SQUINT SURGERY The most common aims of surgery








 procedure is to suture")
















- Slides: 32
SQUINT SURGERY
The most common aims of surgery on the extraocular muscles are to correct misalignment to improve appearance and , if possible , restore BSV. Surgery can also be used to reduce an AHP and to expand or centralize a field of BSV. However, the first step in the management of childhood strabismus involves correction of any significant refractive error and/or amblyopia. Once maximal visual potential is reached in both eyes , any residual deviation can be treated surgically.
the three main types of procedures are : A- weakening , which decreases the pull of a muscle , B- strengthening , which enhances the pull of a muscle and C- procedures that change the direction of muscle action.
WEAKENING PROCEDURES The procedures for weakening the action of a muscle are : - Recession - Disinsertion ( or myectomy ) - Posterior fixation suture.
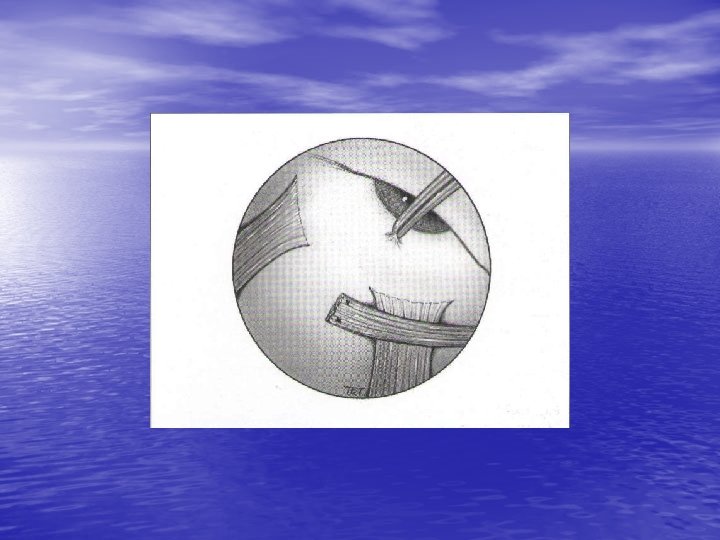
RECESSION Recession slackens a muscle by moving it away from its insertion. It can be performed on any muscle except the superior oblique. 1 - rectus muscle recession - The muscle is exposed and two absorbable sutures are tied through the outer quarters of the tendon. - The tendon is disinserted from the sclera , and the amount of recession is measured and marked on the sclera with calipers.
- The detached end of the muscle is sutured to the sclera at a measured distance behind its original insertion.
2 - inferior oblique disinsertion or recession - The muscle belly is exposed through an inferotemporal fornix incision. - A squint hook is passed behind the posterior border of the muscle , which must be clearly visualized. Care is taken to pick up the muscle without disrupting the Tenon’s capsule and fat posterior to it. - An absorbable suture is passed through the anterior border of the muscle at its insertion and tied. - The muscle is disinserted and the cut end sutured to the sclera 3 mm posterior and temporal to the temporal edge of the inferior rectus insertion.
Disinsertion involves detaching the muscle from its insertion without reattachment. It is most commonly used to weaken an overacting inferior oblique muscle, when the technique is the same as for a recession except that the muscle is not sutured. Very occasionally , the procedure is performed on a severely contracted rectus muscle.
