Airway Management in the Critically Ill Dr CHAN











 n Mask seal ¨ Beard, n Obese / Obstruction ¨ BMI n")





 n")
 n Preoxygenation n Pretreatment n Paralysis with induction")
 n Assess for possible difficult airway n Assemble equipments and")
 n Assess for possible difficult airway n Assemble equipments and")



 n Large tongue (Macroglossia) n Protruding teeth n Short")






 n Assess for possible difficult airway n Assemble equipments and")





 n Preoxygenation (Time -5 mins) n Pretreatment n")
 100% oxygen for 5 minutes n 8 vital capacity breath")

 n Lignocaine n 1. 5 mg/kg ¨ Raised ICP ¨")
 n Ascertain everyone is ready n Sedative →")
 n Cricoid Pressure n Position patient n Do")




 n Check mandible for flaccidity n Insert Laryngoscope")





 n Preoxygenation (Time -5 mins) n Pretreatment (Time")















 ¨")
















 Hypoxia")








 by American Heart Association ACLS Provider Manual")
- Slides: 97
Airway Management in the Critically Ill Dr. CHAN King-chung June 7, 2006
Learning Airway Management
Case Scenario M/65 n Admitted for COAD exacerbation n Put on Bi. PAP n Found to be unresponsive n Sp. O 2 = 87%. BP = 160/90. HR = 120 n What would you do ? n
Indication for Airway n Obstruction n Assisted Ventilation n Aspiration n Secretion Clearance
Airway Obstruction
Opening Airway n Head tile, Chin lift n Jaw thrust
Oropharyngeal Airway
Insertion of Oral Airway
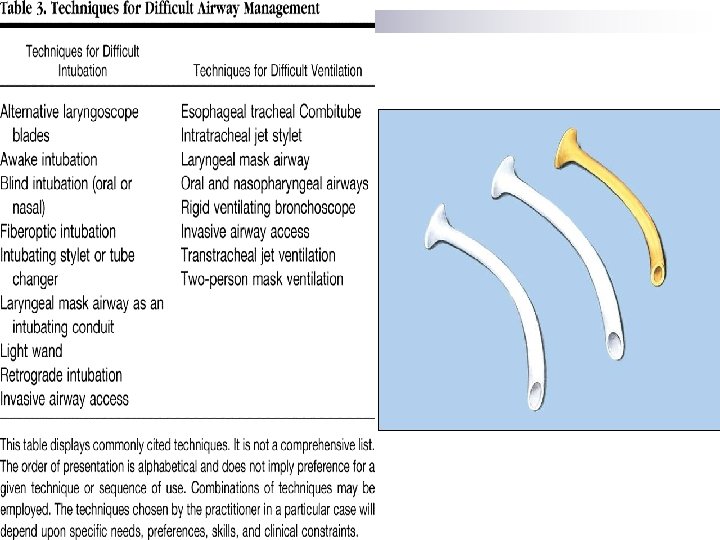
Nasopharyngeal Airway
Mask Ventilation 1 -Person: difficult, less effective 2 -Person: easier, more effective
Difficult Mask Ventilation n Leak around the mask n No clear chest expansion during ventilation n Ventilation possible only with 2 -person
Prediction (MOANS) n Mask seal ¨ Beard, n Obese / Obstruction ¨ BMI n n >26 Age ¨ >55 n facial injury years No teeth Stiff lung
Complications n Gastric distension n Aspiration n Pressure injury to eyes, nose or lips n Facial nerve palsy
Bag-Mask Ventilation
Rapid Sequence Intubation n Virtually simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation without interposed mechanical ventilation
Why RSI ? n Minimize risk of aspiration n Optimal intubating condition n High success rate
Success Rate Medical Trauma RSI 99. 8% 97. 7% No med 94. 7% 96. 3% Sedation only 95% 93. 7% Nasal 97% 98. 1%
7 Ps Preparation n Preoxygenation n Pretreatment n Paralysis with induction (Time Zero) n Protection and positioning n Placement with proof n Postintubation management n
7 Ps Preparation (Time -10 mins) n Preoxygenation n Pretreatment n Paralysis with induction (Time Zero) n Protection and positioning n Placement with proof n Postintubation management n
Preparation (T -10 mins) n Assess for possible difficult airway n Assemble equipments and prepare drugs n Attach monitors n Establish IV access
Preparation (T -10 mins) n Assess for possible difficult airway n Assemble equipments and prepare drugs n Attach monitors n Establish IV access
Difficult Intubation n Intubationist with >2 years of experience ¨ More than 3 attempts ¨ Intubation time >10 minutes
Chances of Difficult Airway Probability Difficult mask ventilation Uncertain Difficult intubation 1 - 4% Failed intubation 0. 05 - 0. 35% Difficult ventilation & Difficult intubation Cannot Ventilate & Cannot Intubate 1. 5% 0. 0001 - 0. 02%
Assessment of Airway n The LEMON rule ¨ Look externally ¨ Evaluate 3 -3 -2 ¨ Mallampati score ¨ Obstruction ¨ Neck Mobility
