Anemia is common in critically ill patients About

• Anemia is common in critically ill patients • About 90% of patients admitted to the ICU have hemoglobin levels below normal • 50~85% of all ICU patients received at least one RBC unit • Many factors can be involved in development of anemia and needs to requirement of RBC transfusion

• The benefit of blood transfusion is controversial • The consequence of Anemia on morbidity and mortality in the critically ill patient is poorly defined • We reviewed articles and summarize the anemia and blood transfusion practice in critically ill patients

Time course of Hb in ICU patients • Many studies were reported • Hb concentrations can fall in ICU patients without active bleeding • At first 3 day admitted in ICU, the amount of Hb decrease is maximum • The amount of RBC transfusion and down of Hb concentration related to LOS of ICU

Mean Hemoglobin concentrations over time

Percentage of Pts receiving transfusion over time

Mean number of RBC units transfused over time

Transfusion in critically ill patients • The expected benefit of transfusion is an immediate improvement in oxygen delivery which, in turn, prevents cellular injury • Transfusion is not always improved clinical outcomes in critically ill patients • RBC transfusion is not risk free

Nosocomial infections and Transfusion

Transfusion and mortality in ICU Pts

Transfusion and mortality in ICU Pts

Pathogenesis of Anemia in ICU Pts Blood loss • Repeated diagnostic blood samplings play a major role in develop of anemia • Occult and overt bleeding are potentially significant

Pathogenesis Regulation of Erythropoietin Expression • In severe hypoxia Erythropoietin production can increase up to 1000 -fold • Induction of erythropoietin expression increases oxygen availability and tissue oxygen tension • In critical illness, the erythropoietin response to low hemoglobin concentration is blunted • Proinflammatory cytokines play a major role in blunting erythropoietin response to anemia

Pathogenesis Iron metabolism • Low serum iron, Total iron binding capacity, iron/total iron binding capacity ratio and normal or more usually, an elevated serum ferritin level • Proinflammatory cytokines play a major role in alterations in iron metabolism

Pathogenesis Nutritional deficiencies • Low concentrations of vitamin B 12, folic acid, iron might contribute to ineffective erythropoiesis • Nutritional deficiency may play a small but potentially correctable role in anemia un critical illness

Pathogenesis Red blood cell life span • RBC, after a life span of 120 days in the circulation, are removed by macrophages by phagocytosis • Proinflammatory cytokines TNF-a, IL-1 decrease erythrocyte survival time

Pathogenesis Functional and structural alterations in RBCs • Erythrocytes can reversibly alter their biconcave, discoid shape, enabling the cells to pass through capillaries • Decreased deformiabilities, microcirculatory function can be decreased, which can contribute to organ dysfunction
 Acute blood loss")
Cause of Anemia in Critically ill patients • Blood loss 1) Acute blood loss ; perioperative blood loss 2) Non surgical blood loss ; GI bleeding ; repeated blood sampling
 Intrinsic cause (RBC itself) : Acute infection,")
• Increased destruction of RBC 1) Intrinsic cause (RBC itself) : Acute infection, sickle anemia etc 2) Extrinsic cause ; IABP, CPB, Mechanical valve, Rapid infusion of hypotonic solution, splenomegaly etc
 depressed RBC poduction in BM 2) blunted")
• Decreased production of RBC 1) depressed RBC poduction in BM 2) blunted EPO response ; proinflammatory cytokines 3) hypoferremia and abnormal iron metabolism 4) Nutritional deficiency

Strategies to prevent anemia in ICU • Prevention and arrest of bleeding • Optimization of oxygen delivery • Minimization of oxygen consumption • Optimization of erythropoiesis • Tolerance of anemia • Minimization of iatrogenic blood loss

Prevention and arrest of bleeding • Close surveillance for blood loss • Rapid diagnosis and control of hemorrhage • Permissive moderate hypotension • Prophylaxis of upper GI bleeding • Anticoagulation management • Hemostasis and anticoagulation management

Optimization of oxygen delivery • Asses tissue perfusion and tissue oxygenation • Judicious fluid replacement • Individualized volume and fluid management • Early optimization of tissue oxygenation and perfusion

Minimization of oxygen consumption • Adequate analgesia, sedation • Consider muscle relaxants • Consider mechanical ventilation • Consider moderate or mild hypothermia

