Nutrition Management in Critically Ill Patients Lana Gettman










 Dosing of EN")
 • • • Pulmonary failure Renal failure Hepatic failure Acute")



")
 NRS 2002 NUTRIC • Risk • High risk – NRS")
 (Quality of Evidence: Very Low) Simplistic")

 Albumin Pre-albumin • T ½ = 21 days")


 vs delayed EN, mortality. Stephen A. Mc. Clave")
 vs delayed EN, infectious complications. Stephen A. Mc.")
 vs parenteral nutrition (PN), infectious complications. Stephen A. Mc.")














 Hepatic failure (cirrhosis) -Use dry weight or usual weight to")
 vs enteral nutrition (EN) in severe acute pancreatitis, mortality.")
 vs enteral nutrition (EN) in severe acute pancreatitis, infections.")




 • Provide EN within 24 hrs postoperatively –")


 BMI 30 -50 >50 Weight-based energy requirements 11")
 BMI 30 -40 >/=40 Protein requirements 2 g/kg")





- Slides: 57
Nutrition Management in Critically Ill Patients Lana Gettman, Pharm. D. Harding University College of Pharmacy AAHP Fall Seminar September, 2016
Learning Objectives • Describe metabolic and nutritional changes during critical illness. • Discuss nutrition assessment in the ICU patients. • Review current guidelines for provision of nutrition support in adult critically ill patients.
Definition of a Critically Ill Patient • American Association of Critical-Care Nurses – “Critically ill patients are defined as those patients who are at high risk for actual or potential lifethreatening health problems. The more critically ill the patient is, the more likely he or she is to be highly vulnerable, unstable and complex, thereby requiring intense and vigilant nursing care”.
Nutrition and Malnutrition in the Critically Ill Patient • Nutrition plays a key role for recovery from illness • Up to 50% of critically ill patients have preexisting nutritional disorders • Patients who are well nourished prior to ICU admission, develop nutritional disorders rapidly – Metabolic demands of illness and healing – Rapid fluid shifts – Loss of specific vitamins and trace elements • Extent of muscle wasting and weight loss is inversely correlated with long-term survival 5
Physiological Changes During Critical Illness Imbalanced hormone levels: catecholamines, cortisol, glucagon, growth hormone, insulin Excess liver glucose production Excess catabolism Insulin resistance Increased production of proinflammatory cytokines
Catabolism and Urine Urea Nitrogen • Protein breakdown • Loss of nitrogen in the urine in the form of urea 16 -24 g/day in critically ill vs 10 -12 g/day in healthy individuals – Loss of 16 g N as urea = loss of 1 lb of skeletal muscle/lean body mass per day • Functional impairment – Respiratory muscles respiratory failure – Heart muscles heart failure – GI mucosa muscles diarrhea • Rapid development of malnutrition 7
Results and Manifestations of Malnutrition in Critical Illness Results Manifestations • Loss of body cell mass • Changes in fluid/electrolytes/mineral homeostasis • Organ dysfunction • Impaired immune function • Prolonged dependence on mechanical ventilation • Increased rates of infection
Terminology Nutrition Support Nutrition Therapy • Adjunctive care to provide exogenous fuels to preserve lean body mass and support the patient throughout the stress response • Help reduce the metabolic response to stress, prevent oxidative cellular injury, and favorably modulate immune response • Achieved by – Early enteral nutrition (EN), appropriate macro-and micronutrient delivery, “meticulous glycemic control” • Potential outcome – Reduce disease severity, decrease complications, decrease length of stay (LOS) in the ICU, favorable patient outcomes
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A. S. P. E. N. ) • Target Patient Population – Adult (>/=18 years) critically ill patient expected to require length of stay greater than 2 -3 days in MICU or SICU who cannot sustain “volitional intake” – Patients with organ failure (lungs, liver, kidney), acute pancreatitis, traumatic brain injury, open abdomen, burns, sepsis, post-op major surgery, chronic critically ill, and critically ill obese Journal of Parenteral and Enteral Nutrition. 2016; 40(2): 159 -211.
