Basics of clinical nutrition in critically ill patients

Basics of clinical nutrition in critically ill patients Jacek Szopinski, Marlena Jakubczyk Department of Anaesthesiology and Intensive Care , Nutrition Support Team

sedation nutrition ventilation …. renal suport katecholamines pain control

CLINICAL NUTRITION Supply of energy, proteins, electrolytes, trace elements and vitamins in the form of intravenous fluids or formulae to the patients who are not able to eat normally due to the main disease or/and its complications

Inflammation and organ failure in the ICU Inflammatory balance ANTI PRO SIRS TNF , IL-1 , IL-6, IL-12, IFN , IL-3 Tissue inflammation, Early organ failure and death days weeks IL-10, IL-4, IL 1 ra, Monocyte HLA-DR suppression Immunosuppression CARS Insult (trauma, sepsis) 2 nd Infections Delayed MOF and death Griffiths, R. “Specialized nutrition support in the critically ill: For whom and when? Clinical Nutrition: Early Intervention; Nestle Nutrition Workshop Series

Survival in and from ICU �ICU is about preventing death from organ failure �Patients die early from single organ failure ◦ Due to primary pathology/ insult/ infection (brain, or heart, or liver or lung) �Patients failure die later from multi-organ ◦ Due to secondary infections (combined organ failure (e. g. lung, liver, and kidney)

Why feed the critically ill? � Provide nutritional substrates to meet protein and energy requirements � Help protect vital organs and reduce break down of skeletal muscle � To provide nutrients needed for repair and healing of wounds and injuries � To maintain gut barrier function � To modulate stress response and improve outcome
")
GALT (Gut Associated Lymphoid Tissue)



WHEN ?

• Pre-existing severe malnutrition • Oral intake matches < 50% of the energy and nitrogen needs • Expected delay before recovery of eating ≥ 3 days after the patient has been stabilised within 48 hrs

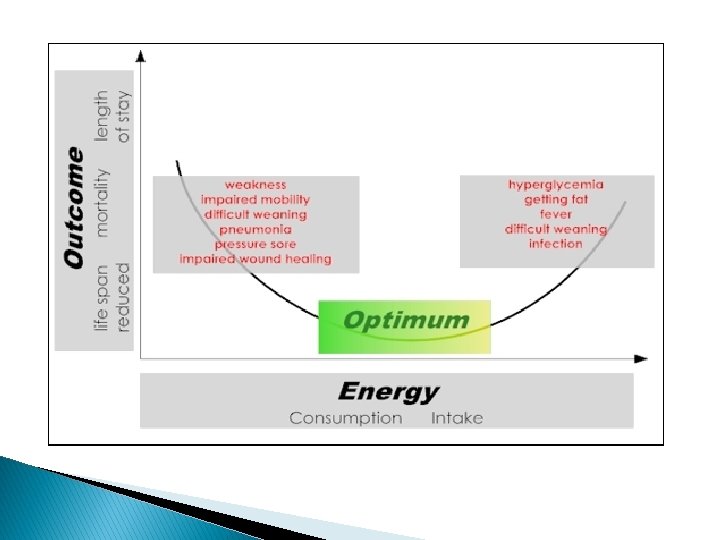
HOW MUCH ?

Malnutrition…

And malnutrition …
 � � � This is energy needed to maintain the")
Resting Energy Expenditure (REE) � � � This is energy needed to maintain the heart, lung, work for synthesis of new chemical bonds & for maintaining electrochemical gradient in cells. This requires 22 kcal/kg/day averagely. Can be measured by calorimetry or using Harris- Benedict equation

Harris – Benedict equation Men BMR = 88. 362 + (13. 397 x weight in kg) + (4. 799 x height in cm) - (5. 677 x age in years) Women BMR = 447. 593 + (9. 247 x weight in kg) + (3. 098 x height in cm) - (4. 330 x age in years)

Energy reqiurements � Acute phase and initial phase of critical ilness 20 – 25 kcal / kg. BW � Anabolic recovery phase � 25 – 30 kcal / kg. BW begin with 30 % of the final energy administration and slowly (days) gain the target

Indirect calorimetry Using indirect calorimetry we can measure: � Oxygen consumption - VO 2 � Carbon dioxide production - VCO 2 � The energy equivalent of VO 2 and VCO 2 is dependent on quantities of carbohydrate (C), protein (P) and fat (F) oxidized. Protein oxidation (g) is calculated from nitrogen lost in urine and subsequently the following formula can be used for calculation of energy expenditure: � EE (MJ) = 16. 20 VO 2 + 5. 00 VCO 2 - 0. 95 P � � Energy expenditure can be also calculated either from oxygen consumption or carbon dioxide production.