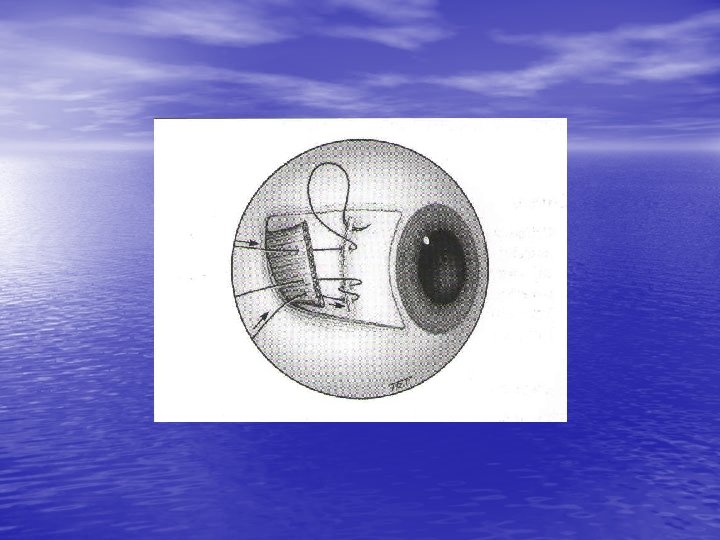
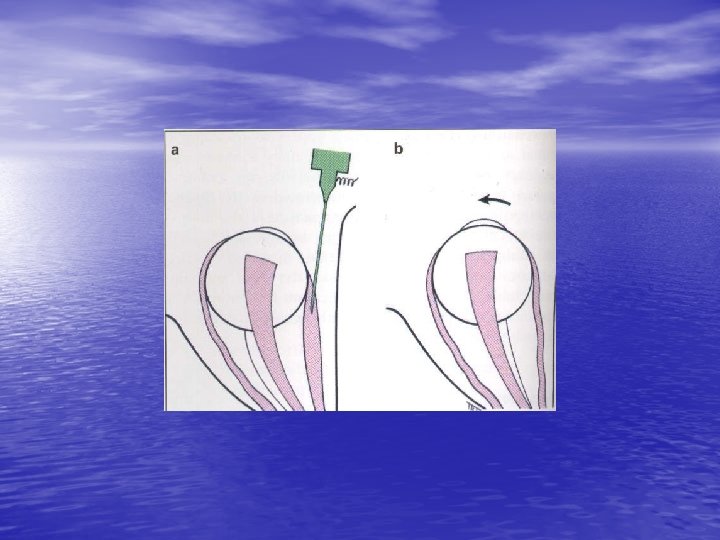
Posterior fixating suture The principle of this ( Faden ) procedure is to suture the muscle belly to the sclera posteriorly so as to decrease the pull of the muscle in its field of action without affecting the eye in the primary position. The Faden procedure may be used on the medial rectus to reduce convergence in a convergence excess esotropia and on the superior rectus to treat DVD. When treating DVD , the superior rectus muscle may also be recessed. The belly of the muscle is then anchored to the sclera with a nonabsorbable suture about 12 mm behind its insertion.
STRENGTHENING PROCEDURES 1 - Resection shortens a muscle to enhance its effective pull. It is suitable only on a rectus muscle and involves the following steps : - The muscle is exposed and two absorbable sutures are tied into the muscle at a measured distance behind its insertion. - The muscle anterior to the sutures is excised and the cut end reattached to the original insertion.
2 - tucking of a muscle or its tendon is usually reserved to enhance the action of the superior oblique muscle in congenital fourth nerve palsy. 3 - advancement of the muscle nearer to the limbus can be used to enhance the action of a previously recessed rectus muscle.
TREATMENT OF PARETIC STRABISMUS Lateral rectus palsy Surgical intervention for a sixth nerve palsy should be considered only when it is clear that spontaneous improvement will not occur. This is usually after at least 3 months have elapsed without improvement , usually at least 6 months in total. Treatment of partial and complete lateral rectus palsies is different
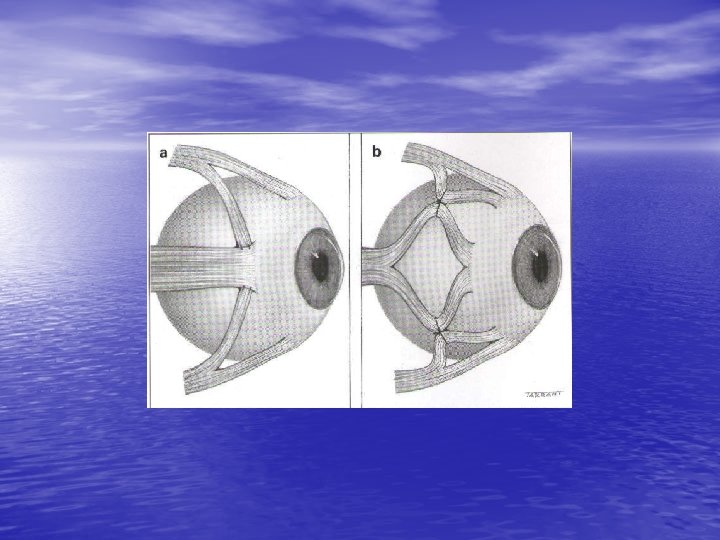
1 - partial palsy is treated by adjustable medial rectus recession and lateral rectus resection of the affected eye , aiming for a small exophoria in the primary position to maximize the field of BSV. 2 - complete palsy is treated by transposition of the superior and inferior recti to positions above and below the affected lateral rectus muscle , coupled with an injection of Botulinum toxin to the medial rectus ( toxin transposition ). NB in an adult , three rectus muscles should not be detached from the globe at the same procedure because of the risk of anterior segment ischaemia.
