Endometriosis Jolanta Zegarska Chair and Clinic of Obstetrics

Endometriosis Jolanta Zegarska Chair and Clinic of Obstetrics, Gynecological Diseases and Oncological Gynecology Collegium Medicum in Bydgoszcz Nicolaus Copernicus University in Torun
 outside its")
Endometriosis • Occurrence of the cells of uterine mucosa (glandular and stromal) outside its natural localization • Functionally corresponds to the endometrium • Estrogen-dependent • Occurs in 5– 15% total population of women – mainly in women of child-bearing potential
")
Endometriosis—pathogenesis • First reports date back to 1600 B. C. (Egyptian reports on papyrus) • Until 1920's, endometriosis was considered as a benign hyperplasia appearing under different names: cystadenoma, cystic fibrosis, adenomyoma • Sampson (1927): the term “endometriosis” and “retrograde menstruation” — ectopic implantation of live endometrial fragments

Endometriosis—pathogenesis • Recklinghausen Cullen Iwanhofen Meyer into 1885 1896 1898 1903 - proinflammatory factors, Pick 1905 Sampson 1922 Halban 1924 Navrital & Kramer Mc Weigh 1955 Weed et al. 1980 from the Wolffian ducts, from the Müllerian ducts, metaplasia of peritoneal epithelium, as above, invagination of epithelium submucosa; inducers: hormones, as above, affects germinal epithelium of the ovary, “retrograde menstruation”, hyperplasia of lymphatic ducts , 1936 - vascular hyperplasia , from the corona radiata cells around oocyte, failure of immune system originating from the Müllerian ducts,
 and induction (1955) •")
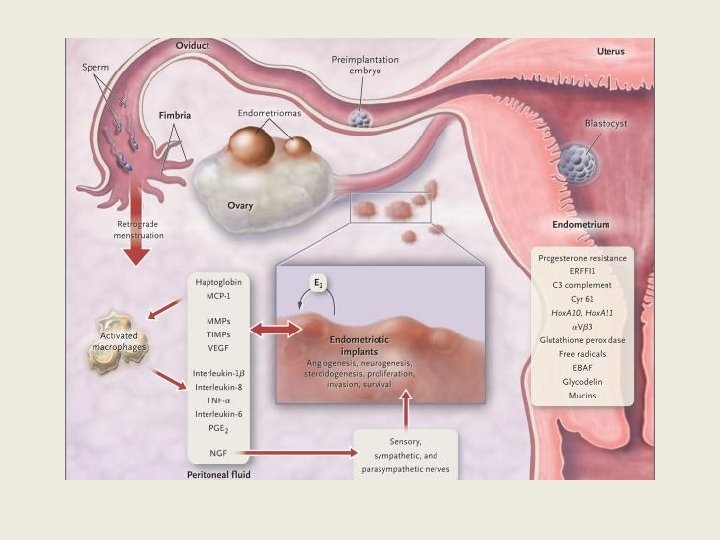
Endometriosis—pathogenesis • Implantation theory coexists with theories of metaplasia (1870) and induction (1955) • Since early 1980 s, it is known that menstrual blood reflux occurs in nearly all women of child-bearing potential • Therefore, mechanisms preventing implantation are sought • Cellular and humoral immunity are crucial for the pathogenesis of endometriosis

Endometriosis—pathogenesis • • Genetic predispositions Immune system dysfunction Environmental influence Mental, emotional and personalityrelated factors may be relevant
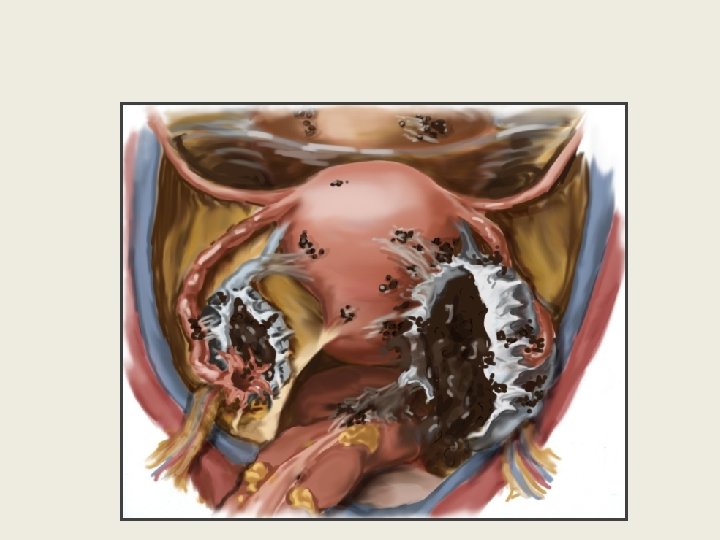