Look Externally Receding mandible (Micrognathia) n Large tongue (Macroglossia) n Protruding teeth n Short neck n Obese n Head & neck injury n
Look Externally
Evaluate 3 -3 -2 n Mouth opening ¨ Accommodate n Hyoid-Mental distance ¨ 3 n fingers Thyrohyoid distance ¨ 2 n 3 fingers (Thyromental distance >6 cm)
Mallampati Score I II IV Faucial pillars + - - - Uvula + + - - Soft palate + + + - Hard palate + + 0% 10% Grade 4 Larynx 33%
Assess this Lion
Obstruction Foreign body n Upper airway tumour n Epiglottitis n Peritonsillar abscess n Neck infection n Goitre n Haematoma n
Neck Mobility n Necessary for a good laryngoscopy view n Sternomental distance <12. 5 cm (normal 15 cm)
Preparation (T= -10 mins) n Assess for possible difficult airway n Assemble equipments and prepare drugs n Attach monitors n Establish IV access
Equipments for Intubation n Airway ¨ Oxygen & Ventilation ¨ Oxygen Source ¨ Mask (Various Size) ¨ Manual Resuscitator ¨ ¨ n Endotracheal Tube 7 -9 mm ETT ¨ Malleable Stylet / Bougie ¨ Syringe ¨ K-Y Jelly ¨ ¨ n Fixation ¨ Adhesive Tape Laryngoscope Blade (Size 3 first) Suction Small Pillow Magill Forceps Drugs Sedative ¨ Muscle Relaxant ¨ ¨ n Laryngoscopy Oral / Nasl Airway ¨ n n n Confirmation Stethoscope ¨ End-tidal CO 2 ¨ Oesophageal Detector ¨
Shape of ETT n Hockey Stick ¨ To manoeuvre within oral cavity ¨ Expect some resistance in removing stylet ¨ Lubricate stylet
Mc. Coy Laryngoscope
Sedation for Intubation n Etomidate 0. 2 mg/kg n More CV stable ¨ Adrenal suppression ¨ ¨ n n Midazolam 0. 1 mg/kg Convenient ¨ Infusion for sedation ¨ Less clear end point of induction Propofol 0. 5 mg/kg Thiopentone 1. 5 mg/kg ¨ ¨ n More hypotension Standard for neurosurgical patient Ketamine 1 mg/kg ¨ Increase BP
Muscle Relaxant n Suxamethonium n Rocuronium ¨ 1. 5 mg/kg ¨ 1 mg/kg ¨ 30 -45 s ¨ 60 s to full action ¨ Last 10 mins ¨ Fasciculation ¨ Increase K n n n Hyper K to start with Burn >24 hrs Spinal injury >24 hrs ¨ Increase ICP to full action ¨ Last 1 hour ¨ No fasciculation
7 Ps Preparation (Time -10 mins) n Preoxygenation (Time -5 mins) n Pretreatment n Paralysis with induction (Time Zero) n Protection and positioning n Placement with proof n Postintubation management n
Preoxygenation (T= -5 mins) 100% oxygen for 5 minutes n 8 vital capacity breath n (Not 100% on Sp. O 2) n n Provide store of oxygen during intubation
Time to Desaturation
Pretreatment (T= -3 mins) n Lignocaine n 1. 5 mg/kg ¨ Raised ICP ¨ Bronchospasm 0. 01 mg/kg ¨ Age < 10 years ¨ n Opioid Fentanyl 1 -3 ug/kg ¨ Raised ICP ¨ Coronary heart disease ¨ Atropine ¨ n Defasciculation 10% paralysis dose ¨ Rocuronium 0. 06 mg/kg ¨ Raised ICP ¨
Paralysis with Induction (T= 0 s) n Ascertain everyone is ready n Sedative → Relaxant → NS flush ¨ As quickly as possible ¨ Don’t flush between sedative & relaxant
Protection & Positioning (T= +30 s) n Cricoid Pressure n Position patient n Do not bag unless Sp. O 2<90 ¨ Increase risk of aspiration
Cricoid Pressure Cricoid: cartilage with a complete ring n Also called Sellick’s Manoeuvre n Firm pressure to prevent regurgitation n
Cricoid Pressure n Release ONLY after ET placement confirmed n BURP n Caution in patient with cervical spine injury n May support the back of the neck with another hand
Positioning n Sniffing position ¨ Head Extended, Neck Flexed
Positioning n No C-spine injury n n In-line immobilization Suspected C-spine injury
Placement with Proof (T +45 s) n Check mandible for flaccidity n Insert Laryngoscope n Intubate, remove stylet ¨ May use Bougie instead n Confirm placement n Release Cricoid Pressure
