CONGENITAL HEART DISEASE Sophie Barbant MD Congenital Heart

CONGENITAL HEART DISEASE Sophie Barbant, MD

Congenital Heart Disease • Almost 1 / 100 babies born with CHD • Estimated 1 million adults in USA • More adults than children • Growth of population about 5% per year

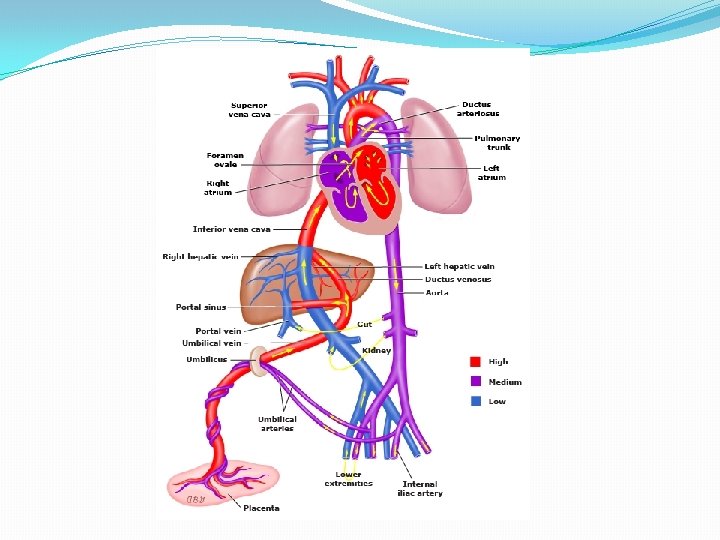
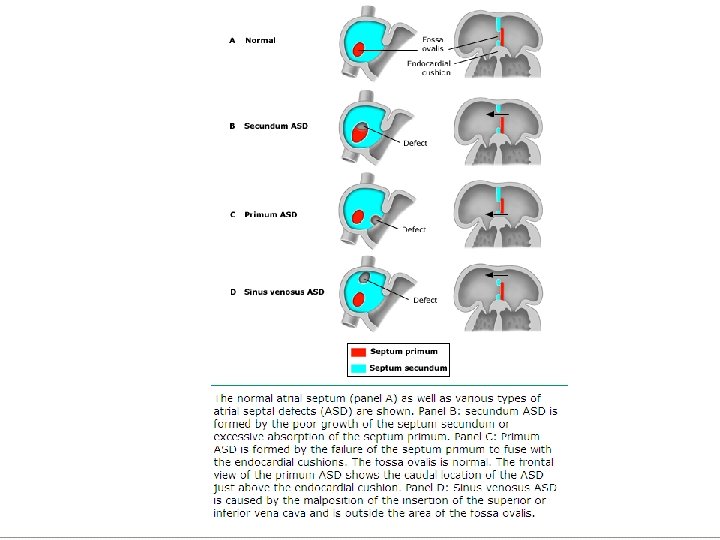
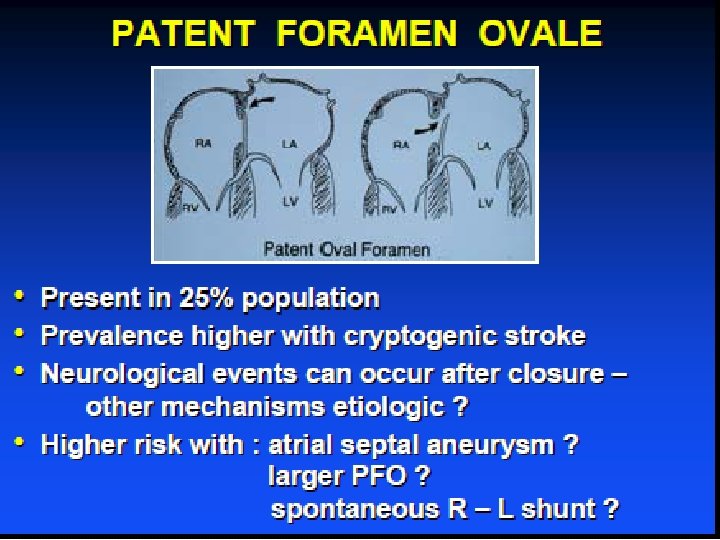
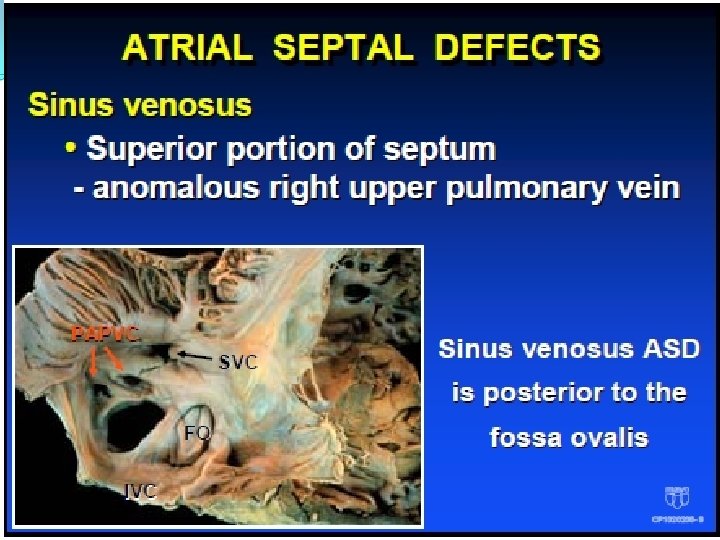
Congenital Heart Disease �ASD/PFO �Secundum ASD �Patent foramen ovale �Sinus venosus ASD �Primum ASD �VSD �PDA �Coarctation of the aorta

