Pediatric ED Case Conference Date 20060425 Presented by

Pediatric ED Case Conference Date: 2006/04/25 Presented by R 1 劉政忠 Instructor: MA 張玉吉吉 醫師 MA 吳孟書 醫師

General data w Name: 張X浩 w Chart number: 20947975 w Age: 3 week 2 day-old w Gender: Male w Body weight : 3 kg
 w T:")
Vital sign w 2006 -3 -29 12: 43 (0 hr 0 min) w T: 36 , P: 165 , R: 65 w E 4 V 5 M 6, Sp. O 2: 93% w 檢傷分類: 3級 w 病患主訴因食慾差 w Chief complaints: SOB for 2 days
 w")
Present illness w Vomiting for 2 days w No cough w Poor appetite(+) w 看起來很乾?

Past history w Nil

PAT w Appearance: ? w Breathing: tachypnea w Circulation: ?

Physical examination w General appearance: poor activity w HEENT: lip cyanosis, dry lip w Chest: bil coarse BS, wheezing(+), rales(+), retraction(+) w Heart: RHB w Abdomen: ? w Extremity: ? w Skin: ?

ED initial impression w r/o GER w r/o aspiration pneumonia

Further history taking w Dyspnea? Cough? Foreign body? Cyanosis? w Vomiting? Content? Projectile? Feeding? Diarrhea? Urine amount? Body weight change? w Fever? w Activity? Appetite? w Drug hx? w Birth hx: BBW? IUGR? Preterm baby? CHD? w Maternal hx: GDM? PROM?

Further PE w Appearance: TICLS w HEENT: frontanelle, tears, dry mouth or mucosa, throat, nasal flaring, accessory muscle use w Chest: retraction, breathing sound w Heart: murmur w Abdomen: soft or distension, tenderness, bowel sound, umbilicus, mass w Skin: rash, turgor, pallor, cyanosis, CRT
 w Birth hx: G 1 P 1 GA: 39+weeks,")
Detail Hx from admission note(1) w Birth hx: G 1 P 1 GA: 39+weeks, NSD, APGAR score? Born in LMD, BBW: 2850 g, BH: 50 cm, NB screen: ? w Drug hx: 八寶粉topical use? w Vaccine: HBV on 95 -3 -10 w Maternal hx: 20 y/o, G 1 P 1, No maternal fever , no PROM , no chorioamnionitis, no maternal GDM , no PIH , no eclampsia , and no use of drug during pregnancy
 w 3 days ago…. w Vomiting w decreased appetite")
Detail Hx from admission note(2) w 3 days ago…. w Vomiting w decreased appetite (80~100 cc to 20~30 per meal) w progressive tachypnea, cyanosis when feeding w BW: 2850 to 2880 g (<3 rd percentile)
 w General appearance : ill looking, poor activity and")
Detail PE from admission note(1) w General appearance : ill looking, poor activity and irritable w HEENT : grossly normal , no facial dysmorphism , no anterior or posterior frontanel bulging , no icteric sclera , no neck mass , no periorbital edema w Heart : regular heart beat , no murmur w Chest : coarse breath sound , no wheeze , no rales , tachypnea and obvious subcostal or supraclavicular retraction , mild nasal flaring
 w Abdomen : soft , flat , no distension")
Detail PE from admission note(2) w Abdomen : soft , flat , no distension , normoactive bowel sound , no abnormal palpable mass , no pus discharge from umbilical area, no hepatosplenomegaly, no perianal redness w Genital organ : grossly normal w Extremity : no edema, distal four limb : warm and pink , no limb cyanosis , peripheral pulse palpable , capillary refill time < 2 sec w Skin: no rash w Neurologic examination : muscle power : +5/+5 , no hypotonia

