APPROACH TO CONGENITAL HEART DISEASE Does the child




































 Outlet septum")












: Intervene earlier, infant")







- Slides: 61
APPROACH TO CONGENITAL HEART DISEASE
Does the child have congenital heart disease? ?
Nada’s Criteria Major Systolic murmur gr III or more in intensity Diastolic murmur Cyanosis Congestive heart failure
Minor Systolic murmur less than gr III in intensity Abnormal second heart sound Abnormal electrocardiogram Abnormal thoracic roentgenogram Abnormal blood pressure
SVC IVC RA LA LV RV Aorta PA Lungs PVs
CHD Fetal circulation Placental blood – Umbilical veins – Ductus venosus – IVC – RA – PFO – LA – LV – Aorta SVC blood – TV – RV – PA – PDA – Aorta Systemic venous blood flows into umbilical arteries into the placenta
Systolic murmurs Organic> gr III or associated with Thrill Pansystolic murmur-MR, TR and restrictive VSD ESM associated with thrill or click. ESM<gr III Hyperdynamic states, anaemia Still’s murmur
Diastolic murmur- always pathological Early- aortic or pulmonary Delayed- mitral or tricupid
Cyanosis R-L shunt Pulmonary disease Low cardiac output Methemoglobinemia Clinically apparent --- saturation <85% Central vs Peripheral
Congestive Heart failure Indicative of structural heart disease Neonates and infants Hypoxia Hypoglycaemia Hypocalcemia Severe anaemia- cause or precipitating factor
Minor Systolic murmur < gr III Does not rule out heart disease- severe heart disease can present without murmur-TGA, TAPVC PSM due MR/TR can be because of myocardial disease.
Abnormal second heart sound Two components A 2 and P 2 Split- normal A 2>P 2 Normal S 2 - All 3 components. Finding a normal S 2 in a significant structural heart disease is practically zero.
Abnormal Electrocardiogram
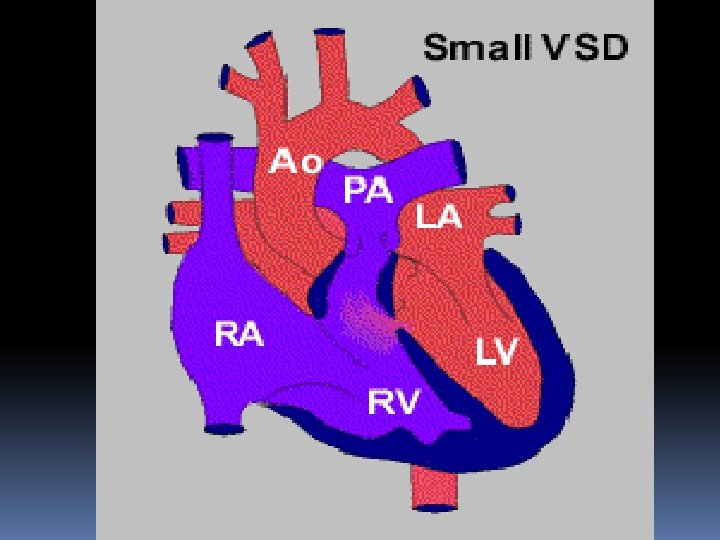
Small VSD in a young child
Moderate sized VSD
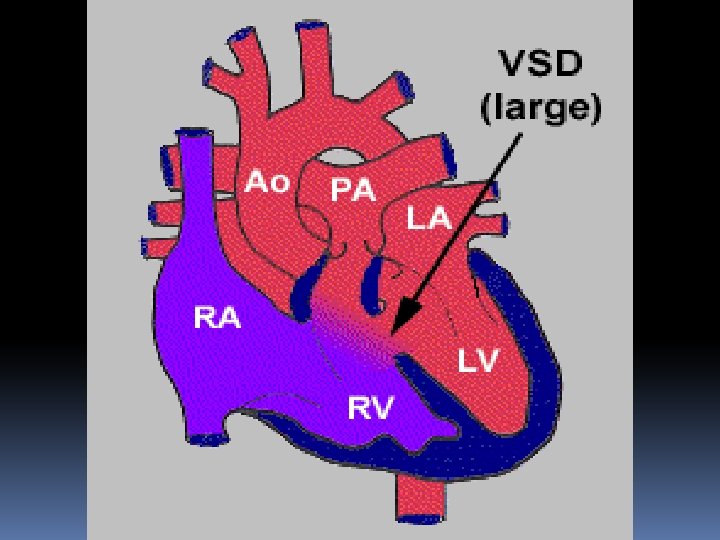
Large VSD with biventricular forces
VSD Eisenmenger
Post op Inlet VSD closure, Wenckebach
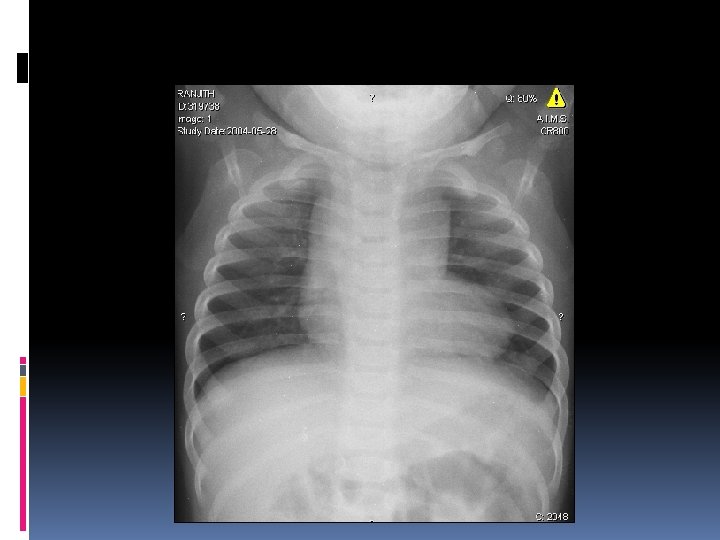
Abnormal chest roentgenogram
1. Trachea 2. Right Mainstem 3. Left Mainstem 4. Left Pulmonary Artery 5. Right upper lobe pulmonary vein 6. Right Interlobar artery 7. Not labeled 8. Aortic knob 9. Superior vena cava 10. Ascending aorta 11. Carina 12. Right atrium 13. Right ventricle 14. Left ventricle 15. Left Hemidiaphragm 16. Right Hemidiaphragm 17. Costophrenic angle
Supracardiac TAPVC Left vertical vein Dilated SVC 8 years old; minimally symptomatic
Transposition of Great Arteries