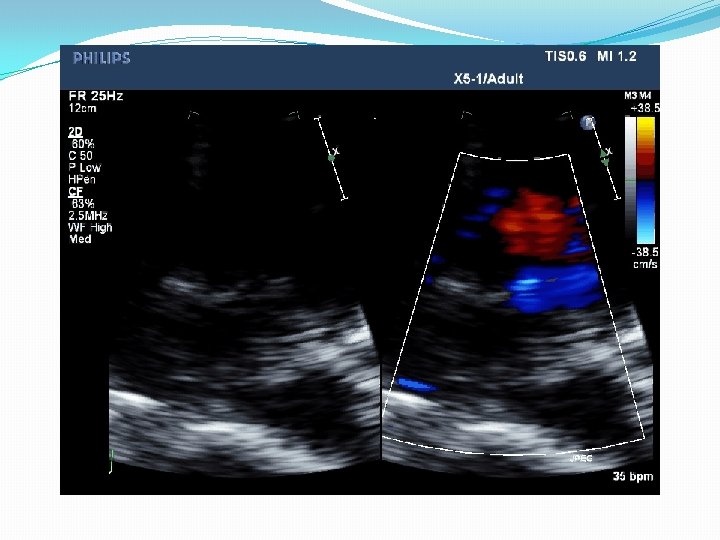
SECUNDUM ASD Signs • Normal or slightly ↑ JVP • RV heave • Ejection systolic murmur PA • Fixed split 2 nd sound • Tricuspid diastolic flow rumble
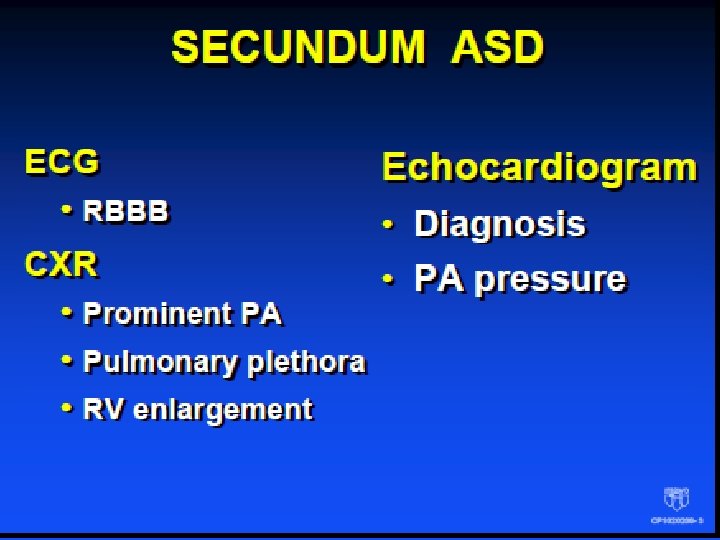

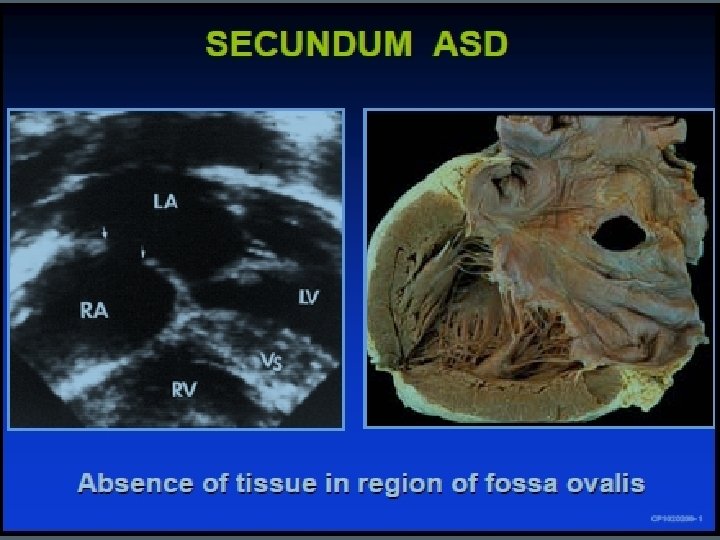
SECUNDUM ASD
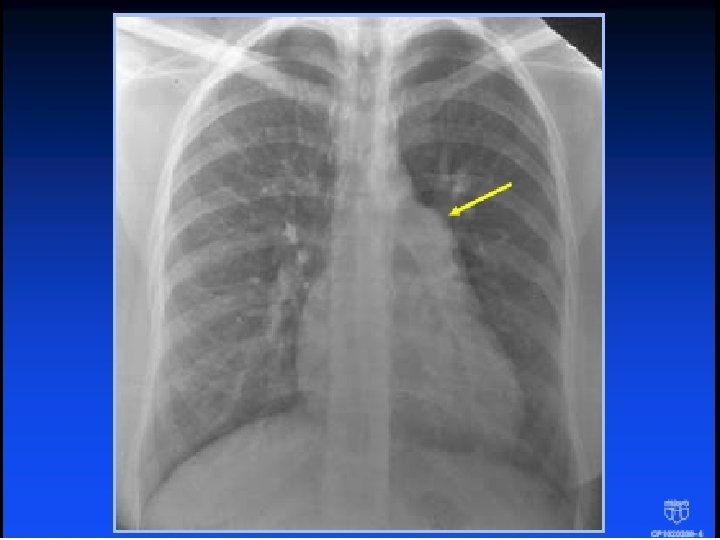