How about this baby? w Respiratory distress + dehydration + poor activity => ? n n n Infection: pneumonia, UTI, viral infection… Endocrine and metabolism: electrolyte imbalance, Inborn errors of metabolism, Hypoglycemia… GI: pyloric stenosis, AGE, T-E fistula, obstruction…
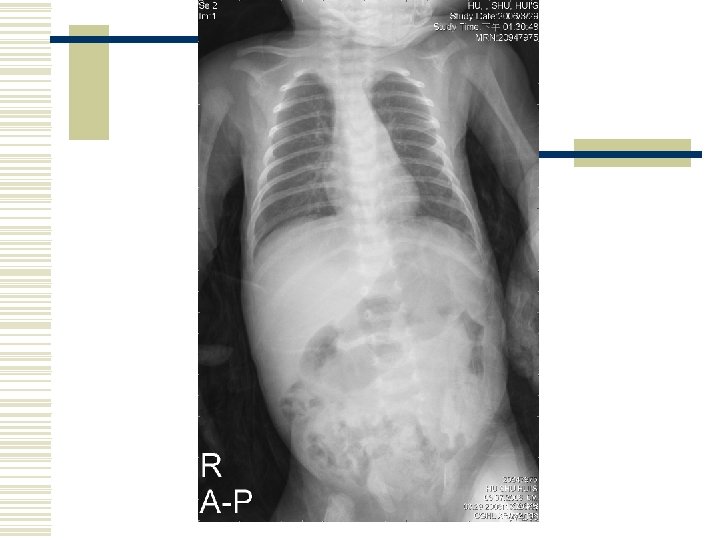
 w CXR w CBC/DC, CRP,")
Initial order 3/29 13: 18 (0 hr 35 min) w CXR w CBC/DC, CRP, AST, ALT, BUN, Cr, Na, K, Cl, Ca, sugar, CRP, B/C*1 w IVF: D 5 S 1/4 run 15 cc/hr w O 2 hood w A+B inhalation st w NPO

Lab—hemogram w w w w w WBC Hemoglobin Hematocrit Platelets Segment Band Lymphocyte Monocyte Eosinophil 21400 15. 5 43. 9 60000 48. 0 % 1. 0 % 41. 0 % 5. 0 %
 Creatinine(B) AST (GOT) ALT/GPT Calcium")
Lab--biochemistry w w w w w Sugar BUN (B) Creatinine(B) AST (GOT) ALT/GPT Calcium Na K Cl CRP 615 !! 17 0. 5 23 22 10. 4 125 5. 7 96 0. 83
 w Admission to NICU")
3/29 14: 45(2 hr 02 min) w Admission to NICU
 w IVF 改 half saline run 15 cc/hr")
3/29 15: 10(2 hr 27 min) w IVF 改 half saline run 15 cc/hr w 補ketone body(B) => 3+

Admission impression w Vomiting and severe dehydration w Severe metabolic acidosis w Respiratory distress and cyanosis episode, r/o sepsis w Leukocytosis and thrombocytopenia
 w w w w IVF: D 2. 5")
Admission order 3/29 16: 06(day 1) w w w w IVF: D 2. 5 S 1/2 IV+ PO 140 cc/q 8 h (150 cc/kg/day) NPO Check F/S stat and q 8 h On OG tube U/C, U/A, urine GBS Ag Sugar, NA, K, Ca, Cl, ABG Ampicillin 70 mg q 6 h iv + GM 7 mg q 8 h ivf

U/A w w w w Color Turbidity SP. Gravity p. H Leukocyte Nitrite Protein Glucose Yellow Clear 1. 025 5. 0 Negative 1. 000 w w w w Ketone 2+ Urobilinogen 0. 1 Bilirubin Negative Blood 2+ RBC 6 WBC 0 Epith-Cell 0

ABG and biochemistry w w w w TEMP PH PCO 2 PO 2 HCO 3 SBE SAT 37°C 7. 148 7. 0 130. 5 2. 4 -26. 5 97. 9% w w w w Sugar 715 Calcium 10. 3 Na 128 K 4. 8 Cl 96 AG: 29. 6 Osmo(C): 301. 7
 w 16: 20 on nasal CPAP w 16: 45")
Hospital course 3/29 (day 1) w 16: 20 on nasal CPAP w 16: 45 NS challenge 40 cc, jusomine 8 m. L ivf w 21: 00 F/S: 524 N/S challenge 30 cc IVF 改 HS run 40 cc/hr RI 10 U in N/S 500 rum 3 m. L/hr w 21: 25 on endo
 w 01: 00 F/S: 266, RI line 改run 2")
Hospital course 3/30 (day 2) w 01: 00 F/S: 266, RI line 改run 2 m. L/hr w 07: 00 jusomin 8 m. L ivf IVF改D 0. 225 + 5 m. L KCl run 140/q 8 h consult endocrine check Osmo(B): 301 => OG: normal w 23: 00 F/S: 216 RI line改run 0. 5 m. L/hr
: extubation DC RI line 改 NPH 0. 5 U")
Hospital course w 3/31(day 3): extubation DC RI line 改 NPH 0. 5 U SC q 8 h w 4/1(day 4): try feeding w 4/4(day 7): DC anti w 4/6(day 9): NPH 1 U SC q 8 h w 4/12(day 15): 轉5 L w 4/17(day 20): 轉7 L, NPH 1. 25 U SC q 8 h w 4/18(day 21): MBD and OPD F/U