Minimization of iatrogenic blood loss • Small volume phlebotomy tubes • Point of Care Bedside Microanalysis • Red Blood cell salvage techniques • Use guidelines for Lab testing • Non-invasive and continuous testing • Education
")
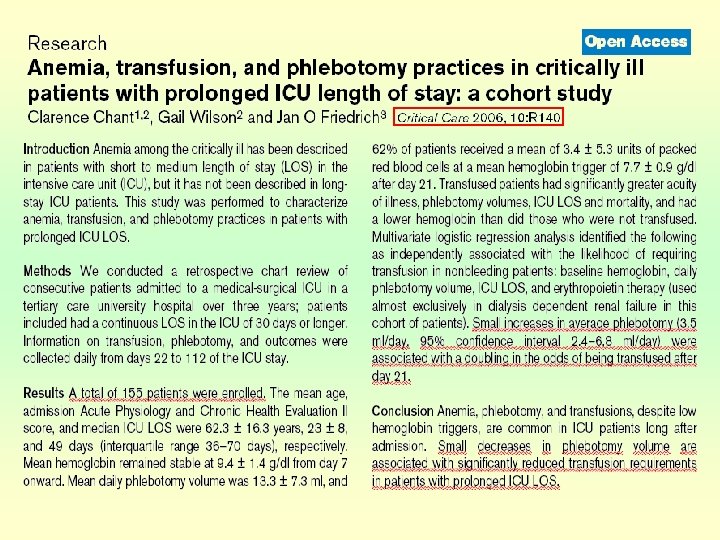
Blood loss from repeated blood sampling • United states (1986, N Engl J Med) ; 377 ml/day in cardiothoracic ICU ; 240 ml/day in surgical ICU • Great Britain (1990, Anaesthesia) ; 85. 3 ml/day and then 66. 1 ml/day • German ICU (1999, Crit Care Med) ; 41. 1 ml/day ; most significant independent predictor

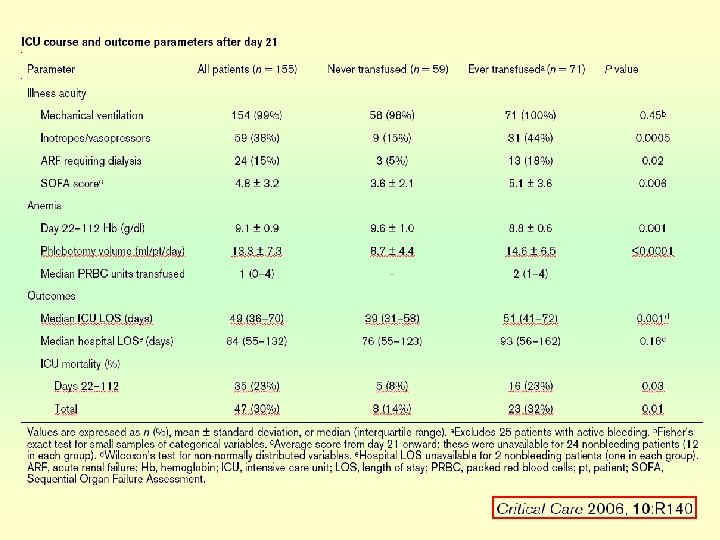
Relationships between phlebotomy and transfusion

Optimization of erythropoiesis • Early EPO therapy • Iron replacement • Nutritional support

Cumulative Units of Red Blood cells Transfused

Mean Hemoglobin by treatment by r. Hu. EPO

Tolerance of anemia • Many recent studies reported • Restrictive blood transfusion • Transfusion trigger

Outcomes in 257 patients with ischemic heart disease

Survival curves in restrictive and liberal groups

Survival curves in restrictive and liberal groups

Summary • Anemia is common problems in ICU • Various factors contribute to development of anemia • Large number of critically ill patients received transfusion • Many recent studies reported that prevention of anemia and reduction in blood transfusion may improve clinical outcomes of ICU patients

• Many studies reported that blood loss by doctor, iatrogenic blood loss play a major role in development of anemia • Reduced iatrogenic blood loss may contribute to decreased RBC transfusion and improve the prognosis of critically ill patients

In conclusion • More conservative approach to RBC transfusion is warranted • Strategies to minimize loss of blood and increase the production of RBCs are important in the management of critically ill patients

Thank you for your attention
- Slides: 44