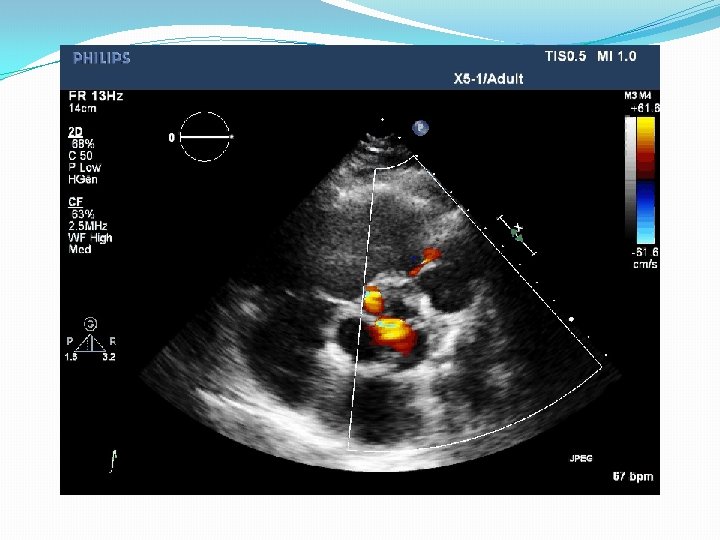
Quiz �The arrow shows: �A An enlarged left atrium �B An enlarged main pulmonary artery �C An enlarged right ventricle �D An enlarged aorta �E I don’t see anything abnormal

SECUNDUM ASD No LA enlargement unless • Patient > 40 years of age • Atrial fibrillation SECUNDUM ASD If LA enlarged, think primum ASD

SECUNDUM ASD Class III NOT RECOMMENDED Diagnostic cardiac catheterization is not indicated for uncomplicated secundum ASD in younger patients with adequate non - invasive imaging.

SECUNDUM ASD. Natural history = AF in the 50 s • Earlier the ASD is closed, the less likely to have AF and subsequent CVA
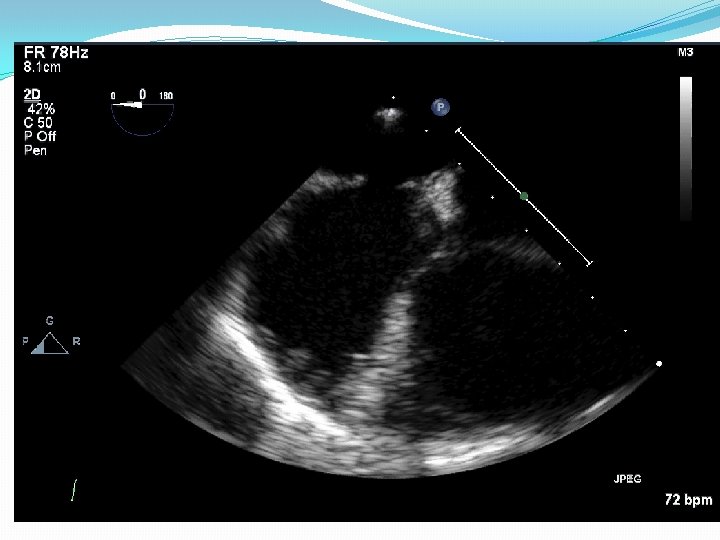

Secundum ASD

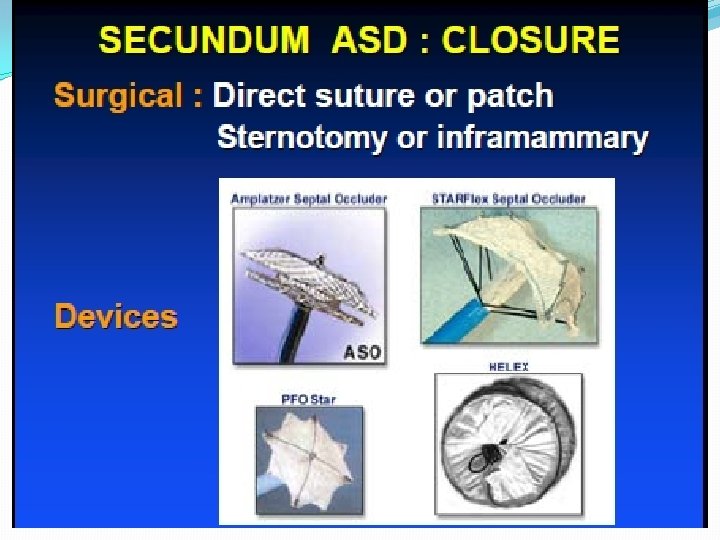
SECUNDUM ASD Management Class I Closure of ASD either percutaneously or surgically is indicated for RA and RV enlargement with or without symptoms Beware: CVA, AF, and pregnancy