Other study during hospitalization w Abdominal echo=> negative findings w Serum amylase and lipase=> normal w C peptite=> 0. 34(low 0. 47~3. 15) w Insulin antibody=> P 11. 0(>10) w Hb. A 1 C=> 9. 6. % w Urine GBS Ag, U/C and B/C=> negative
 under NPH control, complicated with DKA")
Final diagnosis 1. Neonatal DM (type 1 DM) under NPH control, complicated with DKA and severe dehydration 2. Thrombocytopenia post blood transfusion 3. Respiratroy distress due to severe metabolic acidosis with respiratory compensation

Discussion DDx of hyperglycemia in infant DKA in childhood Management of DKA Neonatal DM
 w Infectious: Bacterial sepsis, Meningitis, Urinary tract infection, Viral infections…")
The ill-appearing infant: DDx(1) w Infectious: Bacterial sepsis, Meningitis, Urinary tract infection, Viral infections… w Cardiac: CHD, SVT, MI, Pericarditis, Myocarditis, Kawasaki disease w Endocrine: CAH w Metabolic: Hyponatremia, hypernatremia, Cystic fibrosis, Inborn errors of metabolism, hypoglycemia Textbook of Pediatric Emergency Medicine, 5 th edition
 w Drugs/toxins—aspirin, carbon monoxide w Hematologic: Severe anemia, Methemoglobinemia w")
The ill-appearing infant: DDx(2) w Drugs/toxins—aspirin, carbon monoxide w Hematologic: Severe anemia, Methemoglobinemia w Gastrointestinal: Gastroenteritis with dehydration, Pyloric stenosis, Intussusception, Necrotizing enterocolitis, Appendicitis, Volvulus w Neurologic: Infant botulism, Child abuse=> ICH Textbook of Pediatric Emergency Medicine, 5 th edition

Hyperglycemia in infant: DDx More often in premature infant w Excess glucose administration n IVF, feeding w Inability to metabolize glucose n Premature, sepsis, stress w Neonatal DM n Rare, 2 days ~ 6 weeks, C-peptide may be normal or transiently low w Medications n Caffine, theophylline, steroid, phenytoin w Type 1 DM n Vary rare, low to absent C-peptide level LANGE clinical manual, Neonatology: management, principle, on-call problems, disease and drugs. 5 th edition(2004)

DKA in childhood w Type 1 diabetes: the most common pediatric endocrine disorder w Prevalence: 1/400 w Islet-cell autoantibody, insulin antibody, glutamic acid decarboxylase antibody w 27 ~ 40% of new-onset diabetics present in DKA w The leading cause of mortality in diabetics < 24 y/o w cerebral edema: the leading cause of mortality

Definition w metabolic acidosis (p. H <7. 25 to 7. 30 or serum bicarbonate <15 m. Eq/L) w hyperglycemia (serum glucose >300 mg/d. L) w ketonemia

Clinical feature w Polyuria, polydipsia, dehydration, ketotic breath, hyperpnea, nausea, vomiting, abdominal pain, general malaise, coma w The most common cause: poor compliance w Viral illness and focal infections such as urinary tract infection or gastroenteritis

Life-threatening complications w Cerebral edema w Cardiovascular collapse w Profound metabolic acidosis w Hyperkalemia w Hypophosphatemia

Risk Factors for Cerebral Edema in DKA w Elevated BUN w Low PCO 2 w Treatment with bicarbonate w Failure of measured serum [Na] to rise steadily with correction of hyperglycemia w Age <3 y w New-onset diabetes