Ebstein’s anomaly
Scimitar Syndrome What do the arrows indicate?
Situs inversus, Dextrocardia, left arch
Situs Ambiguous, levocardia Mid line Stomach Liver
Device closure of ASD
Device closure of VSD
The Normal Heart
CHD: Traditional Approach Acyanotic Cyanotic pulmonary blood flow PS PAH L-R Shunts Miscellaneous Obstructive lesions
CHD - Classification Acyanotic CHD – where the shunting of blood is from left side to right side (pressure on the left is higher than right) �Pink �Breathlessness, esp on exertion �Recurrent respiratory tract infections �Failure to thrive Acyanotic CHD without shunt – malformations in the heart
CHD Classification Cyanotic CHD – Where shunting is from right side to left side (pressure in the right side is higher than on the left side) �Blue child – cyanosis �Clubbing �Cyanotic Spells �May occasionally be “pink”
Acyanotic CHD Without shunts Malformations of the heart on right side; on left side With shunts Level of shunt �Atrial - ASD �Ventricular - VSD �Great arteries – PDA, AP window �Multiple levels – AV canal defects �Misc – ALCAPA, RSOV, Coronary AV fistula
Cyanotic CHD With increased pulm blood flow TGA TAPVC Tricuspid atresia with non-restrictive VSD Common atrium Truncus arteriosus TOF with PA and MAPCAs
Ventricular Septal Defects 25 -30% of the cardiac defects Natural history depends on size and location of the defect Perimembranous or ‘subaortic’ (80%) Subpulmonic or outlet VSD Inlet VSD Trabecular or muscular VSD
Ventricular Septal Defect • quiet murmur = large defect • loud murmur = small defect
Ventricular Septum: Landmarks in the RV surface Pulmonary Valve Membranous Conal (outlet) Outlet septum Anterior tricuspid leaflet Septal band Trabecular Inlet Septal leaflet Moderator band
Ventricular Septal Defects: Spontaneous Closure 60% close by 3 years and 90% by 8 years’ 25 -30% overall 75 -80% of small VSDs Rare with large defects Muscular and perimembranous types Inlet VSDs and malalignment VSDs do not close or reduce in size
Large VSDs Heart Failure Pneumonia, can be life threatening Does not respond like usual community acquired pneumonias Failure to thrive Pulmonary vascular changes, can become inoperable fast
Timing Guidelines: Large Perimembranous VSD No symptoms: Anytime after 3 months Symptoms: Earlier Associated conditions & Trisomy 21 Age at operation beyond 1 -2 months does not impact surgical outcome
Timing Guidelines: Large Muscular VSD Higher likelihood of spontaneous closure Close watch for signs of spontaneous closure Medical management of CHF may be tried until the age of 6 months At times PA banding