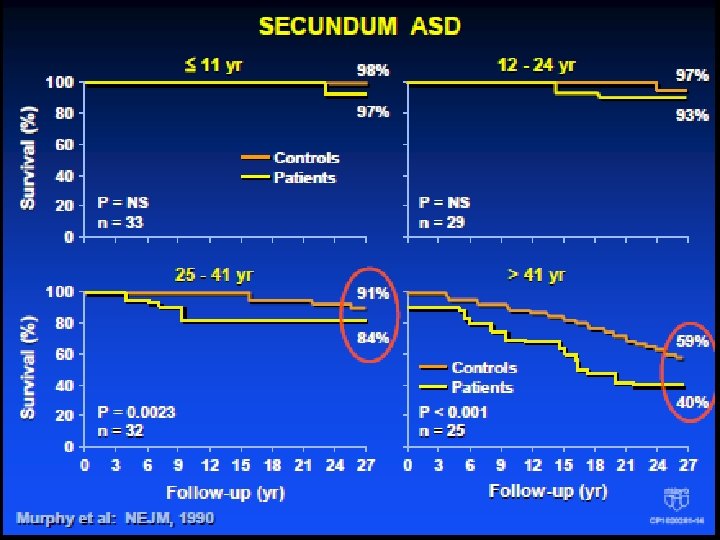
SECUNDUM ASD: Outcome after repair Outcome After Repair • 123 pt repaired 1956 - 60 • Symptoms present in 75% • Followed for 27 - 32 yr • Perioperative mortality 3. 3% • Pt repaired ≤ 25 yr long-term survival similar to age-matched controls
 • Inferior portion of")
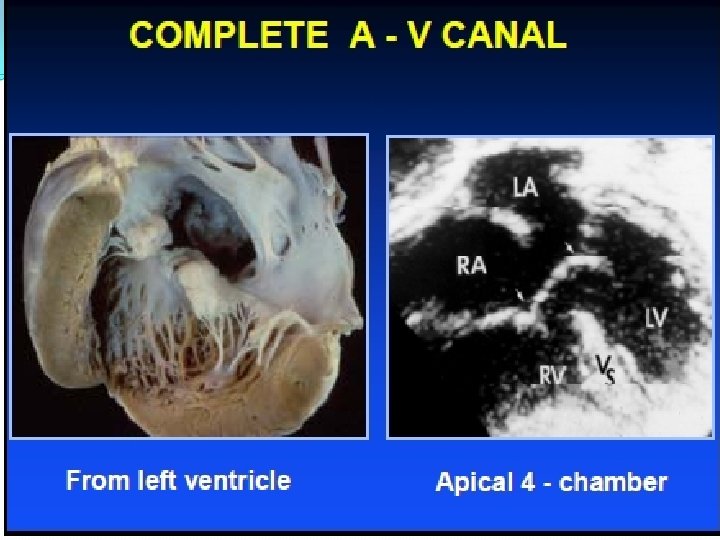
Atrial Septal Defects Primum ASD (partial A - V canal) • Inferior portion of septum - mitral valve usually cleft - often associated with Down’s syndrome.
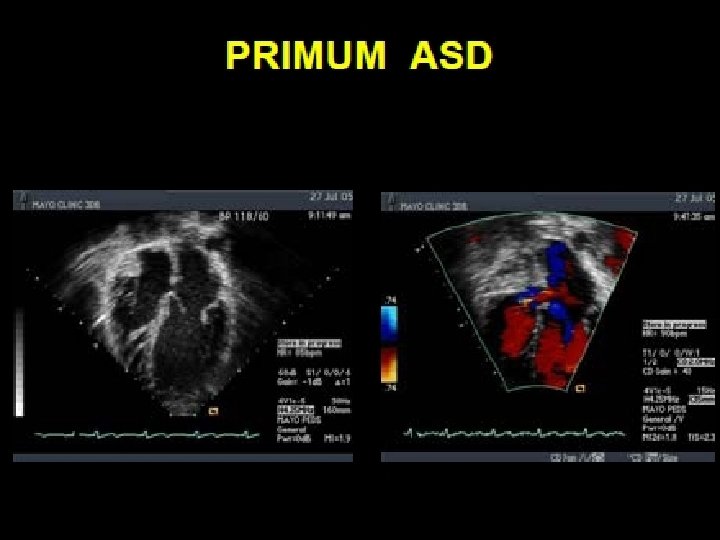

Cleft Mitral Valve

Primum ASD Associated lesions • Secundum ASD • VSD • PS • Subaortic stenosis • Left SVC • Coarctation