Addressed Criteria • • Nutrition assessment Initiation of enteral nutrition (EN) Dosing of EN Monitoring tolerance and adequacy of EN Selection of appropriate enteral formulation Adjunctive therapy When to use parenteral nutrition (PN) When to maximize efficacy of PN
Addressed Criteria (Cont. ) • • • Pulmonary failure Renal failure Hepatic failure Acute pancreatitis Surgical subsets: trauma, traumatic brain injury, open abdomen, burns Sepsis Postoperative major surgery (SICU admission expected) Chronically critically ill Obesity in critical illness Nutrition therapy end-of-life situations
Guidelines Recommendations are Based on the Data Derived From: • • • Randomized controlled trials Nonrandomized cohort trials Prospective observational studies Retrospective case series Quality of evidence ranges from very low-lowmoderate-to high
Current Guidelines Limitations • Data was obtained through December 31, 2013 • Other landmark studies published after this date were not included in this guideline
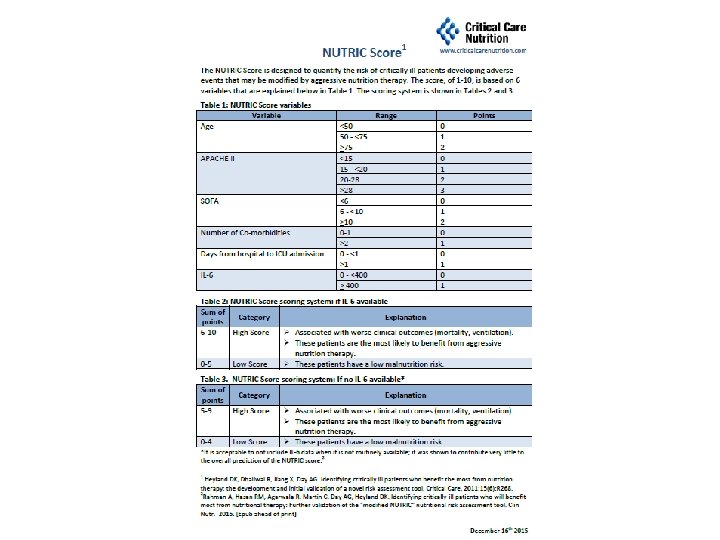
Nutrition Assessment: Determine Nutrition Risk for All Patients Admitted to the ICU Baseline nutrition status Disease severity Use NRS 2002 or NUTRIC score. Nutrition risk
Nutritional Risk Screening (NRS 2002)
Nutrition Assessment (Cont. ) NRS 2002 NUTRIC • Risk • High risk – NRS 2002 >3 • High risk – NRS 2002 >/=5 – NUTRIC >/=5
Nutrition Assessment: Energy Requirement Method Indirect calorimetry (IC) (Quality of Evidence: Very Low) Simplistic formula: 25 -30 kcal/kg/day Comments Accuracy affected by air leaks, chest tubes, supplemental oxygen, ventilator settings, CRRT, anesthesia, PT, excessive movement. Use dry or usual body weight for normal weight patients; use IBW for obese patients. Predictive equations Less accurate in obese and underweight patients. Reevaluate energy expenditure more than once per week. Account for dextrose-containing fluids and lipid-based medications.
Nutrition Assessment: Protein Requirements • Protein requirements are higher than energy requirements • Provision of protein is more closely correlated with positive patient outcomes than provision of total energy • Not easily met by routine enteral formulations and patients might benefit from protein supplementation • Weight-based recommendation: 1. 2 -2 g/kg/day (actual body weight) (Quality of Evidence: Very Low) – May be higher in burn/trauma/CRRT patients
Nutrition Assessment: Protein Requirements (Cont. ) Albumin Pre-albumin • T ½ = 21 days • Indicates body protein stores • Good indicator of initial nutritional status • Not a good indicator of early protein malnutrition • T ½ = 2 -3 days • Responds more rapidly to nutrition support • Reflects improvements in nutrition intake and status • Renally eliminated falsely elevated in ARF/CRF Do not use serum protein markers to determine adequacy of protein provision.
