Congenital hypothyroidism Embryology of thyroid gland Thyroid hormone

Congenital hypothyroidism

Embryology of thyroid gland

Thyroid hormone metabolism

Etiologic classification of CH o Primary hypothyroidism o Central hypothyroidism pituitary hypothalamic
 o Thyroid dysgenesis 1) aplasia 2) hypoplasia 3) ectopia o Thyroid dyshormonogenesis")
Primary hypothyroidism(1) o Thyroid dysgenesis 1) aplasia 2) hypoplasia 3) ectopia o Thyroid dyshormonogenesis 1) Iodide transport defect 2) Thyroid organification or coupling def. 3) H 2 O 2 generation defect 4) Thyroglobulin synthesis defect 5) Deiodination defect
 o o TSH unresponsiveness Thyroid hormone transport defect Iodine deficiency (endemic goiter)")
Primary hypothyroidism(2) o o TSH unresponsiveness Thyroid hormone transport defect Iodine deficiency (endemic goiter) Maternal antibody Thyrotropin receptor-blocking Ab (TRBAb) o Maternal medications iodine, amiodarone, radioiodine, propyothiouracil, methimazole

Central hypothyroidism o o o Pit-1 mutations Prop-1 mutations TSH deficiency Multiple pituitary deficiencies TRH deficiency TRH unresponsiveness

Incidence of CH

Causes of thyroid dysgenesis o familial, 2% Mutations in transcription factors (TTF-1/NKX 2. 1, TTF-2, PAX-8) o Sporadic, unknown: 98%

Clinical manifestations o prolonged physiologic jaundice, feeding difficulty o large tongue, depressed broad nose, respiratory difficulty o constipation, hypotonic, umbilical hernia o cold, mottled skin & coarse, brittle hair o edema of the genitals & extremities, myxedema o slow pulse, asymptomatic pericardial effusion o cardiomegaly, macrocytic anemia, carotenemia o delayed dentition, large fontanel o retardation of physical & mental development
")
Congenital hypothyroidism (infant)
")
CH (dyshormonogenesis)
")
Congenital hypothyroidism (child)
 o Neonatal screening test 1) T 4 ↓ primary hypothyroidism pituitary")
Laboratory findings (1) o Neonatal screening test 1) T 4 ↓ primary hypothyroidism pituitary hypothyroidism hypothalamic hypothyroidism 2) TSH ↑ primary hypothyroidism subclinical hypothyroidism o Thyroid function test free T 4: ↓ T 3: → or ↓ TSH: ↑
 o Thyroid scan & thyroid US (123 I-sodium iodide, 99 m.")
Laboratory findings (2) o Thyroid scan & thyroid US (123 I-sodium iodide, 99 m. Tc-sodium pertechnetate) 1) Aplasia 2) Thyrotropin receptor-blocking Ab. (TRBAb) 3) Iodide-trapping defect 4) Ectopic thyroid o Bone age: retarded o EKG low P, T, QRS

Sublingual thyroid

Diagnostic algorithm
")
Treatment of CH (1)

Prognosis o Delay in Dx. Inadequate Tx. Poor compliance in the 1 st 2 -3 yr. retarded skeletal maturation reduced IQ, incoordination, hypotonia or hypertonia short attention span, speech problems with vocabulary, reading, arithmetic, memory neurosensory hearing deficit

Calcium homeostasis & Bone metabolism

Actions of PTH & vitamin D Hormone Bone Kidney Intestine serum Ca serum P PTH resorption↑ Ca reabsorption↑ P reabsorption↓ Ca absorption↑ ↑ ↓ Vit D resorption↑ Ca reabsorption↑ P reabsorption↑ Ca absorption↑ ↑ ↑

Metabolism of vitamin D
 2) 3) o Early neonatal hypocalcemia (12 -72 hr) Premature")
Neonatal hypocalcemia o 1) 2) 3) o Early neonatal hypocalcemia (12 -72 hr) Premature infant Asphysia Infants of diabetic mother Late neonatal hypocalcemia (2 -7 d. ) high phosphate milk feeding
 Total serum Ca ≤ 7 mg/d. L (1. 75")
Definition of neonatal hypocalcemia 1) Total serum Ca ≤ 7 mg/d. L (1. 75 m. M) 2) Ionized Ca <4 mg/d. L (1 m. M)
 1. Parathyroid hormone def. 1) Aplasia or hypoplasia of")
Etiologic classification of hypocalcemia (1) 1. Parathyroid hormone def. 1) Aplasia or hypoplasia of parathyroids 2) Suppression of neonatal PTH secretion d/t maternal hyperparathyroidism 3) Preproparathyroid hormone gene mut. 4) Ca 2+ sensing receptor activating mut. 5) Autoimmune parathyroiditis 6) Infiltrative lesions
 2. PTH receptor defects (pseudohypoparathyroidism) 3. Mitochondrial DNA mutations")
Etiologic classification of hypocalcemia (2) 2. PTH receptor defects (pseudohypoparathyroidism) 3. Mitochondrial DNA mutations 4. Magnesium def. 5. Exogenous inorganic phosphate excess 6. Vitamin D def.