Ventricular Septal Defect Small defect • Loud holosystolic murmur at the lower left border, often thrill • Asymptomatic–no Rx Larger defect • Mitral diastolic flow rumble Large defect (Eisenmenger) • No murmur (LVp = RVp)

Ventricular Septal Defect Usually benign process • Muscular and membranous defects usually close spontaneously • Subaortic and subpulmonary defects even if small should be closed to prevent AR
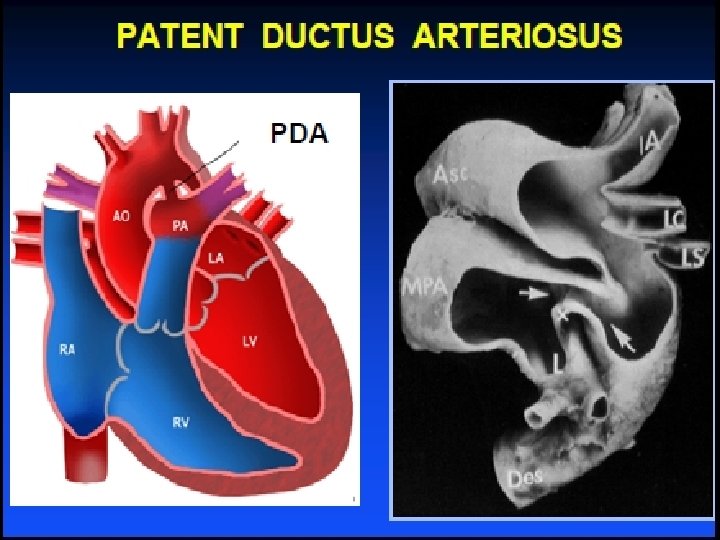

PDA physical examination Associated with maternal rubella • F: M=3: 1 • Brisk upstroke pulse : wide pulse pressure. ? thrill 2 nd left space • Continuous “machinery” murmur : envelops 2 nd sound

PDA Closure Class I LA or LV enlargement or PAH • Prior endarteritis Class II a Reasonable to close small asymptomatic small PDA by catheter device

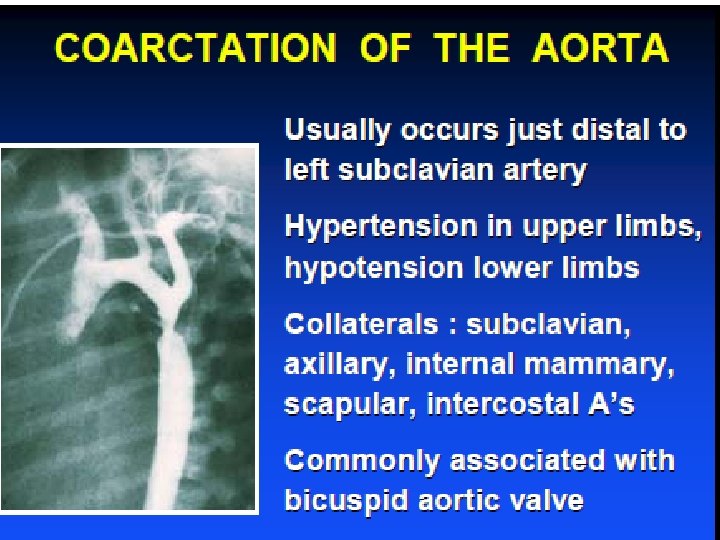


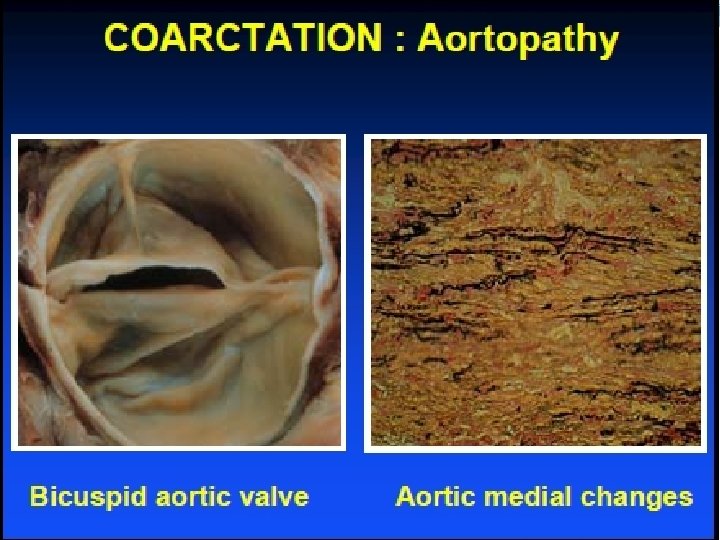
Coarctation Physical exam • Delayed femoral pulses BP difference in arms and legs • Systolic murmur left infraclavicular and under left scapula • Continuous murmur (collateral vessels) • S 4 with LVH and hypertension • Loud A 2 if hypertension • Ejection click ± systolic murmur with bicuspid aortic valve


Coarctation Diagnostic imaging • CXR Figure “ 3” sign – aortic knob Rib notching from intercostal As • Echo – Doppler • CT, MRI / MRA • Angiogram