Suggested feeding: ICU � When to start? CALORIE COUNT!!! ◦ The sooner, the better � How much? ◦ Patients adapted to undernutrition or with a circulatory instability may benefit with a slow start, lower target with stepwise increase � What to give? ◦ Balanced nutrition ◦ Enteral route, parenteral as supplementation Jan Wernermann, “ICU Cookbook”. Franc-, 2003

HOW ?

Nutrition route ENTERAL route always preferable unless contraindications: • mechanical ileus, • severe shock (non-stabilized), • bowel ischemia IF the enteral route NOT POSSIBLE or at least 60% of daily energy intake can not be acheived -> MIXED ENTERAL AND PARENTERAL NUTRITION PARENTERAL route alone
 � Nasojejunal")
Enteral feeding “If the gut works – use it” � Nasogastric (NG) � Nasojejunal (NJ) � Percutaneous Endoscopic Gastrostomy (PEG) � Percutaneous Endoscopic Jejunostomy (PEJ) � Radiologically Inserted Gastrostomy (RIG) � Surgical Gastrostomy � Surgical Jejunostomy (JEJ)

Methods of enteral feeding � Nasogastric tube � Nasoenteral tube � Tube enterostomy � Percuteneous endoscopic jejunostomy (PEG) � Fine catheter needle jejunostomy

Nasoenteric tube

Microjejunostomy

PEG or G-tube

EN � Always check gastric emptying ! �Gastric residuals < 200 ml – ok. �Gastric residuals > 200 ml + prokinetics + elevation + be careful !!!

Central vein access


Central vein access The end of the catheter lower 1/3 vena cava upper 1/3 right atrium X-ray !

The completness rule The administered nutrition formula should have ALL macronutrients (proteins, lipids and carbohydrates) and micronutrients (vitamins, trace elements, electrolytes) and water in the amounts available to compensate patient’s needs

Enteral formulae Protein sources for the whole protein formulae are mostly milk proteins such as casein, often together with soy proteins. In peptidebased formulae hydrolysates of soy, lactalbumin, gelatine and/or whey are used. Amino acid-based formulae contain free amino acids, and accordingly do not contain glutamine, because this amino acid is not stable in its free state. Fat sources in standard whole protein formulae are predominantly mixtures of oils that are high in polyunsaturated ω-6 fatty acids, such as sunflower, soy, safflower and corn oils. Recently, with increasing awareness of the positive effects of the ω-3 fatty acids, canola oil has been added to many formulae, and sometimes fish oils are added. Medium chain triglycerides (MCT) derived from coconut oil form part of several formulae. Peptide-based and elemental preparations often contain dominant amounts of MCTs, on the basis that they do not require bile salts or pancreatic lipase prior to absorption, and that they bypass the lymphatic system with direct uptake into the portal circulation. Self-evidently the MCTs do not contain any essential fatty acids, and a minimum of 5% polyunsaturated fatty acids is added to any such mixture in order to ensure that the formula is nutritionally complete.

Carbohydrate sources are predominantly partial enzymatic hydrolysates of corn starch (maltodextrins with at least 10 glucose molecules). Some formulae, especially those intended for oral use, may contain small amounts of sucrose as this increases palatability. Some whole protein formulae may also contain starch. Minerals, vitamins and trace elements are added, usually to meet 100% of each RDA in the volume of the formula required to yield 1500 kcal.

EN formulae generally do not contain lactose, cholesterol, purines, or gluten This is achieved by careful choice of the base materials rather than through technical elimination processes. Cholesterol, for example, is avoided by the selection of plant oils as the predominant lipid sources. Purines are absent from the principal macro-ingredients (such as milk and soy). Gluten content is minimised by the choice of corn-derived carbohydrates. The protein component of most enteral products is added in highly concentrated powder form, usually with a protein fraction of about 85%; this helps to ensure that only negligible amounts of lactose remain despite the use of milk. Enteral formulae are therefore safe for patients with primary or secondary lactose intolerance, coeliac disease, and appropriate for use in those with gout or hypercholesterolaemia. Despite their use of manipulated products, enteral formulae are still based on natural components mainly using common high quality staples. Emphasising their artificiality is no more logical than in respect of regular supermarket foods (such as milk desserts), and may be counterproductive when encouraging their use by patients.