Enteral Nutrition
Enteral Nutrition • Supports structural integrity of the gut • If structural integrity compromised – Increased bacterial challenge – Risk of systemic infections – Risk of multiple-organ dysfunction • Initiate within 24 -48 hours (Quality of Evidence: Very Low) • Use EN over PN (Quality of Evidence: Low to Very Low) • Bowel sounds and evidence of bowel function are not required for initiation of EN – Safety data came from studies involving critically ill surgical patients • Initiate EN in the stomach, unless – High risk for aspiration – Not able to tolerate gastric infusion • Hold EN in hemodynamically unstable patients – Use caution in patients undergoing withdrawal of vasopressor support
Figure 1. Early enteral nutrition (EN) vs delayed EN, mortality. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Figure 2. Early enteral nutrition (EN) vs delayed EN, infectious complications. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Figure 3. Enteral nutrition (EN) vs parenteral nutrition (PN), infectious complications. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Dosing/Amount of EN • Patients with low nutrition risk and low disease severity (NRS 2002 </=3 or NUTRIC </=5) do not require nutrition therapy during the first week in the ICU – Reassess daily • Patients with ARDS/acute lung injury and are on mechanical ventilation, should receive either trophic (10 -20 kcal/hr or 10 -20 ml/hr or up to 500 kcal/day) or full EN during the first week in the ICU • Patients at high nutrition risk (NRS 2002 >/=5 or NUTRIC >/=5) should be advanced to goal over 24 -48 hours
Monitoring Tolerance and Adequacy of EN: Daily Tolerance Intolerance • Normal physical examination • Passage of flatus and stool • Absence of pain or abdominal distension • Normal radiologic evaluation • • Vomiting Diarrhea Reduced passage of flatus and stool Abdominal distension Complaints of discomfort Abnormal abdominal radiographs High NG output High gastric residual volume (GRV) >500 ml/24 hrs – – – GRV does not correlate with incidences of PNA, regurgitation, or aspiration Not recommended to do routine GRV measurements in patients on EN Not recommended to hold EN for GRV <500 ml/24 hrs in the absence of other signs of intolerance (Quality of Evidence: Very Low) • GRV 200 -500 ml/24 hrs, need to implement measures to reduce risk of aspiration
Who is at Risk for Aspiration? • • • Inability to protect the airway Presence of nasoenteric enteral access device Mechanical ventilation Age >70 years Reduced level of consciousness Poor oral care Inadequate nurse: patient ratio Supine position Neurologic deficit Gastroesophageal reflux Transport out of the ICU Bolus intermittent EN infusion
If at Risk for Aspiration • Deliver EN to the small bowel instead of stomach OR • Use prokinetic agents IV or PO (Quality of Evidence: Low) – Metoclopramide 10 mg QID for normal renal function – Erythromycin 3 -7 mg/kg/day • Intubated patients receiving EN – head of bed to be elevated 30°-45° and use chlorhexidine mouthwash BID • Reduce level of sedation/analgesia when possible • Minimize transport out of the ICU for diagnostic tests and procedures
Figure 7. Motility agents vs placebo, outcome lower gastric residual volume. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Selection of Enteral Formulation • Use standard polymeric formula • Avoid routine use of specialty or diseasespecific formulas – Exception: immune-modulating formula in post-op patient in SICU setting (Quality of Evidence: Very Low) • Rationale for use of pulmonary formulas (high fat: carbohydrate ratio) “has shown to be erroneous”
Adjunctive Therapy Fermentable soluble fiber additive -To be considered in all hemodynamically stable ICU patients on standard EN. -10 -20 g/24 hrs of a fermentable soluble fiber in patients with diarrhea. Probiotics Recommendation cannot be made at this time with regards to routine use across all types of ICU patients. (Quality of Evidence: Very Low) • Probiotics MOA: competitive inhibition of pathogenic bacterial growth and epithelial attachment of invasive pathogens, elimination of pathogenic toxins, enhancement of intestinal epithelial barrier, favorable modulation of host inflammatory response. • Documented safety and outcome benefit in selective patient populations: liver transplantation, trauma, pancreatectomy. Antioxidant vitamins and -To be provided in patients with burns, trauma, and on trace minerals mechanical ventilation. (Quality of Evidence: Very Low)
Parenteral Nutrition
When to Use PN Patient at low nutritional risk (NRS 2002 </=3 or NUTRIC score </=5) If early EN not feasible, recommend to withhold PN over the first 7 days following ICU admission, unless PN dependent. (Quality of Evidence: Very Low) Patient at high nutritional risk (NRS 2002 >/=5 or NUTRIC score >/=5) or severely malnourished If early EN not feasible, recommend to initiate PN as soon as possible following ICU admission. In patients at low or high nutrition risk who are on EN but unable to meet >60% of energy and protein requirements, recommend use of supplemental PN after 7 -10 days. Once patient is able to receive >60% of their goal via EN, recommend to d/c PN.