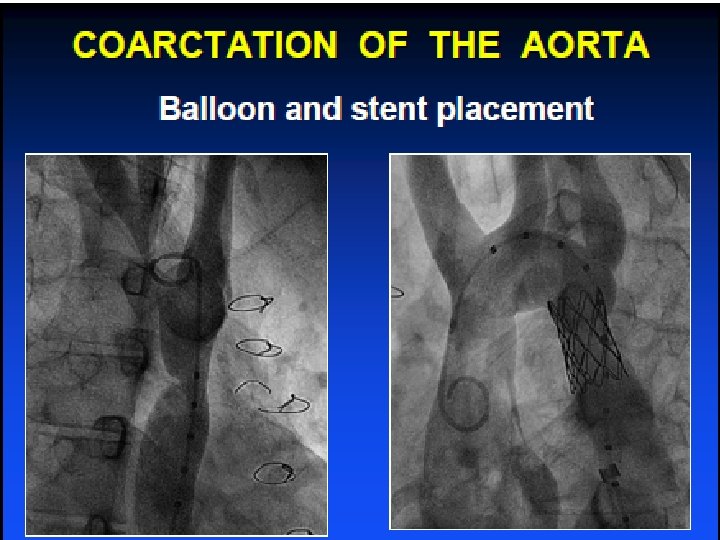
Coarctation Indications for intervention Class I Peak to peak gradient > 20 mm. Hg • Peak to peak gradient < 20 mm. Hg in presence of imaging evidence of significant coarctation with radiological evidence of significant collateral flow

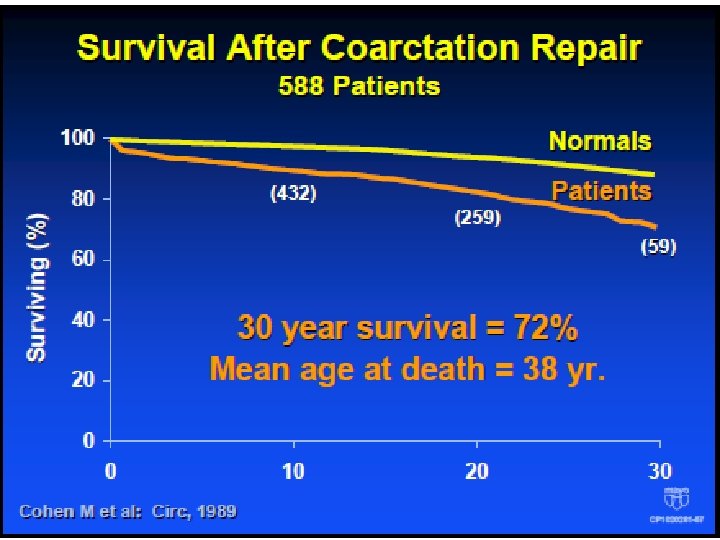
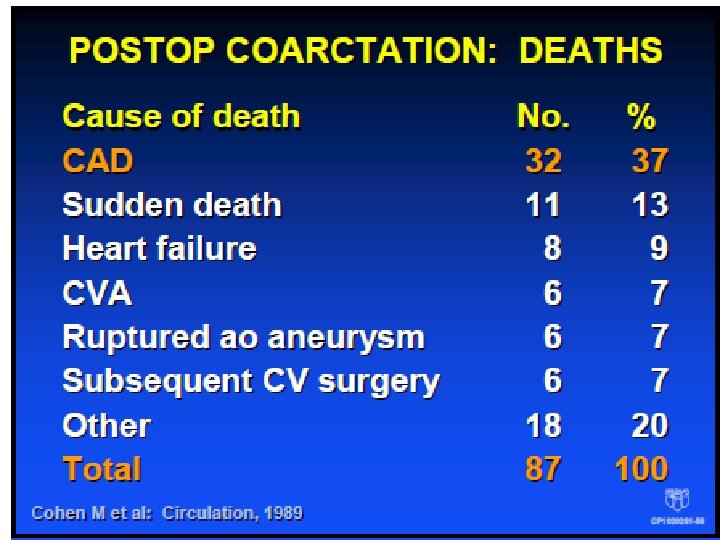
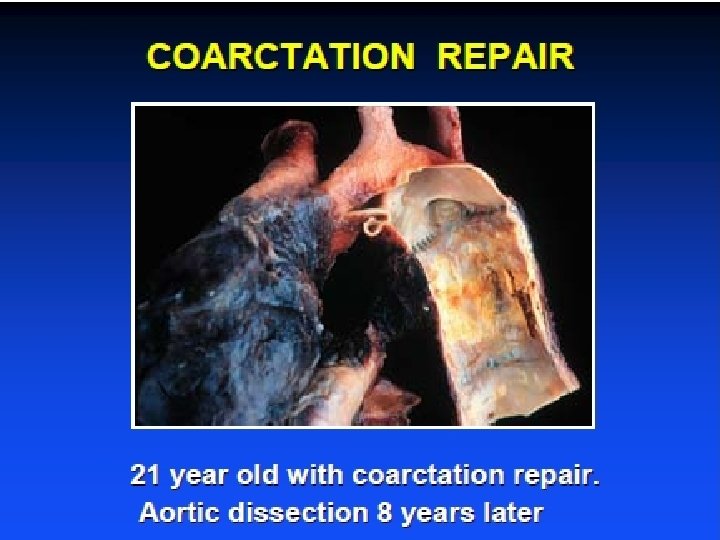
Coarctation High incidence of HTN at follow - up • 75% at 30 years Premature death due to • Coronary artery disease • Heart failure • Stroke • Aortic dissection or rupture Earlier age at repair = better survival
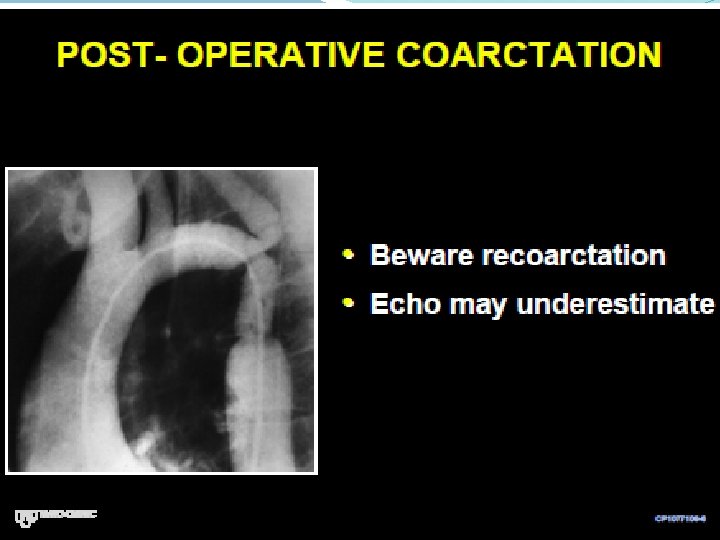
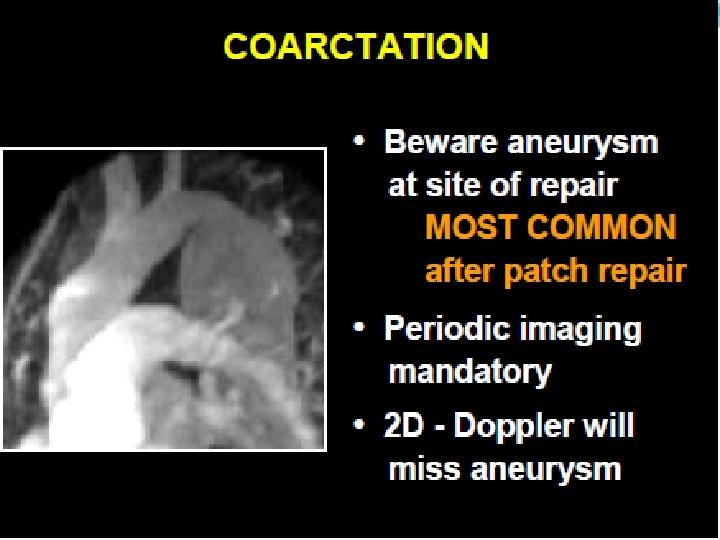