Di. George syndrome

C/M of hypoparathyroidism o o o o Muscular pain & cramp Numbness, stiffness, tingling (hand, foot) Chvostek sign, Trousseau sign Laryngeal spasm, carpopedal spasm Convulsion Late eruption of teeth, irregular enamel Dry & scaly skin, horizontal line on nail
 P")
Lab. of hypoparathyroidism o o o o Ca ↓ (5 -7 mg/d. L) P ↑ (7 -12 mg/d. L) ALP → or ↓ PTH stimulation: u c-AMP, phosphate↑ Bone X-ray: metaphysis density↑ Brain CT: calcification in basal ganglia

Tx of hypoparathyroidism o 5 -10 m. L of 10% calcium gluconate o 1, 25 -dihydroxycholecalciferol (calcitriol) initial: 0. 25 ㎍/kg/24 hr maintenance: 0. 01 -0. 1 ㎍/kg/24 hr o Vit D 2 infant & young child: 0. 1 -0. 5 mg/24 hr older child: 1. 25 -2. 5 mg/24 hr o Elemental Ca: 800 mg/24 hr

Rickets 1. 2. 3. 4. Vitamin D-deficiency rickets Vitamin D-dependent rickets type II Familial hypophosphatemia (Vitamin D-resistant rickets)
 o Etiology Sun exposure dec. Vit D intake dec. Liver")
Vitamin D-deficiency rickets (1) o Etiology Sun exposure dec. Vit D intake dec. Liver dis. Kidney dis. Malabsoption, Anticonvulsant o Sx. Craniotabes, large fontanel, caput quadratum Rachitic rosary, pigeon chest, Harrison groove, Funnel chest, kyphosis, lordosis, scoliosis Bowleg, knock knee, coxa vara, rachitic dwarfism

Rachitic rosary

Active & healing rickets

Harrison groove
 o Treatment 1) Vit D 3 50 -150 ㎍/d. 2)")
Vitamin D-deficiency rickets (2) o Treatment 1) Vit D 3 50 -150 ㎍/d. 2) 1, 25(OH)2 D 3 0. 5 -2 ㎍/d.
D 3 -1α-hydoxylase 의 이상 적은 용량의 1,")
Vitamin D-dependent rickets o Type I 25(OH)D 3 -1α-hydoxylase 의 이상 적은 용량의 1, 25(OH)2 D 3로도 호전 o Type II Hereditary resistance to 1, 25(OH)2 D 3
 o Pathogenesis 1) Defect in proximal tubular reabsorption of phosphate 2)")
Familial hypophosphatemia (1) o Pathogenesis 1) Defect in proximal tubular reabsorption of phosphate 2) Defect in conversion of 25(OH)D 3 to 1, 25(OH)2 D 3 o Sx Short stature, frontal bossing, square head, waddling gait, smooth bowing of lower extremity, intraglobular dentin

Familial hypophosphatemia
 o Radiographic findings Metaphyseal widening, fraying, cupping Coarse-appearing trabecular bone o")
Familial hypophosphatemia (2) o Radiographic findings Metaphyseal widening, fraying, cupping Coarse-appearing trabecular bone o Tx. 1) Oral phosphate (Joulie solution) q 4 hr. 0. 5 -1 g/d. (young), 1 -4 g/d. (older child) 2) Dihydrotachysterol (vit D analogue) 0. 02 mg/kg/d 3) 1, 25(OH)2 D 50 -65 ng/kg/d.

DDx of rickets

Congenital adrenal hyperplasia

Anatomy of adrenal gland adrenal gl.

