Prehospital Documentation Amy Gutman MD prehospitalmdgmail com amy

 serve as: n Patient care record")










































- Slides: 45
Prehospital Documentation Amy Gutman MD prehospitalmd@gmail. com / amy. gutman@hahv. org
Why Is It Important? Patient Care Reports (PCRs) serve as: n Patient care record (continuity of care) n Legal document n Billing resource n Administrative tool
The PCR as a Record of Patient Care n n n Continuity of care Describes condition before & after EMS contact Establishes provider credibility & competency
The PCR “Serves as the ‘official record’ of the care you provided… The purpose of the PCR is to provide the reader with a ‘picture’ of the continuum of care that was provided to the patient from the arrival of first responders to the transfer of care in the hospital. It becomes your ‘substituted’ memory. ” Courtesy : Good Documentation is Your Best Defense: Steve Worth, Esquire
Legal Document n n n A report must be generated for any patient contact No exception for non-transports, patients “missing” on arrival, or situations in which there was minimal contact &/or no treatment provided Local standards on documentation may be viewed under NY EMS website
Billing Tool n Poorly written, incomplete or missing PCRs are billing obstacles
Administrative Tool n n Establishes need for EMS services in a particular area Protects your job
Narratives
DCHARTE D= C= H= A= R= T= E= Dispatch CC History Assessment Rx at scene Treatment Enroute Exemptions
Dispatch n What is the nature of the call? n Updates provided enroute n i. e. CPR in progress, police on scene
Chief Complaint n Why did patient call 911? n n Or who called & why? Described in patient’s own words, quotations if possible EMS should indicate reason patient was unable to speak Document who provided history
Examples n Upon arrival found 54 year old female seated on couch. Patient reports “pressure in chest” describes as “feels like someone is sitting on my chest” n Vs n “Possible heart attack”
What If Patient Curses? n Quote em! n “My chest f_c_ing hurts. ”
SAMPLE History n n n S A M P L E SSX Allergies Meds PMH Last PO intake Events (i. e. MOI)
SAMPLE – OPQRST n n n O P Q R S T Onset Provokes Quality Radiation Severity (scale of 1 -10) Time
Vital Signs n n n Blood Pressure Respirations n Effort n Number n Skin Temperature n Oxygen saturation n CO 2 n If possible Heart rate / regularity n Monitor strip
Treatment n All interventions n Includes: n n Interventions by bystanders prior to your arrival Your interventions Response to treatment Document telemetry or notification calls as part of treatment
Examples of “Treatments/ Interventions”
Other Treatments/ Interventions
Transportation n Method by which patient transferred n n ALS, BLS Method of transport to hospital n n n Seated Supine C spine immobilization Emergent (lights & sirens) Non-Emergent
Transportation n n Description of treatment initiated / continued n “VS reassessed q 15 mins. O 2 10 LPM via NRB due to decreased pulse ox from 99% RA to 90% RA” Also: n n Changes in condition upon ED arrival Document name / title of person care transferred to at ED
“Exceptions” n Anything that is an “exception” from the norm n i. e. “Patient refused aspirin due to known allergy” n All treatment must be consistent with protocols n Through CQI process, PCRs reviewed n Document everything that was done, & if a standard treatment was not done, why not?
