Cardiovascular Emergencies Amy Gutman MD Amy Gutmanuc edu



 is the #1 cause of death in developed")








")

 perfuses right ventricle / inferior wall n Left")




, V 3, V 4 n Septum & anterior left")





 in I, a. VL, V 1 -V 5 with reciprocal changes")



 n BSI / PPE n Place patient in a")




 showed the availability of AEDs")





 n Emergency bypass surgery for MI less common then")
 n Primary PCI restores flow in 95% of patients")











 forms around atherosclerotic plaques n Since blockage of")















- Slides: 70
Cardiovascular Emergencies Amy Gutman MD Amy. Gutman@uc. edu
Overview n Myocardial Infarction n Stroke
Myocardial Infarction n Blood supply to heart muscle interrupted usually due to occlusion of a coronary artery following fatty plaque rupture n Lack of blood = lack of oxygen n STEMI (ST Segment Elevation MI) is ongoing ischemic damage to the heart muscle from a blocked artery causing a significant change in electrical delivery & positive enzymes n NSTEMI (Non-ST Elevation MI) is recent, mild ischemic damage to the heart muscle not significantly changing an electical pattern with +/- enzymes – Tissue hypoxia = “ischemia” – Tissue death = “infarction”
Epidemiology n Coronary artery disease (CAD) is the #1 cause of death in developed countries – #3 rd to AIDS & respiratory infections in developing countries n In the US: – – – 1 in 5 deaths 7, 200, 000 men & 6, 000 women have CAD 1, 200, 000 people suffer a an MI annually 40% die as a result of the attack within 90 days Every 65 secs, an American dies of a coronary event
Risk Factors n Cardiovascular disease n Older age – Men >40 – Women >50 n Tobacco smoking n High lipids (triglycerides, LDLs) & low HDLs n Diabetes n HTN n Obesity n Kidney disease n CHF n Excessive alcohol consumption n Cocaine / stimulant usage n Chronic high stress levels n Male gender
Socioeconomic & Genetic Risk Factors n Shorter education n Inflammatary diseases n Lower income (particularly in women) n Periodontal disease n Baldness & hair greying n Diagonal earlobe crease n Living with a partner n Birth control pills n Nicotine usage
Triggers n Intense psychological or physical exertion n Intense exercise & subsequent recovery associated with a 6 x higher MI rate for people who are physically very fit – For those in poor condition, the rate is 35 x higher n Increased incidence in the morning hours (0300 -0600) – – – Cortisol spike Increased platelet aggregation Increased inflammation
Symptoms n “Angina” is most common – Sensation of tightness, pressure, or squeezing – Radiates & may mimic heartburn n Dyspnea occurs when heart damage limits cardiac output causing heart failure & pulmonary edema n Loss of consciousness due to inadequate cerebral perfusion or cardiogenic shock n Other ssx from nervous system catecholamine surge – Diaphoresis – Weakness – Vertigo – Palpitations
Atypical Symptoms n Women & geriatrics often experience atypical symptoms n The most common symptoms of MI in women include dyspnea, insomnia & fatigue – “Angina” less predictive of ischemia than in men – 50% experience warning ssx prior to infarction, often weeks earlier n 25% of all MIs are “silent” – Discovered later on ECG or at autopsy – Common in the elderly, diabetes, post heart transplantation
Differential Diagnosis n Pulmonary embolism n Aortic dissection n Pericardial effusion n Cardiac tamponade n Tension pneumothorax n Esophageal rupture
Physical Exam n Diaphoresis – Cool & pale skin due to vasoconstriction n Dyspnea / Evidence of CHF – Elevated JVD, LE swelling & decreased cardiac output n Anxiety or irritability n Abnormal &/or irregular pulse rate n Hypo / Hypertension n Nausea or vomiting n Auscultation abnormalitites: – S 3 & S 4, systolic murmurs, pericardiac friction rub
EKG n Detects electrical abnormalities n Limitations: – A “normal” EKG does not rule out acute MI – Represents a brief period of time – Difficult for evaluating posterior & lateral heart – Mistakes in interpretation are relatively common n STEMI requires >1 mm ST elevation in contiguous limb leads & >2 mm elevation in precordial leads n ECG mimics of acute MI include: LVH, LBBB, paced rhythms, early repolarization, pericarditis, hypo/erkalemia, ventricular aneurysm