Endometriosis Three types of endometriosis have been characterised Peritoneal Ovarian Deep infiltrating

Diagnostics • Anamnesis • Physical examination • Diagnostic imaging

Symptoms • • Lower abdominal pain Painful menstruation Abundant menstruation Dysuria Dyspareunia Pain in sacrum area Diarrhoea during menstruation Constipation, tympanites

Less typical symptoms • Recurring sciatic-type limb pain • Recurring rectal bleeding • Recurring bleeding from urinary tract

Less typical symptoms • Often diagnosed accidentally – During surgeries – Reduced fertility!

Physical examination • Palpation of adnexal area may reveal pathological resistance—endometrial cysts

Physical examination • Transvaginal and transrectal examinations help to examine uterosacral and rectovaginal septum ligaments, the locations of endometriotic nodules • Performed during menstruation increases the likelihood of finding foci of deep infiltrating endometriosis
 • During a speculum examination, lesions pathognomonic of endometriosis are")
Deep infiltrating endometriosis (DIE) • During a speculum examination, lesions pathognomonic of endometriosis are first sought Cyanotic foci located at 1/3 of upper rear vaginal wall

Endometriosis seen in the rear vaginal fornix
 • Palpation of vaginal walls usually reveals nodular lesions, •")
Deep infiltrating endometriosis (DIE) • Palpation of vaginal walls usually reveals nodular lesions, • painful infiltration of – uterosacral ligaments, – vesicouterine pouch – Douglas's sinus • Finding these lesions is not necessary for a full diagnosis of DIE

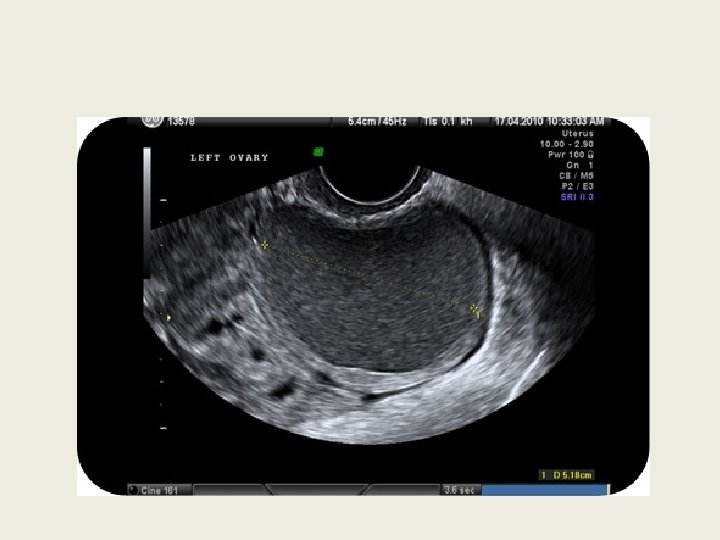
Endometrial cysts • In adnexal area: tissue resistance and tenderness • Normal ovaries are not always palpable • Endometrial cysts are often accompanied by tissue adhesions and thickening in adnexal area

Diagnostic imaging • Transabdominal and transvaginal ultrasound examinations are the primary diagnostic tools for detecting nodular lesions of the adnexa and for the evaluation of other pelvis minor structures

Diagnostic imaging • Magnetic Resonance Imaging shows high specificity in diagnosing endometrial cysts • Computed Tomography is not a standard method of the diagnostics of endometrial cysts
 • Surgical procedure is of particular importance • For the")
Deep infiltrating endometriosis (DIE) • Surgical procedure is of particular importance • For the proper and effective procedure, it is necessary to establish a map of existing pathological lesions using various imaging methods

