CASE STUDY 44 Facilitator Pawin Puapornpong Past History




 V/S BT 37°C RR 20 /min BP 123/84 mm. Hg PR")


 • 1) Work up • Transabdominal ultrasound DDx fetal anomaly •")
 10/10/58 ทองแขงถเทาๆเดม ลกดนด uterine contraction: 4 min, 40 second, moderate to")




 Evaluated fetus • Fetal heart rate monitoring • Transabdominal ultrasound •")
 • Singleton fetus, intrauterine pregnancy • Cephalic presentation, EFW 1444 gm (<Percentile")
 • Placenta: posterior middle, grade II, no placenta previa • No venticulomegaly")

 S: ตนด ไมมไข นำนมไหลนอย ไมมคดตงเตานม นำคาวปลาจางลงและปรมาณลดลง 1 padไมชม กนขาวไดตามปกต ปวดแผลลดลง")



- Slides: 26
CASE STUDY 44 Facilitator: Pawin Puapornpong
Past History • No underlying disease • No history of drug, food allergy • No history of smoking, alcoholism • Current medication : none
Obstetric and Gynaecologic history • LMP 20/02/58 • PMP regular • No history of abortion • No history of PAP smear • G 1 P 0 GA 33⁺² wk by LMP • ANC รพ. นครนายก ทงหมด 7 ครง • First ANC GA 11⁺¹ wk by LMP • First Ultrasound at 6/07/58, GA 19⁺² wk by LMP • ANC risk: 1) Teenage pregnancy
Obstetric and Gynaecologic history • ANC Laboratory • Female • Male Hematocrit 34% DCIP negative OF negative Blood group A, Rh+ Anti HIV negative VDRL nonreactive HBs. Ag negative DCIP negative Anti HIV negative OF negative Blood group B, Rh+ • None couple at risk for severe thalassemia*
Physical Examination(รพ. นครนายก) V/S BT 37°C RR 20 /min BP 123/84 mm. Hg PR 116 bpm GA : A Thai pregnant woman, good consciousness HEENT : Not pale conjunctiva, anicteric sclerae Heart : Regular rhythm, normal S 1 S 2, no murmur Lung : Equal breath sounds, no crepitation both lungs Abdomen : Fundal height 3/4 > umbilicus, large part at left side longitudinal lie, cephalic presentation, engaged, fetal movement positive, fetal heart sound positive Uterine contraction: interval 4 min, regular duration 50 second, moderate intensity
Physical Examination • Extremities : no edema, no petechiae • CNS : E 1 M 1 V 1, pupil 3 mm RTLBE • Pelvic examination : cervical dilatation 3 cm, effacement 50%, station 0, membrane intact
Diagnosis • G 1 P 0 33+1 wk by LMP with • Preterm labor pain • Fetal anomaly • Teenage pregnancy
Management (รพ. นครนายก) • 1) Work up • Transabdominal ultrasound DDx fetal anomaly • Work up infection • 2) Promoted lung maturity : : Dexametrasone 12 mg IM q 12 hr x 2 dose (ครบ 9/10/58) • 3) Tocolytic agent : : Bricanyl 5 mg + 5%DW 1000 ml iv drip 40 ml/hr (3. 3 mcg/min) มใจสน , maternal HR 116 -126 bpm fetal heart rate 160 -165 bpm
Management (รพ. นครนายก) 10/10/58 ทองแขงถเทาๆเดม ลกดนด uterine contraction: 4 min, 40 second, moderate to strong intensity PV cervical os dilatation 4 cm, effacement 80%, station 0 1) พจารณาเรอง tocolytic agent เนองจากไดรบ dexamethasone ครบ 2) GBS prophylaxis : : Ampicillin 2 gm iv stat then 1 gm iv q 4 hr Refer to MSMC
REFER TO MSMC 11/10/58
Reevaluation at MSMC • 11/10/58, 12. 35 น. • ใจสน ไมมคลนไสอาเจยน ทองแขงมากขน ไมมมกเลอด ไมมนำเดน ลกดนปกตด • V/S BT 37. 2°C RR 20 /min BP 128/73 mm. Hg PR 124 bpm Abdomen : Fundal height 3/4 > umbilicus, large part at left side longitudinal lie, cephalic presentation, engaged, estimate fetal weight 1, 500 gm, fetal movement positive, fetal heart sound positive by doppler Uterine contraction: interval 4 min, duration 50 second, moderate intensity • Pelvic examination(12. 45น. ) : cervical dilatation 4 cm, effacement 50%, station 1+, soft consistency, posterior position, membrane intact