Superior oblique palsy Surgical intervention should be considered to improve troublesome diplopia or an abnormal head posture. The treatment of unilateral and bilateral palsies is different. General principles are as follows : 1 - unilateral a- congenital cases can usually be treated either by inferior oblique weakening or by superior oblique tucking.
b- acquired - Small hypertropia is treated by ipsilateral inferior oblique weakening. - Moderate to large hypertropia may be treated by ipsilateral inferior oblique weakening which can be combined with , or followed by ipsilateral superior rectus weakening and /or contralateral inferior rectus weakening if required. It should be noted that weakening the inferior oblique and superior rectus of the same eye may result in defective elevation.
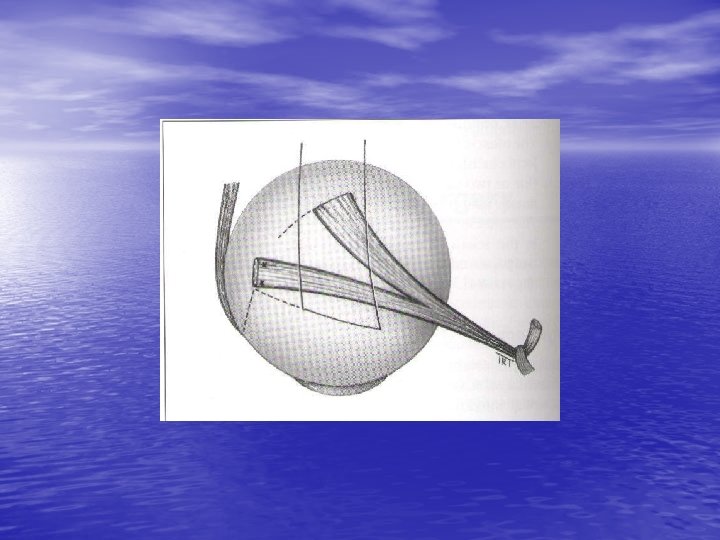
2 - bilateral a- excyclotorsion should first be corrected by the Harada-Ito procedure which involves splitting and anterolateral transposition of the lateral half of the superior oblique tendon. b- any associated vertical deviation can be either corrected at the same procedure or subsequently.
ADJUSTABLE SUTURES Indications The results of strabismus surgery can be improved by the use of adjustable suture techniques on the rectus muscles. These are particularly indicated when a precise outcome is essential and when the results with more conventional procedures are likely to be unpredictable ; for example, acquired vertical deviations associated with thyroid myopathy or following a blowout fracture of the floor of the orbit.
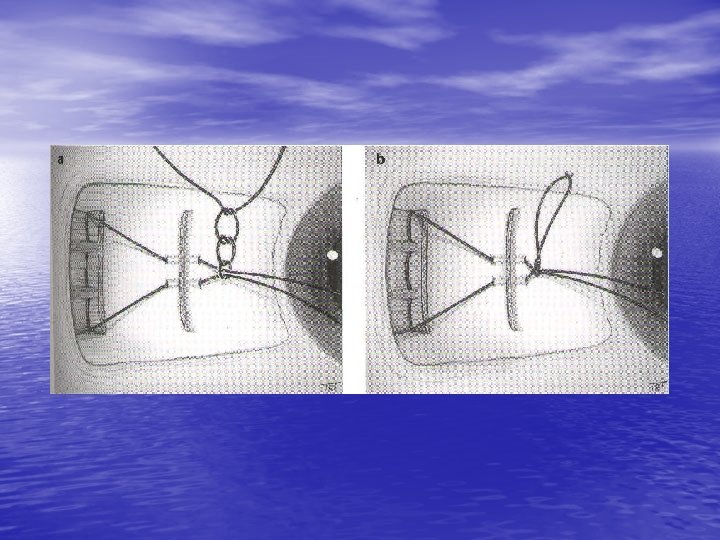
Other indications include sixth nerve palsy , adult exotropia and reoperations in which scarring of the surrounding tissues may make the final outcome unpredictable. The main contraindication is patients who are too young or unwilling to cooperate during postoperative suture adjustment. Initial steps a- the muscle is exposed and a doubleended absorbable suture is tied into the center of the muscle at the insertion.