Moderate to Small VSDs Aortic cusp prolapse causing AR 5 -8% with Perimembranous VSD 30% with Subpulmonic VSD Infective Endocarditis Incidence 2. 5/1000 patient years More with LV-RA shunts (STL aneurysm) Subaortic membrane in up to 6%
Moderate VSD If symptomatic, operate If asymptomatic, decision based on the shunt Clinical assessment Echo: Significant LA and LV enlargement and degree of restriction
Small VSD Medical follow up Infective Endocarditis Prophylaxis Echo at regular intervals Operate if AR develops
Ventricular Septal Defects 25 -30% of the cardiac defects Natural history depends on size and location of the defect Perimembranous or ‘subaortic’ (80%) Subpulmonic or outlet VSD Inlet VSD Trabecular or muscular VSD
Atrial Septal Defect Incidence: Accounts for 14% of all CHD with female predominance (4: 1) Types: Sinus venosus Fossa ovalis or ostium secundum Ostimum primum
Atrial Septal Defects Fossa Ovalis ASD Primum ASD
ASD Wide fixed second sound P 2 is generally loud even without PAH Short Ejection murmur at pulmonary area = Small defect (<2: 1 shunt) 3/6 ESM + RV S 3 or Tricuspid MDM = Large defect (>2: 1 shunt)
Atrial septal defect
Timing Guidelines: Large ASD No symptoms: Preschool age If symptomatic (510%): Intervene earlier, infant repair not associated with increased risk
Early closure of ASD Advisable if the child is symptomatic July 1998 – March 2004, 43 children aged <2 years 2. 3% of ASD repairs Indications: FTT or RTI ( 2 admissions) Follow up: No LRTI or admission Significant weight gain
Non-surgical management of ASD • Transcatheter closure • Amplatzer septal occluders • HELEX septal occluder Suitable for older children and adults with adequate margins around ASD
Patent Ductus Arteriosus Pathophysiology vascular communication that persists after birth between the pulmonary artery and the aorta Incidence accounts for 12% of CHD with female predominance
Patent Ductus Arteriosus Newborn – Preterm Vs Term Baby Role of Indomethacin or ibuprofen/ surgery Unlikely to close or reduce in size after a month in term babies Preterms may take longer
Patent Ductus Arteriosus Large Duct – Usually symptomatic Surgical intervention or transcatheter closure Asymptomatic PDA Risk of Infective endocarditis Large ducts develop Eisenmenger syndrome Silent PDA can be left alone
Transcatheter interventions in PDA
Patent Ductus Arteriosus Surgical Management VATS Ligation Division and suturing Transpulmonary closure