Risks Associated with PN Hyperglycemia Electrolyte imbalances Oxidative stress Immune suppression Infections
Risk Factors for Refeeding Syndrome Alcoholism Weight loss Low BMI Prolonged NPO Advance to goal over 3 -4 days.
How to Maximize Efficacy of PN in High Risk/Severely Malnourished Patients • During first week (Quality of Evidence: Low) – Hypocaloric PN: </=20 kcal/kg/day or 80% of estimated energy – Adequate protein: >/= 1. 2 g/kg/day • Once patient is stable, advance to 100% of estimated goal • Withhold or limit soy-based IV fat emulsion during the first week of PN to maximum of 100 g/wk (divided in 2 doses/wk) if there is concern for essential fatty acid deficiency (Quality of Evidence: Very Low) • Target BG 140 or 150 -180 mg/d. L
EN/PN Recommendations for Organ Dysfunctions
Organ Dysfunctions Pulmonary failure -Do not recommend use of high-fat/low CHO formulations to reduce CO 2 production in patients with acute respiratory failure. (Quality of Evidence: Very Low) -Avoid rapid infusion of IVFE. -Use fluid-restricted energy-dense EN formulations. -Close serum phosphate monitoring and appropriate replacement. Renal failure (AKI/ARF) -Use standard enteral formulation. -Energy provision: 25 -30 kcal/kg/day. -Protein provision: 1. 2 -2 g/kg/day (actual body weight); up to 2. 5 g/kg/day if on HD or CRRT (Quality of Evidence: Very Low). -Consider specialty formulations (low in phosphate and potassium) with appropriate electrolyte profile.
Organ Dysfunctions (Cont. ) Hepatic failure (cirrhosis) -Use dry weight or usual weight to determine energy and protein requirements. -Avoid restricting protein. -EN is preferred route. -Use standard EN formulation (there is no evidence of benefit of branched-chain amino acids formulations on coma grade in patients with encephalopathy). Acute pancreatitis Mild pancreatitis: specialized nutrition is not recommended; advance to oral diet as tolerated. If not able to advance to oral diet within 7 days, then consider specialized nutrition. (Quality of Evidence: Very Low) Moderate to severe pancreatitis: start EN (preferred over PN) at a low-volume rate within 24 -48 hrs of admission and advance to goal as tolerated. (Quality of Evidence: Very Low) • Consider use of probiotics with severe pancreatitis in patients on EN. (Quality of Evidence: Low) • If EN not feasible, use PN after 1 week from the onset of symptoms.
Figure 12. Parenteral nutrition (PN) vs enteral nutrition (EN) in severe acute pancreatitis, mortality. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Figure 13. Parenteral nutrition (PN) vs enteral nutrition (EN) in severe acute pancreatitis, infections. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Recommendations for Surgical Subsets
Surgical Subsets Trauma -Early EN within 24 -48 hrs of injury with high protein. (Quality of Evidence: Very Low) -Energy requirements: 20 -35 kcal/kg/day. Less energy in early phase and more energy in rehabilitation phase. -Protein requirements: 1. 2 -2 g/kg/day, target higher end of range. -In severe trauma: consider immune-modulating formulations. (Quality of Evidence: Very Low) Traumatic brain injury -Early EN within 24 -48 hrs of injury. (Quality of Evidence: Very Low) -Energy requirements: vary depending on use of paralytics and/or coma-inducing agents. -Protein requirements: 1. 5 -2. 5 g/kg/day. -Suggest arginine-containing immune-modulating formulation or EPA/DHA supplement with EN formulation.
Surgical Subsets Open abdomen -Early EN within 24 -48 hrs post-injury in the absence of a bowel injury. -Determine energy needs similar to other patients in surgical or trauma ICU. -Protein requirements: suggest additional 1530 g of protein/liter of exudate lost. Burns -EN should be provided if GI tract is functional and be initiated within 4 -6 hrs of injury. -PN reserved if EN not feasible or not tolerated. -Suggest IC to assess energy needs, repeat weekly. -Protein requirements: 1. 5 -2 g/kg/day.