Diagnosis • G 1 P 0 33+1 wk by LMP with • Preterm labor pain • Fetal anomaly • Teenage pregnancy
Differential Diagnosis
Management • 1) Evaluated fetus • Fetal heart rate monitoring • Transabdominal ultrasound • 2) Evaluated maternal comorbidity : : side effect, infection • 3) Continue GBS prophylaxis: : Ampicillin 1 gm iv q 4 hr • 4) Expectant management for progression of labor
Transabdominal ultrasound(11/10/58) • Singleton fetus, intrauterine pregnancy • Cephalic presentation, EFW 1444 gm (<Percentile 5, reference จฬา ) • BPD 75. 5 mm/ 29+6 wk • HC 273 mm/ 29+4 wk • AC 251. 0 mm/ 29+2 wk • FL 55. 8 mm/ 29+3 wk • Fetal movement: positive, fetal cardiac activity: positive • AFI: 14. 2 cm
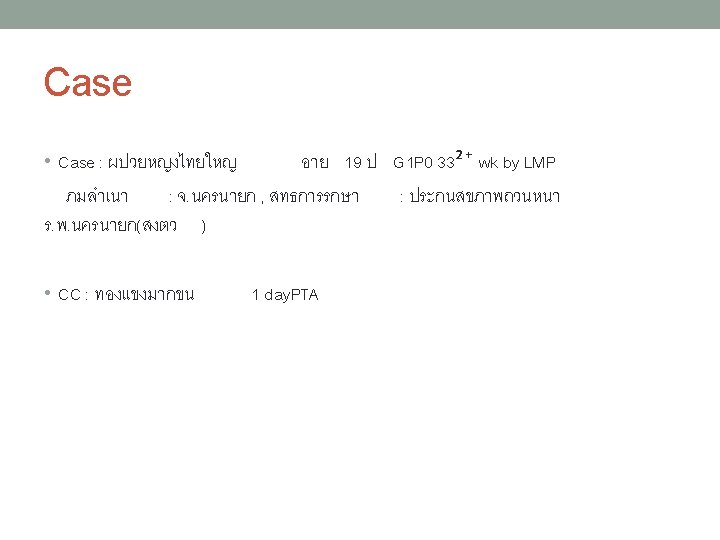
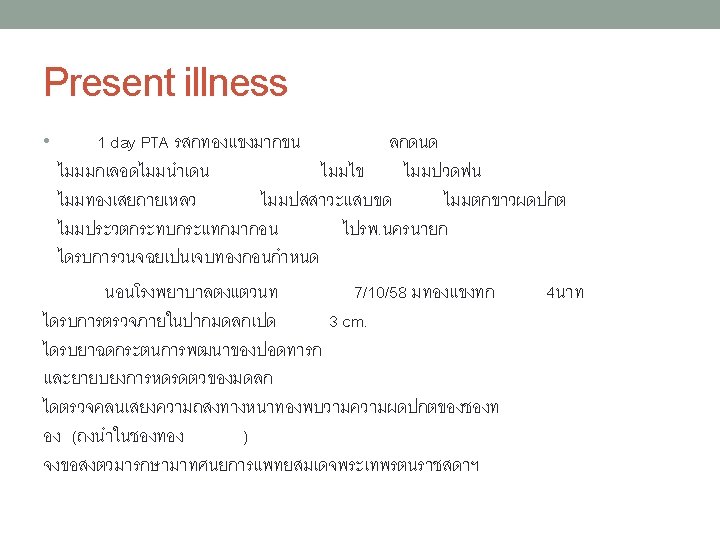
Transabdominal ultrasound(11/10/58) • Placenta: posterior middle, grade II, no placenta previa • No venticulomegaly • No cleft lips • Four cardiac chamber, not clearly seen LVOT, RVOT due to fetal position • Abdominal wall defect 2 cm, no liver protrude suspected gastroschisis • Seen both kidney, bladder
Progression of labor 11/10/58 Time Uterine contraction PV Management 12. 45 I 6 min 30 sec, D 30 sec, moderate intensity 4 cm, 100%, 1+, MI Expectant management and matero -fetal monitoring 14. 45 I 3 min 30 sec, D 30 sec, moderate intensity 5 cm, 100%, 1+, MI Expectant management 15. 40 I 3 min, D 40 sec, moderate intensity Fully dilate spontenous membrance rupture, thick meconium 15. 48 16. 20 Second degree Rt. episiotomy wound NL, term male NB, BBW 1, 670 gm(P 10), APGAR 4, 10 Nonvigorous child direct tracheal suction x 2 time transfer to NICU EBL 600 ml Hct 31% #PPH, due to uterine atony methergin, uterine massage
Progress note (12 -13/10/58) S: ตนด ไมมไข นำนมไหลนอย ไมมคดตงเตานม นำคาวปลาจางลงและปรมาณลดลง 1 padไมชม กนขาวไดตามปกต ปวดแผลลดลง O: v/s BT 36. 5 -37. 0°C RR 20/min BP 100 -110/60 mm. Hg, PR 80 -90 bpm CVS & Lung : WNL Abdomen : Fundal height at umbilicus, good uterine contraction, soft, not tender Perineum : Good wound healing A: # Postpatum normal labor with preterm delivery with fetal gastrochisis # Post PPH due to uterine atony clinical stable
Gastroschisis • Full thickness abdominal wall • Incidence 1: 20, 00 -40, 000 • Imaging – multiple loop of bowel are seen floating free in amniotic fluid (typical cauliflower appearance) - located in right umbilical cord - dilated loop of bowel in late pregnancy • Associated: : Associated Duodenum atresia, FGR • DDx - Rupture omphalocele - Umbilical cord cyst - Urachal cyst - Bladder or cloacal extrophy
• Antepartum monitor dilate - serial USG: : Fetal growth, Amniotic fluid, Bowel - MCA Doppler - Fetal echodiagram - GA 32 -34 wk NST, BPP q 2 time/wk - consult prenatal Ped and Sx • Delivery - Tertiary care hospital - C/S - - OB indication • Prognosis - survival rate 90% in uncomplicated dz - m/c NICU 30 day - NEC 4 -10%, dysfunction bowel 50%