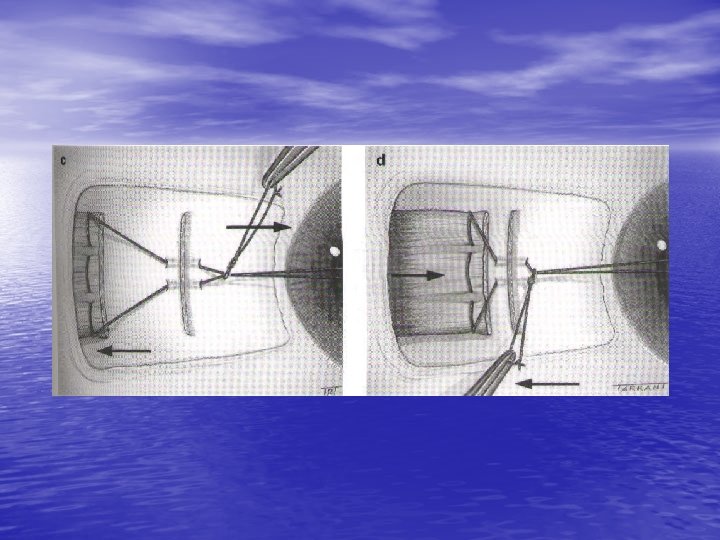
b- each end is then passed through one muscle border and locked. The tendon is disinserted from the sclera ( as for a rectus muscle recession ). c- the two ends of the suture are passed forward through the upper and lower ends of the insertion and then forward through the center of the insertion where they are tied in a bow. d- the conjunctiva is replaced in a recessed position so that it just covers the knot.
Postoperative adjustment This is performed under topical anesthesia , usually a few hours after surgery when the patient is fully awake. a- the accuracy of alignment is assessed. b- if ocular alignment is satisfactory the muscle suture is tied off and its long ends cut short. c- if more recession is required , the bow is undone and the knot slackened so that the muscle can be further recessed.
d- if less recession is required the suture is pulled anteriorly and the bow retied. e- alignment is retested and adjustment repeated as required. A similar technique can be used for rectus muscle resection.
Botulinum toxin chemdenervation Temporary paralysis of an extraocular muscle can be created by an injection of botulinum toxin under topical anesthesia and EMG control. The effect takes several days to develop , is usually maximal at 1 -2 weeks following injection and has generally worn off by 3 months. Side-effects are uncommon, although about 5% of patients may develop some degree of temporary ptosis. The following are the main indications for chemodenervation :
1 - to determine the risk of postoperative diplopia. For example , in an adult with a consecutive left divergent squint and left suppression , straightening the eyes may make suppression less effective , resulting in diplopia. If postoperative diplopia testing by correcting the angle with prisms is negative then the risk of double vision after surgery is very low. If testing is positive then the left lateral rectus muscle can be injected with toxin so that the eyes will either straighten or converge and the risk of diplopia can be assessed over several days while the eyes are straight. If diplopia does occur the patient is able to judge whether it is troublesome.
2 - to assess the potential for BSV In a patient with a constant manifest squint by straightening the eyes temporarily. The deviation can then be corrected surgically if appropriate. A small proportion of patients maintain BSV long-term when the effects of toxin have worn off. 3 - in lateral rectus palsy Botulinum toxin can be injected into the ipsilateral medial rectus to give symptomatic relief during recovery and to see whethere is any lateral rectus action when there is medial rectus contracture. The temporary paralysis of the muscle causes relaxation so that the horizontal
forces on the globe are more balanced , thus allowing assessment of lateral rectus function. 4 - patients with a cosmetically poor deviation who have undergone multiple squint operations can be treated by repeated botulinum toxin injections which may reduce in frequency with time.