Sepsis • EN to be initiated within 24 -48 hrs of diagnosis of severe sepsis/septic shock as soon as resuscitation is complete and patient is hemodynamically stable – Hemodynamically stable: adequate perfusion pressure, stable doses of vasoactive drugs, stabilized or decreasing levels of lactate and metabolic acidosis, MAP >/=60 mm. Hg • Regardless of patients’ nutrition risk, do not recommend use of exclusive PN or supplemental PN in conjunction with EN early in the acute phase of severe sepsis/septic shock (Quality of Evidence: Very Low) • Energy requirements: up to 500 kcal/day during first 24 -48 hrs of initial phase, then advance to >80% of goal energy (25 kcal/kg/day) over the first week • Protein requirements: 1. 2 -2 g/kg/day • Cannot make recommendation regarding selenium, zinc, and antioxidant supplementation due to conflicting results
Postoperative Major Surgery (SICU Admission Expected) • Provide EN within 24 hrs postoperatively – Exceptions: GI obstruction, bowel discontinuity, increased risk of bowel ischemia, ongoing peritonitis • Recommend immune-modulating formulas for post-op patients on EN • EN is suggested in patients with prolonged ileus, intestinal anastomosis, open abdomen, on vasopressors (Quality of Evidence: Low to Very Low) • In patients s/p major upper GI surgery and EN not feasible, initiate PN only if duration of therapy is anticipated >/=7 days and be initiated post-op day 5 -7 – Exception: in patients at high nutrition risk may initiate it earlier • Post-op diet to be advanced to solid food and not clear liquids
Chronically Critically Ill • Persistent organ dysfunction requiring ICU LOS >21 days • “Persistent inflammation, immunosuppression, and catabolism syndrome” • Recommend – Aggressive high-protein EN therapy – Glycemic control
Obesity in Critical Illness • EN within 24 -48 hrs of ICU admission • Determine actual, usual, and ideal weight – Adjusted body weight is not recommended • Calculate BMI, identify class of obesity, measure waist circumference (if possible) • Evaluate biomarkers of metabolic syndrome: BG, TG, cholesterol • Assess preexisting conditions • In patients with history of bariatric surgery, supplement thiamine prior to initiating dextrose-containing IV fluids or nutrition therapy – Evaluate for micronutrient and trace minerals deficiency • Implement high-protein hypocaloric feeding
Obesity in Critical Illness (Cont. ) BMI 30 -50 >50 Weight-based energy requirements 11 -14 kcal/kg actual body weight/day 22 -25 kcal/kg ideal body weight/day -Energy goal should not exceed 65 -70% of goal as measured by IC. -Weight-based equations represent 65 -70% of measured energy expenditure.
Obesity in Critical Illness (Cont. ) BMI 30 -40 >/=40 Protein requirements 2 g/kg ideal body weight/day Up to 2. 5 g/kg ideal body weight/day
Nutrition and Hydration Therapy in End-of-Life Situations • Not obligatory • Cultural, ethnic, religious, or individual patient issues may necessitate delivery of nutrition and hydration • Should be communicated to patients, family members, or decision makers • Respect for dignity and patient autonomy
Table 2. Bundle Statements. Stephen A. Mc. Clave et al. JPEN J Parenter Enteral Nutr 2016; 40: 159 -211 Copyright © by The American Society for Parenteral and Enteral Nutrition
Question #1 • You do NOT use serum protein markers to determine adequacy or protein provision. A. True B. False
Question #2 • When should admitted patients be required for initial nutrition screening? A. B. C. D. No later than 24 hours Within 48 hours of admission At admission None of the above
References • Bongard F. S. , Sue D. Y. , Vintch J. E. Current Diagnosis & Treatment Critical Care, 3 rd edition, Mc. Graw Hill 2008, Ch. 6. • Gastroenterology and Nutrition. ACCP PSAP, 6 th edition, book 9, pp. 119 -128. • Kondrup J. , et al. Nutritional Risk Screening (NRS 2002): a New Method Based on an Analysis of Controlled Clinical Trials. Clinical Nutrition 2003; 22(3): 321 -336. • Mc. Clave S. A. , et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A. S. P. E. N. ). Journal of Parenteral and Enteral Nutrition 2016; 40(2): 159 -211. 57