EN Standard formula standard energy 0. 9 – 1. 2 kcal / ml low energy < 0. 9 high energy > 1. 2
 - contain intact proteins, and usually include lipids in")
1. Whole protein formulae (polymeric) - contain intact proteins, and usually include lipids in the form of long chain triglycerides (LCTs), and carbohydrates predominantly as maltodextrins; - require relatively normal gastrointestinal function for digestion and absorption, but can be used successfully in up to 95% of patients on artificial enteral nutrition; - nutrients are not hydrolysed - osmolality reasonably close to the physiological level (about 200 to 350 mosmol/kg). 2. Peptide – based formulae (oligomeric) - partially "pre-digested" and are thus more easily absorbed than whole protein formulae. - contain nitrogen predominantly in peptide form (chains of 2 -50 amino acids). - lipids are provided at least in part as MCTs, since these also are more readily digested and absorbed. 3. Free amino acid formulae (monomeric) contain single amino acids as the nitrogen source; very few indications for their use, since oligopeptides are generally better absorbed than free amino acids and combine this with lower osmolality.

Indications for monomeric formulae Some forms of congenital metabolic disease, Severe allergy to dietary protein, Nutritional treatment of Crohn's disease

Proteins amino acids always 8 obligatory amino acids: (izo, leu, liz, met, fen, tre, try, wal) + non obligatory amino acids total amount: 12 -16 g/l daily requirement for healthy adults: 0. 75 /kg BW daily requirement for patients: 1. 0 – 1. 5 / kg BW
 usually 50 -70 %")
Carbohydrates Glucose one of 2 main energy sources (4 kcal/g) usually 50 -70 % of energy lowers the level of gluconeogenesis, regulates metabolism of amino acids and lipids Max dose 5 mg/kg/min produced CO 2 RQ (Respiratory Quotient) = _______ used O 2 RQ glucose = 1. 0 RQ lipids = 0. 7 Maintain plasma glucose < 150 mg/dl
 source of energy (1 g = 9 kcal) and")
Lipids soybean fatty acids (LCT) source of energy (1 g = 9 kcal) and obligatory fatty acids (linoleic acid, alpha-linolenic acid) phospholipids – structure of the cell membrane 25 -50 % energy 0. 1 g/kg/h (LCT) or 0. 15 g/ kg/ h (MCT/LCT) stop infusion if hipertrigliceridemia (> 350 mg/dl) able to modify inflammation: MCT, olive oil, fish oil

Vitamins 9 water soluable vitamins + 4 lipid soluable obligatory for metabolism of proteins, lipids and carbohydrates – coenzymes, regulatory functions, antioxidants for free radicals ALL vitamins should be given from the very begining (50% pts shortage of vitamins D, folic acid, E, A, H) administration of some vitamins modifies the need for others (ie. ↑ C -- ↑ B 2 i B 12) Solutions: Soluvit, Cernevit (water sol. ) Vitalipid (lipid sol. )

Electrolytes All electrolytes should be administered to fulfil daily requirements and losts The amino acids solutions contain electrolytes Can be added separately if necessary Na. Cl, KCl, Ca. Cl 2, Ca gluconate, Phosphate Solutions: Glycophos, Addiphos Limitted amout in the All in One bags !!!
")
AIO (”All in One” bags)