Diagnosis • Suspected based on clinical signs and history • Confirmed using US and MRI
 • MRI – thorough simultaneous evaluation of front and rear")
Deep infiltrating endometriosis (DIE) • MRI – thorough simultaneous evaluation of front and rear pelvic areas – a map of all occurring DIE foci can be established • Transrectal Ultrasonography (TRUS) – accurate evaluation of the depth of endometriosis infiltration of the colorectal wall

TRUS—indications – functional disorders of the intestines – pain recurring during menstruation – incidents of lower gastrointestinal bleeding – suspected lesions in colorectal wall – large focal lesion near the rear vaginal fornix (diameter ≥ 3 cm)
 • Double-contrast colorectal imaging: lesions covering the front wall of")
Deep infiltrating endometriosis (DIE) • Double-contrast colorectal imaging: lesions covering the front wall of the large intestine, impaired spatial structure of surrounding tissues • When the lateral areas of pelvis minor are affected by DIE: urography • When foci in the urinary bladder are suspected: cystoscopy

Laparoscopy • Gold standard in the diagnostics of endometriosis – The only exception to this rule is the presence of endometriotic foci visualized during speculum examination of the vagina • Histopathological examination is recommended for all collected or excised tissues for a clear diagnosis

Laparoscopy—indication • Patients with pelvic pain: – suffering from • • dyspareunia painful menstruation dyschezia chronic pain Patients whose quality of life deteriorates and in whom pharmacological treatment is ineffective or contraindicated

Laparoscopy—indication • Patients with a suspected acute condition, e. g. , adnexal torsion or adnexal cyst rupture • Patients with suspected endometriotic infiltration of – intestines – urinary bladder – ureters – pelvic area nerves

Laparoscopy—indication • Patients with painful nodules on the uterosacral ligaments detected during gynaecological examination • Patients with diagnosed nodular lesions of the adnexa • Patients with infertility and no pathological lesions detected during gynaecological examination and additional imaging examinations

Noninvasive diagnostics • Concentrations of the glycoproteins Ca 125 and Ca 19 -9 • do not provide definitive answers but help in making decisions and targeting further procedures, therefore remain a recommended complementary tool

Conservative treatment • Reduction or elimination of pain • Inhibition of further development and regression of endometrial foci • Restoration of fertility

Conservative treatment • Possibility of starting pharmacological treatment of endometriosis only based on the clinical image without the need to confirm the disease in a laparoscopic examination (empiric therapy)

Conservative treatment • May be used as preparation for surgery • Complementary procedure in the postoperative period • Best therapeutic effects are achieved by combining surgical and pharmacological treatment

Conservative treatment Estrogen–progestogen products oral progestogen products depot progestogen products intrauterine device releasing progestogen • Gn. RH agonists • danazol • •

Conservative treatment • The efficacy of these drug groups is similar • Differences occur in the severity and type of adverse effects resulting from hypooestrogenism • Emerging Gn. Rh-related adverse effects limit therapy to six months
 – oestrogen–progestogen products –")
Conservative treatment • First-line medications: – Nonsteroidal antiinflammatory drugs (NSAIDs) – oestrogen–progestogen products – progestogen products

Conservative treatment ? ? ? • Nonsteroidal antiinflammatory drugs – inhibit prostaglandin synthesis – contribute to the reduction of inflammation – contribute to the reduction of pain • Complex oestrogen-progestogen therapy may be used periodically or continuously • Progestogens are given orally or as hormonal intrauterine system

Conservative treatment • Dienogest is a new drug with endometriosis as an authorized indication, administered orally at 2 mg/day • Exhibits selective activity of – 19 -nortestosterone and progesterone

Conservative treatment • Danazol, due to its numerous adverse effects: body weight gain, acne, seborrhoea, hirsutism, atrophic vaginitis, hot flushes, lowered libido, virilism, change in voice pitch, negative impact on lipid profile, • is currently used only occasionally

Surgical treatment • Indications for the surgical treatment of endometriosis: – Pain in the pelvis minor area – Infertility in endometriosis – Deep infiltrating endometriosis – Endometrial cysts of the ovaries

Surgical treatment • Conservative – In adolescent patients and women of child -bearing potential planning pregnancy • Radical – In patients not planning pregnancy or those with persisting pain despite appropriate pharmacotherapy – Intended to induce surgical menopause following bilateral ovariectomy