How To Read ECGs (The 10 Minute Version)
What Does This Mean? I Av. R V 1 V 3 II Av. L V 2 V 4 III Av. F V 3 V 5 Lead II Continuous Strip
Coronary Arteries n Right Coronary (RCA) perfuses right ventricle / inferior wall n Left Main (LMA) divides into: – Left Anterior Descending (LAD) which perfuses the anterior left ventricle – Left Circumflex (LCX) which perfuses lateral left ventricle
Inferior = Right Coronary Artery II, III, Av. F n Right ventricle positioned down & inferior n Perfused by RCA n Innervated by same nerve as stomach: – Inferior wall MIs cause nausea & vomiting
Inferior Leads: RCA II Inferior III Av. F Inferior
Septal = RCA & LAD V 1, V 2 n Two vessels cover this large area of the heart n V 2 overlaps septal & anterior areas n A septal MI is best seen in V 1 & V 2
Septal Leads V 1 Septal V 2 Septal
Anterior = LAD (V 2), V 3, V 4 n Septum & anterior left ventricle perfused by LAD n V 1 & V 2 directly over cardiac septum n V 2 (septal overlap), V 3, V 4 look at anterior heart n “Precordial” leads
Anterior Leads V 4 Anterior V 3 Anterior
Lateral: LMA & LCX I, Av. L, V 5, V 6 n Winds around left chest & lateral left ventricle n LMA “Widow Maker”: – Divides into LAD & LCX – LMA occlusion causes a massive antero-lateral MI
Lateral Leads I Lateral Av. L V 5 Lateral V 6 Lateral
Contiguous Leads I, Av. L, V 5, V 6 II, III, Av. F V 1, V 2 (V 2, V 3) V 3, V 4 I Av. R V 1 V 4 Lateral Septal Anterior LMA, LCX RCA, LAD II Av. L V 2 V 5 Inferior Lateral Septal Lateral RCA LMA, LCX RCA, LAD LMA, LCX III Av. F V 3 V 6 Inferior Anterior Lateral RCA LAD LMA, LCX
Evolution of Infarction Q Wave ST Elevation ST Depression Resolution The more leads of the ECG with infarction changes, the larger the infarct size & the worse the prognosis
ST-segment elevation (orange) in I, a. VL, V 1 -V 5 with reciprocal changes (blue) in inferior leads, indicative of an anterior wall myocardial
Acute inferior STEMI, with elevations in leads II, III, & a. VF with reciprocal ST segment depression in leads I & a. VL
ECGs & Prehospital Treatment n Early access to EMS via 911 available in 90% of the US n EMS plays a key role in reducing door to balloon intervals by performing a field ECG & rapid triage n ECG transmitted to the receiving hospital, allowing time saving decisions to be made prior to patient's arrival – In the absence of a formal alert program, prehospital ECGs associated with reduced treatment intervals in the ED n Three things save patients: – Early Recognition (Speed) – Early Defibrillation (Electricity) – Adequate Compressions (Power)
Prehospital Management (Adopted from AOM) n BSI / PPE n Place patient in a position of comfort while performing a focused history & physical examination n Obtain & serially monitor vitals n Maintain airway & provide O 2 if <94% n Initiate early transport – Request ALS back-up if available
Prehospital Management ~ Medications n Administer 4 baby aspirins n Ask if patient has personal NTG; if no contraindications give 0. 4 under the tongue every 5 mins if in pain – Ask if patient has taken Viagra, Levitra, Cialis in past 24 - 72 hrs n Reassess q 3 - 5 minutes or if any chest discomfort, lightheadedness, dizzy, &/or hypotension n If patient is symptomatic after administration of NTG, place patient flat or Trandelenberg n If the patient experiences no relief & SBP remains > 100 mm Hg contact medical control for further direction n Continue serial assessments
Cardiac Arrest Management n Unresponsive, with apneic or agonal respirations & pulseless n BSI / PPE / ABCs n Start CPR – If CPR started prior to your arrival, stop & confirm apnea & pulselessness n Request ALS back-up or intercept n Continue CPR x 2 minutes then apply AED
Cardiac Arrest Protocol n If pulse present: – Assess ABCs – If respirations adequate, administer high flow O 2 via NRB – If respirations not adequate, assist with BVM at 8 -10 BPM & prepare to provide an advanced airway n If pulse absent: – Assist ventilations with BVM at 8 -10 BPM & prepare to provide an advanced airway – Stop CPR, ensure people are clear of patient & again press "Analyze" on the AED – Follow AED directions for "Deliver Shock" or "No Shock“ – Resume CPR immediately after shock without pulse check