Histology of adrenal gland aldosterone cortisol androgen catecholamine

Steroid biosynthesis
 classic form: 1: 15000 -20000")
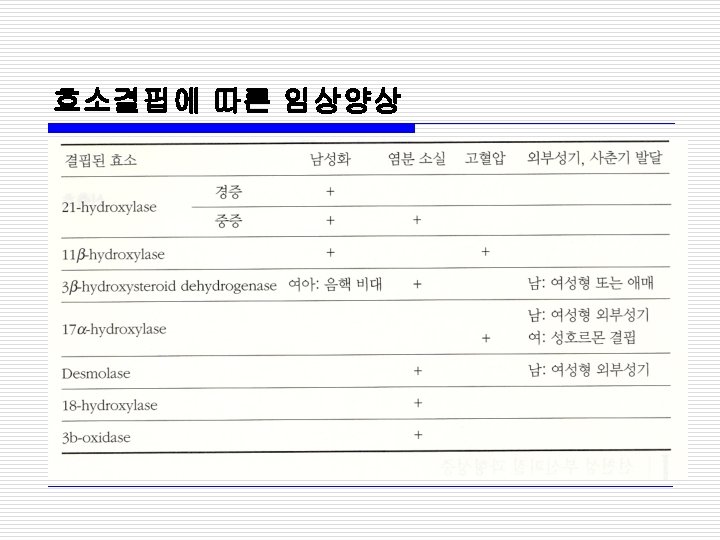
Classfication of CAH o 21 -hydroxylase def: 90% 1) classic form: 1: 15000 -20000 a) salt-losing, virilizing form(75%) b) simple virilizing form(25%) 2) nonclassic form: 1: 1000 o 11ß-hydroxylase def: 5 -8% 1) classic, severe form 2) nonclassic, milder form

Genetics of CAH
 progressive wt")
C/M of classic CAH o Salt losing form (aldosterone, cortisol def. ) progressive wt loss, anorexia, dehydration, vomiting, weakness, hypotension, hypoglycemia, hyponatremia, hyperkalemia o Virilizing form (pre-, post-natal androgen↑) 1) male: premature isosexual development 2) female: female pseudohermaphroditism

C/M of nonclassic CAH o Late-onset form Female: premature pubarche, menstrual irregularity, severe acne, hirsuitism, infertility, premature epiphyseal fusion Male: premature pubarche, increased phallus but small testis, severe acne, premature epiphyseal fusion o Cryptic form: No specific Sx
")
Addison disease(1)
")
Addison disease(2)
")
External genitalia (GP 7 wk. )
")
C/M of CAH (1)
")
C/M of CAH (2)
")
C/M of CAH (3)

Lab. of CAH o 1. 2. 3. 4. 5. 21 -hydroxylase def. Hyponatremia, hyperkalemia, hypoglycemia ↓: Cortisol ↑: ACTH, PRA, 17 -OHP, androstenedione ↑: 24 h urine 17 -ketosteroid 17 -OHP/cortisol after ACTH stim. > 0. 1: CAH with 21 -hydroxylase def. 0. 023 -0. 08: heterozygote (carrier)

w/u for ambiguous genitalia 1. 2. 3. 4. P/Exam. US: uterus, gonad Karyotype Hormonal test

Prenatal Dx. of CAH o amniocentesis: 임신 15 -18주 양수의 17 -OHP 측정 o Chorionic villus biopsy: 임신 8 -11주 융모 조직 배양 세포의 DNA 분석 (HLA typing, CYP 21 gene analysis)
 : 임신")
Prenatal Tx. of CAH o Dexamethasone 20㎍/kg/day (0. 5 mg x 2/day) : 임신 6주부터 Chorionic villus biopsy male female stop Tx continue Tx

Newborn screening of CAH o 17 -OHP level↑: 2주 후 recheck, electrolyte GP 26 -28 W. : 124 -841 ng/d. L GP 31 -35 W. : 26 -568 ng/d. L Full-term: 7 -77 ng/d. L 1 -12 M male: 40 -200 ng/d. L female: 13 -106 ng/d. L Prepubertal children: 3 -90 ng/d. L

Tx of CAH o Hydrocortisone 10 -20 mg/m 2/24 hr (stress시 2 -3배, op. 시 5 -10배 용량) o fludrocortisone 0. 1 -0. 3 mg daily (older infant: 0. 05 -0. 1 mg) o Na. Cl 1 -3 g o Recession of enlarged clitoris 4 -12 mo.

Synthetic steroid

Side effects of glucocorticoid
 2) 3) 4) 5) Electrolyte PRA 17 -OHP, androstenedione BA")
F/U of CAH 1) 2) 3) 4) 5) Electrolyte PRA 17 -OHP, androstenedione BA Growth, pubertal development
- Slides: 73