Exceptions: Trauma Patients n n Principles of trauma triage suggest EMS providers document if patient meets criteria for transportation to a trauma center i. e. “Patient unconscious following MVC. Transported to a Level 1 trauma center due to bilateral femur fractures”
Alternative Methods: “SOAP” n n S O A P Subjective Observations Assessment Plan
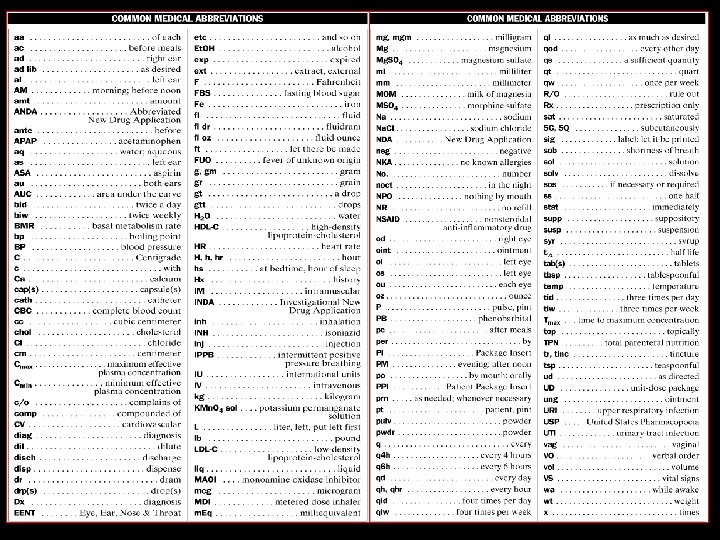
Abbreviations n No home-grown abbreviations n n n DRT, BFN Only accepted abbreviations Spelling counts n If a jury looks at your errorfilled chart they may conclude that you are as sloppy at patient care as you are at documentation
Pertinent Negatives n Anything you would expect to find during assessment, yet patient denies n n i. e. “no diaphoresis” while patient having CP NV status before / after splinting & spinal immobilization
Utstein OOHCA Documentation n Date/ Time n n Incident Number n n Accepting Hospital n Age/ DOB n n Gender n n Past Medical History n Down Time n ROSC n Time to Patient Contact n HPI Narrative n Witnessed Arrest n Bystander CPR Initial & Serial Rhythms Initial & Serial Vitals (ventilation rates!) Initial & Serial ETCO 2 Any Interventions (meds, defibrillation)
Basics A Good Narrative tells a “story”, giving a full picture of the code
Down Time n Best estimate based upon “story” received on scene n Quantify as: n n n <10 mins 11 -15 mins 16 -30 mins 31 -60 mins > 60/ unk mins
Time to Patient Contact • NOT time “on scene” • If another unit arrives first, document their interventions
Witnessed Arrest & Bystander CPR n n “Yes” or “No” Bystander CPR can be noted in HPI as well, including if AED used on scene n Tracks community involvement & outcomes n Helps in receiving public health grants for education
Vitals are VITAL! n If patient is coding with “no” vitals, document rate at which you are ventilating patient n n n New CPR Guidelines Ongoing research ETCO 2 not just a number, it is a predictor of outcome
• Et. CO 2 is a cardiac output indicator • The lower the CO, the lower the Et. CO 2 • If Et. CO 2 <10 mm. Hg after 20 minutes of CPR, resuscitation success rate is <1% • Higher Et. CO 2 = effective resuscitation
Rhythm n Initial n Changes with any intervention n Final rhythm at presentation to ED
ROSC n n Perfusing BP, sustained HR, spontaneous respirations prior to transferring patient to the ED After that, it’s the QA officer’s / medical director job to determine if the “ 20 minute” Utstein criteria time frame present, & patient outcome
Important Points to Document n n n NV status before & after splinting & spinal immobilization Loose/ missing teeth prior to intubation Reason for Triage: n n n Closest facility Patient request Trauma Triage n Transfer of Care n n n Facility Name of person Title of person Condition at time of transfer Times: n n n Dispatched to scene Arrival on scene Time on scene Departure to hospital Arrival to hospital
Bystanders n Include name, level of training & license number of ANY non-EMS personnel who assist during assessment or management
Just The Facts, Please n n n Avoid name calling, i. e. “frequent flyer” If an error was made, document what happened & what you did to correct it Report delays in care, & how it affected treatment: n “Police did not secure the scene for 15 minutes, resulting in a delay of care”
Refusals n NEVER accepted by any pediatric patient or adult with AMS / not competent to make decisions n Document attempts to convince patient transport is recommended n n n Include potential consequences explained to patient Potential consequences always includes DEATH All refusals must be signed, including signatures by the patient/ guardian / health care agent, provider & witness n If police or an adult family member not available, your partner’s signature is appropriate
DNR / MOLST n n n DNR/ MOLST? Competent patient / health care agent can change mind at any time Include statement regarding DNR / MOLST in your report n n ? Date ? Signed Physically present at scene DNR does not equal “Do Not Treat”
This Is Not CSI n Unless you’re a medical or forensic specialist don’t make assumptions n n i. e. entrance & exit wounds Explain what was found & how it appeared n “Infant found face-down under bed-sheets, cold, cyanotic, with vomitus noted in oropharynx”
Helpful Hints n Protect patient confidentiality n Follow HIPAA guidelines n Falsification of EMS report equals fraud n Any PCR CAN be subpoenaed without you being there to defend it
Of Course… n n n If it was not documented, it never happened If it was documented…it doesn’t mean it happened Always proofread
Questions? prehospitalmd@gmail. com / amy. gutman@hahv. org