Initial lab evaluation w w w w CBC Glucose Electrolyte (Na, K, Ca, P, Cl) blood gas Serum osmolality ketones Urinary ketones Lactate
 w 10– 20 m. L/kg NS bolus until hemodynamically stable w Then begin")
Management(1) w 10– 20 m. L/kg NS bolus until hemodynamically stable w Then begin 0. 45% NS(or 0. 9%NS) at 1. 5 times maintainance w K (if patient is urinating) n n n <5. 5 m. Eq/L=> add 30 m. Eq/L. 2. 5– 3. 5 m. Eq/L=> add 40 m. Eq/L <2. 5 m. Eq/L=> consider adding more
 w RI at 0. 1 units/kg/hr after intravenous fluid bolus. Adjust dose to")
Management(2) w RI at 0. 1 units/kg/hr after intravenous fluid bolus. Adjust dose to maintain glucose decline at 50– 100 mg/d. L/hr. w Add dextrose to intravenous fluids when BS is <200– 250 mg/d. L.
 w Avoid bicarbonate therapy in DKA. Only consider n n n arterial p.")
Management(3) w Avoid bicarbonate therapy in DKA. Only consider n n n arterial p. H<6. 9 impaired cardiac contractility and vascular tone life-threatening hyperkalemia. w Follow serum electrolytes q 2 h. w Follow serum glucose every hour
 w Hyperglycemia that occurs during the first one month of life")
Neonatal DM, NDM(1) w Hyperglycemia that occurs during the first one month of life w Require insulin tx and last more than 2 weeks w A rare dx with incidence: 1/500000 neonates w IUGR, SGA, hyperglycemia, dehydration, glucosuria, acidosis with or without ketouria Permanent neonatal diabetes mellitus manifesting as diabetic ketoacidosis. Journal of the Formosan Medical Association. 102(12): 883 -6, 2003 Dec.
 w Transient NDM n n Insulin can be discontinued after several weeks or")
NDM(2) w Transient NDM n n Insulin can be discontinued after several weeks or months Maturational delay of the adenyl cyclase-c. AMP system of islet cells w Permanent NDM n n pancreatic agenesis or hypoplasia or absent beta cells Gene mutations: ATP-sensitive potassium channel subunit Kir 6. 2 w Type 1 DM n n Autoimmune dx Manifests later in life Permanent neonatal diabetes mellitus manifesting as diabetic ketoacidosis. Journal of the Formosan Medical Association. 102(12): 883 -6, 2003 Dec.
 w In a series of 57 infants with NDM w 18=> Transient w")
NDM(3) w In a series of 57 infants with NDM w 18=> Transient w 13=> Transient with recurrence between 7~20 y/o w 26=> Permanent Long-term course of neonatal diabetes. N Engl J Med 1995; 333: 704.
 Case 1 33 days 3200 Duration")
Case report of TNDM Age of onset BBW(gw) Case 1 33 days 3200 Duration of Insulin tx 5 months Case 2 49 days 3400 4. 9 months Case 3 49 days 2400 10 months Case 4 60 days 1300 2 weeks Different faces of non-autoimmune diabetes of infancy. Acta Paediatrica. 87(1): 95 -7, 1998 Jan

Case report of PNDM w A case of PNDM in a 3 -day-old female infant. w This full-term neonate was born small for gestational age. w Respiratory distress, poor activity, hypothermia, poor feeding, dehydration, and ketoacidosis. w After insulin therapy and fluid replacement, her condition became stable. w Serum C-peptide level to be low for her age. w During the first year of life she had catch-up growth, but insulin therapy was still required. Permanent neonatal diabetes mellitus manifesting as diabetic ketoacidosis. Journal of the Formosan Medical Association. 102(12): 883 -6, 2003 Dec.
 w All children(5) diagnosed as having PNDM between 1991 and 1995")
PNDM in Oman(1) w All children(5) diagnosed as having PNDM between 1991 and 1995 in Oman were included in the study w The mean incidence: 2. 2 per 100 000 live births/year w IUGR was noted in all (mean BBW 1. 86 kg) w DKA in 80% w Circulating islet cell antibody: (-) Permanent neonatal diabetes mellitus: clinical presentation and epidemiology in Oman Archives of Disease in Childhood Fetal & Neonatal Volume 80(3), May 1999, pp 209 F-212 F
")
PNDM in Oman(2)

Thanks for your attention!!
- Slides: 51