Coarctation repair Annual follow- up with meticulous control of BP at rest and exercise. B blockers • Imaging of entire aorta : ascending and coarctation site. Multimodality imaging • Screen for coronary disease and optimize risk factors • Offer cranial screening
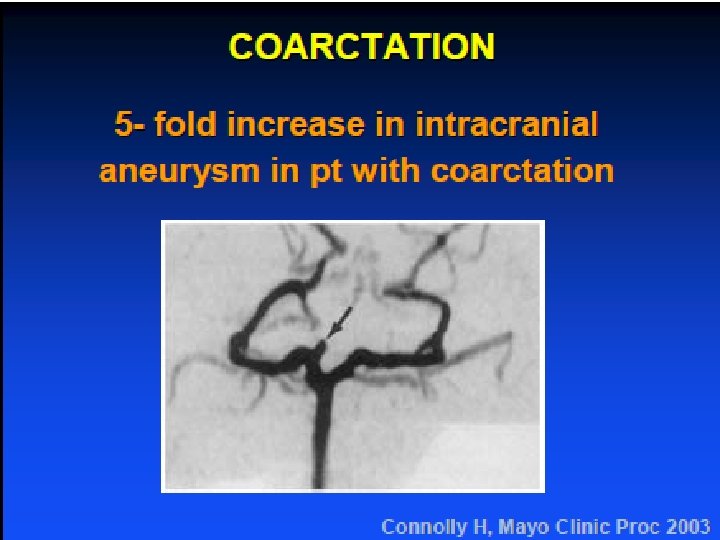

Coarctation conclusion Age at time of initial repair is a predictor of survival • Lifelong follow-up mandatory : BP control at rest and exercise. Imaging entire aorta. • CAD most common cause of late death. Risk factor modification important. • Assoc. CV anomalies requiring subsequent CV surgery are common

BE prophylaxis: dental procedures Class IIA Prosthetic cardiac valves Previous IE Unrepaired and palliated cyanotic CHD including surgically constructed shunts and conduits Repaired CHD with prosthetic materials (surgery or cath) for the first 6 mo after procedure Repaired CHD with residual defects at site or adjacent to site of prosthetic patch or device ( that inhibit endothelialization )