Surgical/conservative treatment • Release of adhesions, particularly periovarian and peritubal • Resection or ablation of endometriotic foci • Removal of endometrial cysts • Resection of endometriotic foci in adjacent organs Ablation of endometriotic lesions can be performed using electrodiathermy or laser

Surgical treatment • The recommended operating technique in the treatment of endometriosis, irrespective of the degree of the disease, is laparoscopy

Surgical treatment—DIE • The primary method of DIE treatment is radical resection of endometriotic foci. • This may require the resection of – uterosacral ligaments – upper rear vaginal wall – part of urinary bladder wall – segment of the intestine

Surgical treatment—DIE • It is not recommended to resect foci of DIE detected in diagnostic laparoscopy • In such cases, it is required to perform full preoperative diagnostics and obtain the patient's written consent for the necessary enhancement of surgical procedures, e. g. , partial resection of urinary bladder wall or intestine

Surgical treatment—cysts • Often coexist with advanced endometriosis. • When planning treatment, patient's plans regarding reproduction need to be considered • This is related with surgical procedures maximally sparing the ovary and/or fallopian tube structure

Surgical treatment—cysts • Complete resection of endometrial cyst increases fertility • Reduces risk of – recurrence of the disease – painful menstruation – dyspareunia – pain in the pelvis minor area – reoperation

Surgical treatment—cysts • Resection of endometrial cyst may also involve unintentional resection of normal ovarian structures and thus reduction of “ovarian reserve” • It is recommended to resect endometrial cysts greater than 3 cm in diameter

Surgical treatment—cysts • Recurrence of endometrial cysts after laparoscopic resection reveal in 30% patients • Postoperative hormonal suppression reduces the risk of recurrence and helps to reduce the severity of symptoms of endometriosis

Endometriosis—infertility • Pregnancy rate in healthy couples: 15– 20 %/month • Pregnancy rate in untreated women with endometriosis: 2– 10% • There is no clear mechanism explaining the link between endometriosis and infertility but several hypotheses and mechanisms are considered

Endometriosis Confirmed fertility Treatment for infertility Incidence of endometriosis 5– 10% ~50% Pregnancy rate 15– 20% 2– 10%

Endometriosis • 25– 50% women treated for infertility have endometriosis • 30– 50% women with endometriosis have problems with fertility

Endometriosis—infertility • Adhesions and altered anatomical structure of pelvis minor • Disrupted function of the peritoneum – Increased amount of fluid in the peritoneal cavity – Increased concentration of prostaglandins, proteases, cytokines (IL-1, IL-6, TNF-α), proangiogenic cytokines (IL-8) and VEGF • Increased concentration of proinflammatory cytokines in the blood serum of women with endometriosis – Generalized inflammation?

Endometriosis—infertility • Altered functions of hormones and mediators – Levels of Ig. G and Ig. A antibodies and lymphocytes are increased in the endometrium of women with endometriosis (alters endometrial function and impairs implantation) – Antiendometrial antibodies are produced

Endometriosis—infertility • Ovulatory and endocrine disorders – Unruptured Follicle Syndrome – Luteal Phase Defect – Disrupted follicle growth – Premature and multiple LH peaks – Follicular phase may be longer with lower oestradiol levels in blood serum and lower LH-dependent progesterone secretion in the second phase of the cycle • Incorrect implantation

Endometriosis—infertility • Follicle disturbances • Poor quality of oocytes and thus disturbed embryogenesis • Impaired endometrial receptivity • Impaired fallopian transport

Surgical treatment • Operator experience is important • Involvement of the ureter – 5% cases: hydronephrosis – 18% cases: ureter damage • Late complications – Intestine perforation – Rectovaginal and uretrovaginal fistulae

Infertility • Impact of deep endometriosis of infertility has never been proved • Dubious effect of inflammation in pelvis minor • Very often coexists with peritoneal endometriosis • Few articles comparing the impact of potential treatment on improving fertility are available

Endometriosis— contraception • Endometriosis was diagnosed more often in patients using OC in the past • When the reason for using contraception was severe primary dysmenorrhoea, DIE was diagnosed more frequently • Using OC in the past due to dysmenorrhoea may be considered as a marker of endometriosis, especially DIE Chapron C. Hum Reprod 2011

Thank you for your attention
- Slides: 62