Cardiac Arrest Protocol n If indicated by the AED, provide up to a total of 3 shocks (not stacked) n Contact medical control after the 3 rd shock or after three consecutive "No Shock" advisories are obtained n Advanced airway should be performed after the second shock or after the second "No Shock“
AEDs & MI n The PAD (Public Access Defibrillator) showed the availability of AEDs in public places may significantly increase chances of survival n AEDs now in public buildings & transportation facilities, casinos, & in non-ambulance emergency vehicles n AEDs analyze the heart's rhythm & determine whether the rhythm is amenable to defibrillation – Decreases time to first shock by minutes increasing survival
MI Arrhythmia Pathophysiology n Injured heart tissue conducts electrical impulses more slowly than normal tissue n The difference in conduction velocities triggers a feedback loop causing lethal arrhythmias n The most serious of these arrhythmias is ventricular fibrillation, the leading cause of sudden cardiac death n Ventricular tachycardia usually results in rapid heart rates that prevent the effective pumping of blood, droping cardiac output & BP, leading to further coronary ischemia & extension of the infarction
Arrhythmia Treatment ~ Defibrillation n Defibrillation designed to terminate potentially lethal arrhythmias n Delivers electrical shock to to depolarize the heart muscle, in effect "rebooting" the heart n Time dependent; successful defibrillation decline rapidly after the onset of cardiac arrest – <1 minute = 80% – >4 minutes = 50% – >8 minutes = 10%
Cardiac Arrest Important Points ~ Peds, Trauma, AEDs n Weight not age used for AED as cardiac injury can occur at 10 joules/kg – AEDs cannot provide low energy required for pediatric defibrillation n In traumatic arrest the AED may not be helpful as condition is result of blood loss requiring surgical intervention rather than electricity n When using the AED during transport, stop the vehicle to analyze the rhythm or deliver shocks n If patient is successfully defibrillated, has a pulse, & rearrests, continue rhythm analysis & follow directions of the AED for "Deliver Shock" or "No Shock" advisories
MI Hospital Management Strategies
Thrombolysis n Treatment of STEMI within 12 hours of the onset of symptoms & primary PCI is immediately available – Effectiveness highest in the first 2 hours – Failure rates >20% n Thrombolytics contraindicated in treatment of unstable angina, NSTEMI, & treatment of individuals with evidence of cardiogenic shock n Intracranial hemorrhage & stroke are serious side effects – Previous ICH, age, & thrombolytic regimen being used – Complications are significantly higher with rescue PCI than with primary PCI due to the action of the thrombolytic agent
Coronary Artery Bypass Surgery (CABG) n Emergency bypass surgery for MI less common then PCI or medical management n CABG with intra-aortic balloon pumps simultaneously treats a mechanical complication (i. e. valvular defect) & cardiogenic shock – Uses an artery or vein from the patient being implanted to bypass coronary artery occlusions n There is a higher mortality rate than in PCI of performed immediately following infarction n In patients with >2 arteries affected, CABG associated with higher long-term survival compared to PCI
Primary Percutaneous Coronary Intervention (PCI) n Primary PCI restores flow in 95% of patients with STEMI n Goal is to open artery <90 mins after symptom onset – “Symptoms-to-balloon” n Angiogram determines anatomical location of blocked, followed by balloon angioplasty +/- stenting – Stents decrease rates of vessel restenosis compared to balloon angioplasty
Key Prehospital Points n Early recognition n Aspirin / O 2 / AED saves lives n Goal is in the catherization lab < 90 mins post onset of symptoms