BE non dental procedures CLASS III NOT RECOMMENDED

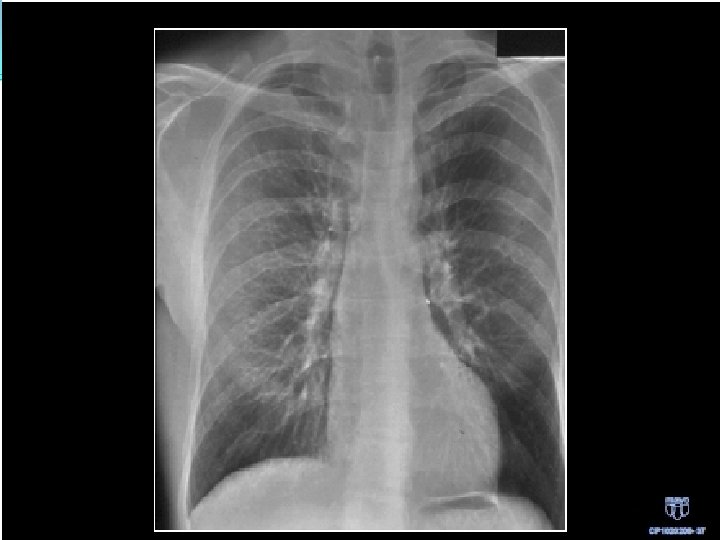
Which one of the physical signs would be expected with this chest X Ray? � A Wide Split 2 nd heart Sound � B Loud holosystolic murmur at the apex radiating to the axilla � C Loud holosystolic murmur at the lower left sternal border � D Delayed Femoral pulses � E Ejection systolic murmur in the pulmonary area

25 yr old male is evaluated during a routine examination. He has a history of aortic coarctation repaired in childhood. He is entirely asymptomatic. PE BP: 150/40 mm. Hg, HR: 80/min, CVP is normal. The carotid upstroke is brisk and collapses quickly. The apical impulse is displaced. 2/6 early systolic murmur in 2 nd ICS. 3/6 high pitched decrescendo diastolic murmur along left sternal border toward apex. There is evidence of nailbed pulsation. Femoral pulsations are full, collapse quickly, and there is no lag between the radial and femoral pulsations.

Which of the following is the most likely cause of this patients cardiovascular findings: A. Ascending aortic aneurysm B. Bicuspid aortic valve with aortic valve regurgitation C. Mitral valve prolapse with mitral regurgitation D. Recoarctation with associated systemic hypertension

Which of the following is the most likely cause of this patients cardiovascular findings: A. Ascending aortic aneurysm B. Bicuspid aortic valve with aortic valve regurgitation C. Mitral valve prolapse with mitral regurgitation D. Recoarctation with associated systemic hypertension

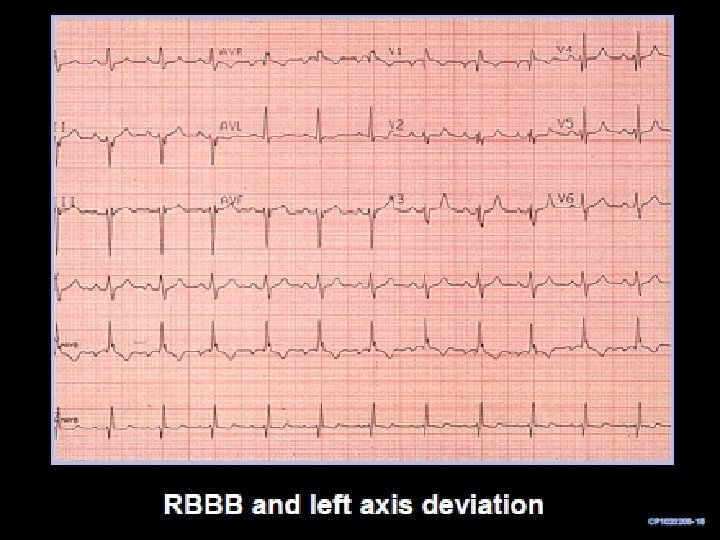
A 26 -year-old woman recently diagnosed with an ostium secundum atrial septal defect is evaluated to determine a treatment plan. She has no symptoms, but an exercise stress test demonstrates reduced exercise tolerance at 70% of predicted functional aerobic capacity. An EKG demonstrates normal sinus rhythm, first-degree atrioventricular block, and an incomplete right bundle branch block. A transthoracic echocardiogram demonstrates a 1. 5 -cm ostium secundum atrial septal defect with evidence of moderate right-sided cardiac chamber enlargement. There is no evidence of pulmonary hypertension by clinical evaluation or Doppler echocardiography.

Which of the following is the most appropriate next step in the management of this patient? A. Re evaluate in 12 months B. Recommend endocarditis prohylaxis C. Refer for atrial septal defect closure D. Start warfarin anticoagulation

Which of the following is the most appropriate next step in the management of this patient? A. Re evaluate in 12 months B. Recommend endocarditis prohylaxis C. Refer for atrial septal defect closure D. Start warfarin anticoagulation
- Slides: 67