Laryngoscopy Grading Complete glottis visible Anterior glottis not seen Only epiglottis Epiglottis not seen
Signs of Successful Intubation n Non-fail-save signs ¨ Breath sound in chest ¨ No breath sound over stomach ¨ Chest rise and fall ¨ Moisture condensation on tube in expiration ¨ ‘Normal’ compliance on bagging ¨ CXR ¨ Hearing air exit from tube on chest compression ¨ Feeling of cartilage with Bougie ¨ Resistance upon passing Bougie / Suction catheter
Signs of Successful Intubation n Near-fail-save signs ¨ ETCO 2 n n (6 breaths / 1 min) False negative in cardiac arrest False positive after carbonated drinks ¨ Oesophageal n Detector Gastric distension
Signs of Successful Intubation n Fail-save signs ¨ Fiberoptic visualization of the bronchial tree ¨ Visualization of tube between cord n DL not always reliable
Postintubation Management n Secure Tube n CXR n Sedation +/- paralysis n Set ventilator
7 Ps Preparation (Time -10 mins) n Preoxygenation (Time -5 mins) n Pretreatment (Time -3 mins) n Paralysis with induction (Time Zero) n Protection and positioning (Time +30 s) n Placement with proof (Time +45 s) n Postintubation management n
Failed Intubation n Summon Help n Mask ventilation n Think about why n Change blade or intubator n Optimize patient n ? ? Impossible to intubate
Maintain Ventilation n Patient die not from failed intubation but failed ventilation Rescue from failed intubation is bagging n Rescue from failed bagging is ‘better’ bagging n n Another dose of relaxant often KILLS
Endoscopy Mask Able to pass bronchoscope and ETT n For bronchoscopic intubation if mask ventilation effective n
Fiberoptic Intubation n Cut tube to 26 cm before use n Fix the tube to the top end with tape n Open the airway with jaw thrust
Difficult Bagging n Insertion of oral / nasal airway n Other Airway adjuncts ¨ Laryngeal n Mask Airway Intubating Laryngeal Mask ¨ Combitube n Laryngeal Tube
Laryngeal Mask Airway
Position of LMA n Tip in oesophageal opening n Cover laryngeal opening n Air seal with inflatable cuff
Selection of LMA Size Weight Max Cuff Volume 1 <6. 5 kg 4 m. L 3. 5 2. 7 mm 2 6. 5 -20 kg 10 m. L 4. 5 3. 5 mm 2. 5 20 -30 kg 15 m. L 5 4 mm 3 30 -60 kg 20 m. L 6 (cuff) 5 mm 4 >60 kg 30 m. L 6. 5 (cuff) 5 mm Pass ETT FOB Size
Insertion of LMA 1 3 2 n Keep neck in flexion n Insertion difficult with Cricoid Pressure n Move out 1 to 2 cm upon inflation 4
Advantage of LMA n High success rate ¨ 87 -94% with only brief training n No muscle relaxation required n Conduit for subsequent intubation ¨ Fiberoptic / Bougie / 6 mm ETT
Disadvantage of LMA n Risk of Aspiration ¨ Partially n Failure Rate 1 to 5% ¨ Improve n reduced with the newer Proseal with training Airway obstruction with over inflation
LMA Insertion
Intubating Laryngeal Mask n Easier insertion ¨ Rigid n handle Designed for intubation ¨ Blind ¨ FOB guided
Inserting ILMA
Inserting ETT via ILMA
Combitube n Combitube ¨ Adult n > 5 ft Combitube SA (Small Adult) ¨ 4 - 5 ft
Insertion of Combitube
Advantage of Combitube n n Can be inserted in any position Minimized risk of aspiration No fixation needed after inflating oropharyngeal balloon IPPV at higher pressure n n Neck movement not necessary Little training Work in either tracheal or oesophageal position No preparation necessary
Problem with Combitube n Clearance of airway secretion no possible n No conduit to change to ETT