Stroke n Loss of brain function from a cerebralvascular abnormality – WHO: "neurological deficit of cerebrovascular cause persisting >24 hrs or causing death within 24 hrs“ n Causes from a lack of blood flow (ischemic), or an interrupted blood flow (hemorrhagic) n Hippocrates (460 BC) termed stroke “Apoplexy”, which is Greek for "struck down with violence”
CVA vs TIA vs RIND n Transient Ischemic Attack n Reversible Ischemic Neurological Deficit n 30% of those with TIA will have a major CVA wihin 90 days – Stroke related syndrome that resolves in <24 hrs – Stroke related syndrome that resolves in <72 hours – 30% of these patients will not survive
Epidemiology n Disability affects 75% of survivors – #1 cause of adult disability in the US & Europe – #3 cause of death worldwide after CAD & cancer – Causes 10% of deaths worldwide n Management costs $43 billion annually in the US n Incidence increases exponentially >30 yrs – Etiology varies by age – 95% of strokes occur in people >45 yo – 75% of strokes occur in people >65 yo
Gender Differences n Men 1. 25 x more likely to suffer strokes than women n However, 60% of deaths from stroke occur in women n Since women live longer than men, they are older on average when they have their strokes & therefore more often killed n Some risk factors for stroke apply only to women: – Pregnancy – Childbirth – Menopause – HRT
Stroke Risk Factors n Advanced age n Previous stroke or TIA n Diabetes n High cholesterol n Cigarette smoking n Atrial fibrillation n HRT n Migraines n Thrombophilia n Patent foramen ovale n HTN – Mst important & modifiable
CVA History n AMS n Altered speech, sensory, or motor function without suspected trauma – Trauma can cause an intracerebral bleed, but is treated differently than a CVA n Possible history of prior stroke or TIA
Stroke Symptoms n Fairly rapid development n Symptoms related to anatomical location of damage n Ischemic: – Affect regional areas of brain perfused by blocked artery n Hemorrhagic: – Affect local or global symptoms due to bleeding & increased ICP n By history & neurological examination, as well as the presence of risk factors, the anatomical nature of the stroke can often be identified
Stroke Mimics n Seizure n Infection – Meningitis – Sepsis – Endocarditis n Hypoglycemia n Syncope n Brain abscess or tumor n Drug overdose n Head trauma n Migraine n Vascular lesions n Hypertensive encephalopathy – Arteriovenous malformation
Stroke Categories n Ischemic: n Hemorrhagic: – Interruption of the blood supply – 80% of strokes – Rupture of a blood vessel or an abnormal vascular structure – 20% of strokes
Ischemic Stroke n Blood supply to part of the brain is decreased, leading to brain tissue dysfunction & necrosis n 4 Causes: – Thrombotic: n Obstruction of vessel by a local clot – Embolic: n Clot from elsewhere in the body – Systemic hypoperfusion: n Low BP due to shock – Cryptogenic: n Unknown origin
Thrombotic Stroke n Thrombus (blood clot) forms around atherosclerotic plaques n Since blockage of the artery is gradual, onset of symptomatic thrombotic strokes is slower than an embolic CVA n A thrombus can lead to an embolic stroke
Embolic Stroke n Blockage of an artery by a traveling particle or debris in the arterial bloodstream originating from elsewhere n Generally a blood clot, fat (bone marrow in a broken bone), air, cancer cells or clumps of bacteria (endocarditis) n Sudden onset, symptoms usually are maximal at start n Emboli commonly arise from the heart (A fib) but may originate from elsewhere in the arterial tree n In paradoxical embolism, a DVT embolises through an ASD or VSD in the heartdirectly into the brain – Symptoms may be transient as the embolus is partially resorbed and moves to a different location or dissipates altogether
Systemic Hypoperfusion n Reduction of blood flow to all parts of the body n Causes: – – – n Pump failure: cardiac arrest, arrhythmias Reduced cardiac output: MI, PE, hemorrhage, shock Hypoxemia Entire brain affected, especially penumbra / "watershed"