AIO 1+ ions: Na + K < 130 mmol/l 2+ ions: Ca + Mg < 8 mmol/l CAN (Critical Aggregation Number a maximal concentration of cations above which the aggregation of lipid particles can occur) 1+ ions + 64 x 2+ ions + 729 x 3+ ions < 600 /l Ca. HPO 4 - unsoluable Ca 3 PO 4 - unsoluable 2+ ions => 60 x more destabilizing effect of a monovalent ions
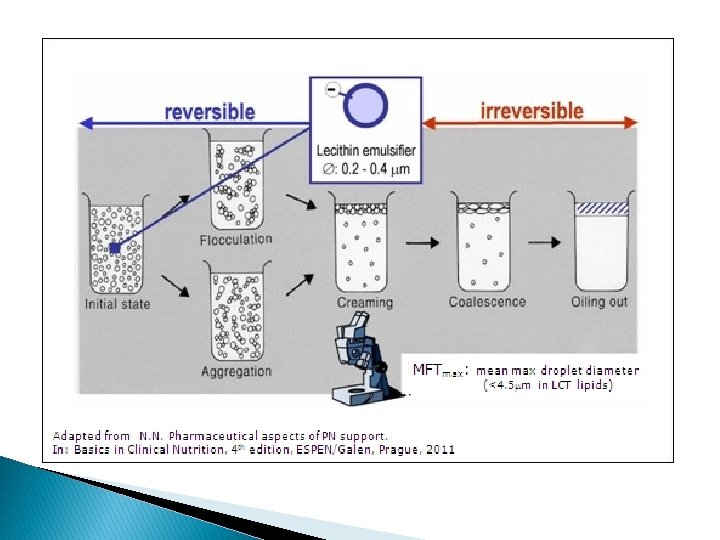

Precipitation of Calcium Hydrogen Phosphate. The sediment is deposited when the product of concentration of Ca 2+ and ions is above 72 mmol 2/L. Many other factors such as p. H and the content of the mixture, the way it was prepared, and storage conditions may affect the solubility of Ca. HPO 4. Currently, the risk of precipitation of Ca. HPO 4 can be eliminated by the use of organic calcium salts such as gluconates and glycerophosphate which do not dissociate in aqueous solutions Inactivation of Vitamins, as They Are Highly Susceptible to Degradation. Parenteral nutrition generally contains vitamins at the minimal concentrations necessary for the body function. Sometimes the clinical state of the patient requires additional supplementation with high doses of some vitamins: vitamin B 1 in severe malnutrition or vitamin C in patients with increased cell catabolism. Inactivation of vitamins may follow many mechanisms: photolysis of vitamin A and B 1, oxidation of vitamin C, reduction of vitamin B 1, or adsorption of vitamin A onto the surface of the container

Immunonutrition Recently - some advantages of specific components for patients’ survival and lowering the number of complications (several trials, some still ongoing) glutamine, arginine, nukcleotydes, ώ- 3 fatty acids GLUTAMINE (Dipeptiven) – elevating the number and activity of limphocytes and the cytotoxic activity of mononuclears; obligatory AA for fast proliferating cells strong indications (grade A) in severe burn and trauma daily dose in critically ill: 0, 3 -0, 6 g/kg OMEGA 3 FATTY ACIDS (Omegaven) – immunosupresive effect (lower cytokine production, lower the expression of Tcell activating receptors) lower inflammatory response (support CARS) max 30 % of daily lipid

brain heart

The Case 26 year old male car accident; no health complaints before the accident Hemorrhagic shock spleen rupture, rupture of the iliac mesentery - laparotomy: spleen removal, sutures of the mesentery open hip fracture - orthopedic stabilisation C 5 fracture - conservative treatment Lung injury with costal fracture 4 -7 left - mechanical ventilation => ICU, pharmacological coma, pain treatment BMI 23 (W: 74 kg H: 178 cm) Albumin (admission) 4, 2 g/dl Is the patient malnourished ?

Answer: NO Should we start and nutritional intervention on the admission day ?

Should we start and nutritional intervention on the admission day ? Answer: No The patient needs hemodynamic stabilisation, fluid and blood resuscitation pain management etc.

Should we start and nutritional intervention on the second day ?

Should we start and nutritional intervention on the second day ? Answer: Yes Polytrauma, inrceased katabolism, potentially long therapy, Inability to eat normally (sedation) and mechanical ventillation

What is the energy requirement ?
 + (4. 799")
BMR = 88. 362 + (13. 397 x weight in kg) + (4. 799 x height in cm) - (5. 677 x age in years) W: 74 kg H: 178 cm Age: 26 === 1786 kcal / d In politrauma REE x 1, 2 = 2144 kcal / d OR 25 -30 kcal / kg -- 1850 - 2200 kcal/ d

Which route to chose: enteral or parenteral ?

Which route to chose: enteral or parenteral ? Answer: Enteral route

Which enteral formula and how ?

Which enteral formula and how ? Answer: Polimeric standard formula Nasogastric tube

What should be checked?

What should be checked? Answer: gastric residuals if > 200 ml - + prokinetics, elevation, reason ?

ESPEN The European Society for Clinical Nutrition and Metabolism www. espen. org
- Slides: 67