Contraindication n Intact gag reflex n Under 4 feet n Central airway obstruction n Known oesophageal pathology n Caustic ingestion
Combitube Insertion
Laryngeal Tube Similar to Combitube n Conduit available for tracheal access n
Sizes of Laryngeal Tube Size Patient Size Colour Volume 0 Newborn <5 kg Transp. 10 m. L 1 Infant 5 -12 kg White 20 m. L 2 Child 12 -25 kg Green 35 m. L 3 Teenage <155 cm Yellow 60 m. L 4 Adult 155180 cm Red 80 m. L 5 Large Adult >180 cm Pruple 90 m. L
Cannot Intubate / Ventilate n Patient will DIE in minutes n Continue with mask ventilation despite difficulties Call Surgeon for surgical airway n ? Trial of of Combitube n Prepare for Cricothyrotomy n
Cricothyrotomy n Last resort for cannotintubate, cannot-ventilate n Surgical Cricothyrotomy n Needle Cricothyrotomy ¨ Require jet ventilation
Needle Cricothyrotomy
Needle Cricothyrotomy
Difficult Cricothyrotomy Surgery of neck n Haematoma, infection, or other neck swelling n Obesity n Radiation distortion n Tumour of the neck n
Percutaneous Tracheostomy n Elective procedure n At least 2 doctors ¨ Surgeon ¨ Anaesthetist n / Airway management Usually under LA & sedation
Advantage n Lower risk of infection ¨ OR n Lower incidence of bleeding ¨ OR n n = 0. 29 (0. 12 - 0. 75) Lower mortality ¨ OR n = 0. 28 (0. 16 - 0. 49) = 0. 71 (0. 50 - 1. 0) Similar major peri-procedural complications Similar long-term complications Crit Care. 2006 Apr 7; 10(2): R 55
Contraindications n Emergency airway n Tracheomalacia n Infection of the neck n PEEP > 15 cm. H 2 O n Obesity with short neck n Age <15 years n Bleeding diatheses n Distortion of the neck anatomy ¨ ¨ ¨ PT/APTT > 1. 5 x normal Platelet count <50 Bleeding time > 10 mins ¨ ¨ ¨ Hematoma Tumor Thyromegaly High innominate artery Scarring from previous neck surgery
Procedure n n ETT withdrawn before starting Dilation methods 1 2 3 4 ¨ Serial ¨ Blue Rhino ¨ Giggs Forceps ¨ Percutwist n Bronchoscopic monitor for beginners
Complications n Immediate ¨ ¨ ¨ ¨ Death 0. 4% Haemorrhage (2. 5%) Hypoxia False Passage (0. 8%) Posterior Tracheal Wall Perforation Surgical Emphysema Tension Pneumothorax Accidental Extubation n Early Post-op Haemorrhage ¨ Stomal Infection (1%) ¨ Excessive Granulation tissue ¨ Tracheal Arterial Fistula ¨ n Late Post-op (>6 m) Tracheal Stenosis (2%) ¨ Tracheocutaneous Fistula ¨ Voice Change (up to 50%) ¨ Disfiguring scar (4%) ¨
Dislodged Tracheostomy n Confirm dislodgement ¨ Cannot pass suction catheter ¨ No ETCO 2 Remove Tracheostomy tube n Do not re-insert tracheostomy if track is not formed (< 1 to 2 weeks) n Start mask ventilation n Reintubate trans-laryngeally n
Changing ETT n Adequate fasting n Sedation + paralysis n Cook’s Airway Exchange Catheter ¨ NOT Bougie as it has to be at least twice the length of ETT
Cook’s Catheter
Procedure
Procedure
Procedure
Procedure
Reference n Video on the use of various adjuncts ¨ n Use of LMA ¨ n http: //www. lmana. com/prod/components/education_center. html Percutaneous Tracheostomy ¨ n http: //www. trucorp. co. uk/sections/insertion. asp http: //www. emedicine. com/ent/topic 682. htm General airway management http: //theairwaysite. com/education. html ¨ http: //www. aic. cuhk. edu. hk/web 8/Airway. htm ¨
Reference n n BLS Provider Manual (2006) by American Heart Association ACLS Provider Manual (2003) by American Heart Association Airway Management: Principles and Practice (1995) by Benumof et. al. Manual of Emergency Airway Management (2004) by Walls et. al.