Hemorrhagic Stroke n Accumulation of blood anywhere within the skull n Mrtality rate of 44% at 30 days n Types: n Causes: – HTN – Trauma – Intraparenchymal – Bleeding disorders – Intraventricular hemorrhage – Amyloid angiopathy – EDH – SAH – Illicit drug use – Vascular malformations
Symptoms n Generally Unilateral – Stroke site on opposite side than clinical ssx – LOC, HA, & vomiting common in hemorrhagic than ischemic (increased ICP from leaking blood vessels compresses brain) n Cerebral Cortex: – – Occipital: Temporal: Parietal: Frontal: Visual field defect Memory deficits Hemineglect , aphasia Disorganized thinking, confusion, hypersexuality
Symptoms n Brainstem / Cranial Nerves: – Altered smell, taste, hearing, or vision – Ptosis, diplopia, pupil reactivity – Decreased gag, tongue movement, facial sensation & muscle weakness – Balance problems & nystagmus – Altered breathing & pulse n Cerebellum – Altered coordination – Vertigo or disequilibrium
Time is Brain n From the time a patient first experiences ssx there is a 3 hour window to administer t. PA n That window includes: Recognition of symptoms Call to 911 & activation of EMS response, assessment, management & transport – ED assessment & CT scan to rule out hemorrhagic stroke – Stroke team activation & screening for TPA – – –
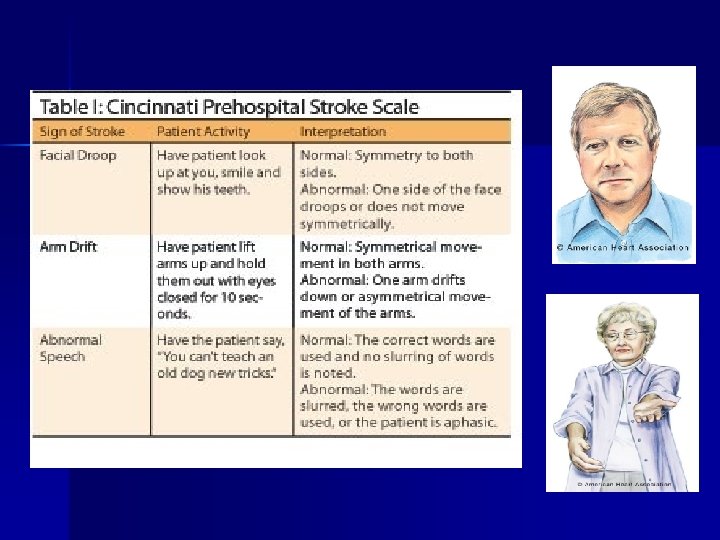
MEND Examination Miami Emergency Neurological Deficit Exam n Based on the NIH Stroke Scale, incorporates the Cincinnati Prehospital Stroke Scale (CPSS), takes < 3 mins to perform n ABCD n En route, perform full MEND Exam – D = CPSS
Management n BSI / PPE n Rapid administration of stroke scale + glucose testing n Maintain airway & administer O 2 – Prepare to assist ventilations & provide advanced airway – Request ALS if unresponsive or airway compromise n Place patient in supine position with head elevated n Begin early transport n Notify receiving ED of ETA & time of symptom onset n Perform serial assessments
Prehospital Treatment n Transport to a hospital with a stroke management team n Aggressive airway management n Treatment should be aimed at maintaining O 2 saturation > 95% & CO 2 between 28 – 35 mm. Hg – Patients with a GCS <8 , loss of gag, or failure to maintain adequate oxygenation or ventilation – If O 2 sat falls below 95%, there is a 150% increase in mortality n Prophylactic hyperventilation of the head-injured patient is no longer recommended n Elevate the head of the bed 30 - 35 degrees to reduce ICP n Thrombolysis ("clot-busters") both in the field & in the ED
t. PA Thrombolysis n “Clot busting“ unblocks the artery with t. PA +/- mechanical “rotor rooter” n Useful <3 hours of onset of symptoms if no abnormal lab values, HTN, recent surgery or GI bleed n When given in <3 hrs post ssx, 40% had good outcomes vs 26% of placebo – >6% developed fatal ICH n It is the position of the AAEM that evidence regarding efficacy, safety & applicability of t. PA for ischemic stroke is insufficient to warrant classification as “standard of care”
Hypertension Management n Prehospital management of hypertension is now considered dangerous for “cerebral resuscitation” n There is no evidence that emergent HTN improves neurological outcome – Numerous studies report neurological deterioration in strokes immediately following BP reduction n In the first 48 hrs post stroke, if the SBP drops <100 or O 2 sat falls <95%, there is a 150% increase in mortality n Rapid & dramatically lowered BP reduces blood flow to ischemic tissue & vulnerable but viable penumbra
Prevention n Primary prevention less effective than secondary n Determine patient's risk for other cardiovascular diseases n The most important modifiable risk factor are HTN n Medication is the most common method of prevention n Carotid endarterectomy is a surgical prevention method – Comprehensive medical management includes diet, exercise, & cessation of smoking & alcohol use – – – Statins Aspirin Antihypertensives
Key Prehospital Points n Early symptom recognition n Early hospital notification n Maintain hemodynamic stability
Summary n Cardiovascular diseases are among the top killers worldwide n Early recognition, treatment & transport are keys to good outcome
Questions? Amy. Gutman@uc. edu