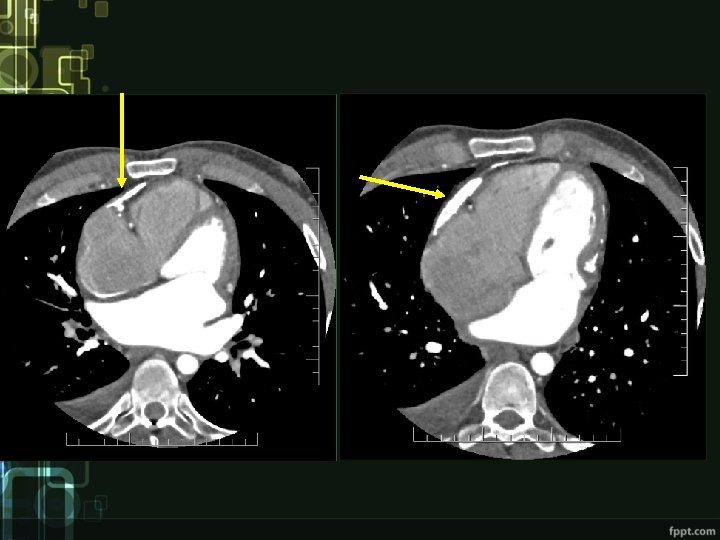
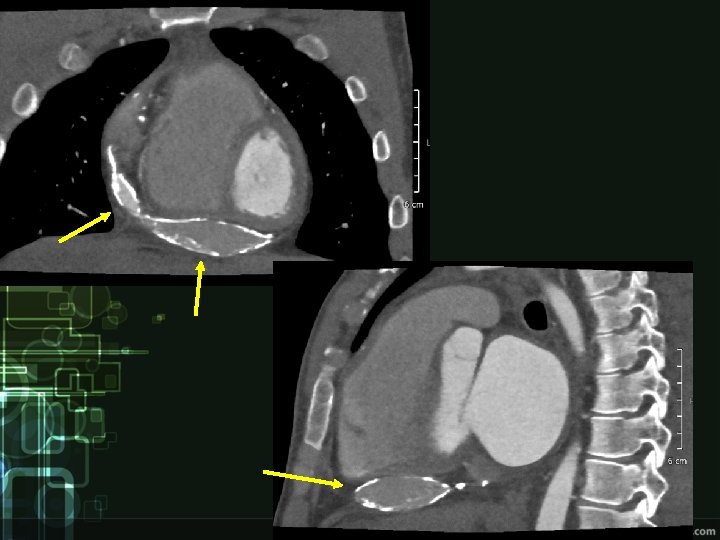
cardiac tamponade
Treatment • bed rest • anti-inflammatory drugs (nonsteroidal) • pericardiocenthesis +/ • purulent – sur. drainage, ATB
Constrictive pericarditis • extremly rare complication • Etiology - previous inflammation of the pericardium (TBC, others) - after traumatic hemopericardium - after cardiac surgery • Hemodynamics - limited filling of the heart in rigid pericardium • Clinical manifestation - exertional dyspnea - weakness, fatique - edema - chest pain, sometimes syncope
Diagnostics • Clinical picture • ECG – low voltage, repolarization changes (inverted T waves) • ECHO – thickened pericardium, impaired ventricular filling, „dancing septum“, IVC and atrial dilatation • Other imaging techniques
Treatment • pericardiectomy
Kawasaki disease • inflammatory disease of unknown etiology • mainly in small children • 25% of patients have cardiac complications • good prognosis (except those with persistent cardiac complications)
Clinical manifestation • Acute phase Ø high fever 39 °C, at least 5 days not responding to ATB and antipyretics Ø bilateral conjunctivitis Ø red swollen lips, strawberry tongue, diffuse erythema of oropharyngeal mucosa, cracking and dryness of lips Ø edema and erythema of palms and soles Ø polymorphic rash on trunk Ø unilateral cervical lymphadenopathy Ø myocarditis, pericarditis • Subacute phase Ø desquamating leasion, temperature drop, coronary aneurysms • Reconvalescent phase Ø disappearance of symptoms
Diagnostics • clinical manifestation • laboratory findings Ø leukocytosis, elevated CRP, ALT, hypoalbuminemia, Ø leukocyturia • imaging techniques Ø ECG, ECHO, angiography +/ • exclude infections! – hemocultures, urine, X-ray, otoskopy
aneurysms of left coronary artery and their reduction in 1 year
Treatment • imunoglobulins in high doses as soon as possible! • acetylsalicylic acid • +/- anticoagulation (only in severe aneurysms)
Paediatric multisystem inflammatory syndrome in timely relation to SARSCo. V-2 (PIMS-TS/MIC-C) • systemic inflammatory disease of unknown etiology • first appearance in spring 2020, time relation to the first wave of the COVID-19 pandemic • similar to kawasaki disease, frequent development of cardiogenic shock!!
Clinical features and diagnosis • pediatric population • persistent fever • laboratory evidence of inflammation, with no other obvious cause • multisystem involvement (2 or more) • evidence of SARS-Co. V-2 infection • myocardial dysfunction, rash, coagulopathy, GI problems. . .
Therapy • high-dose immunoglobulin therapy! • venous thromboembolism prophylaxis – LMWH • antiplatelet therapy – ASA • antibiotics – if infection can not be excluded !! transmission to ICU and administration of inotropic agents if cardiac shock develops !!
Questions • • Characterise endocarditis, prevalence, etiology, clinical manifestation, diagnostics and treatment. Characterise myocarditis, prevalence, etiology, clinical manifestation, diagnostics and treatment. Characterise pericarditis, prevalence, etiology, clinical manifestation, diagnostics and treatment. Characterise Kawasaki disease, prevalence, clinical manifestation, diagnostics and treatment.