Strabismus squint Ahmed Ali Amer Lecturer of ophthalmology
 Ahmed Ali Amer Lecturer of ophthalmology South Valley University")
Strabismus ( squint) Ahmed Ali Amer Lecturer of ophthalmology South Valley University

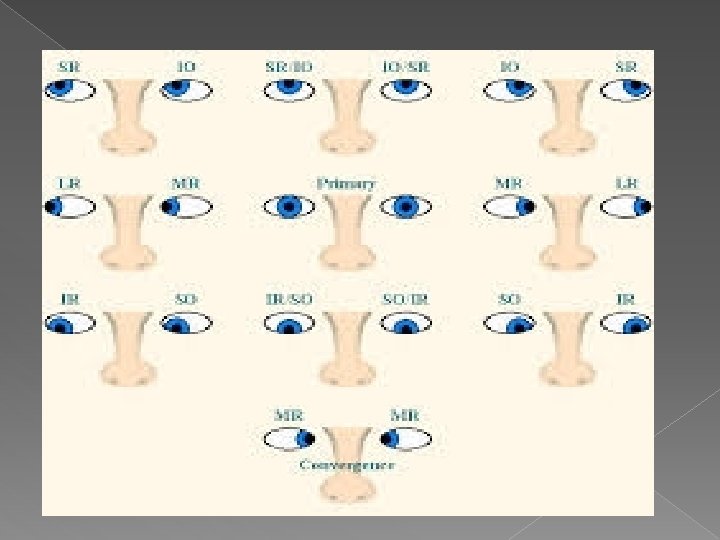
Extraocular muscle � 4 reacti and 2 oblique � Orinign � Insertion � Nerve supply � Action � Testing
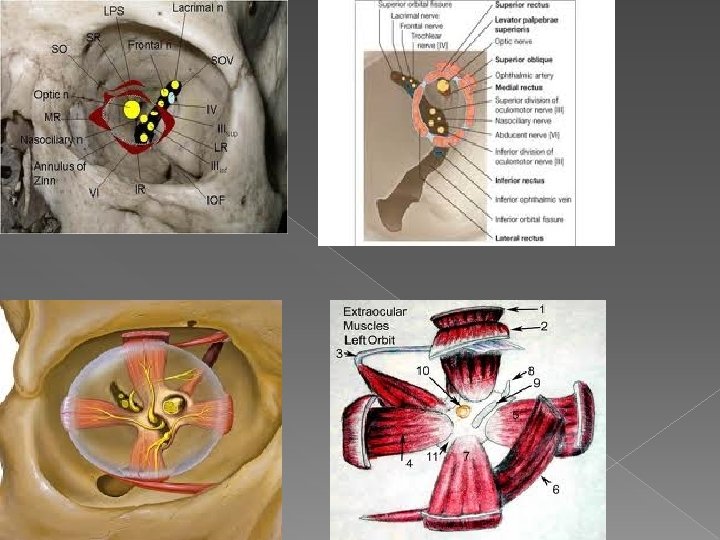
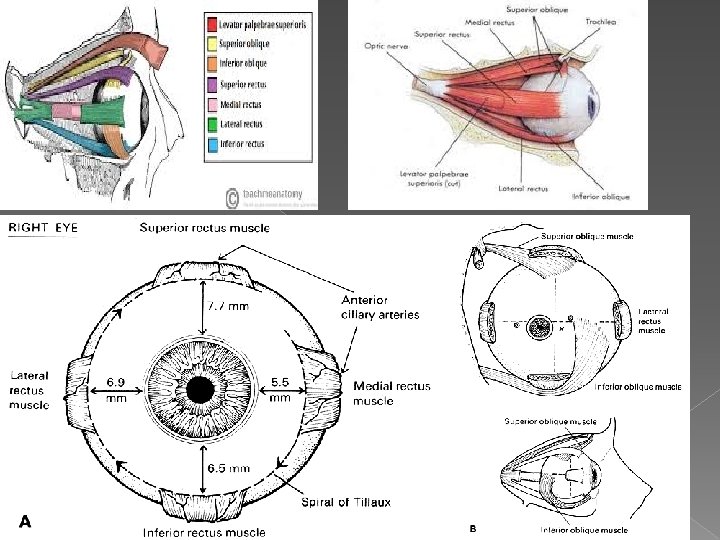

Nerve supply � All by oculomotor nerve except LR and SO

Action Muscle MR Primary Action Adduction Secondary Teritiary action LR Abduction SR Elevation Intorsion adduction IR Depression extorison adduction SO Intorsion Depression abduction IO Extorsion Elevation abduction
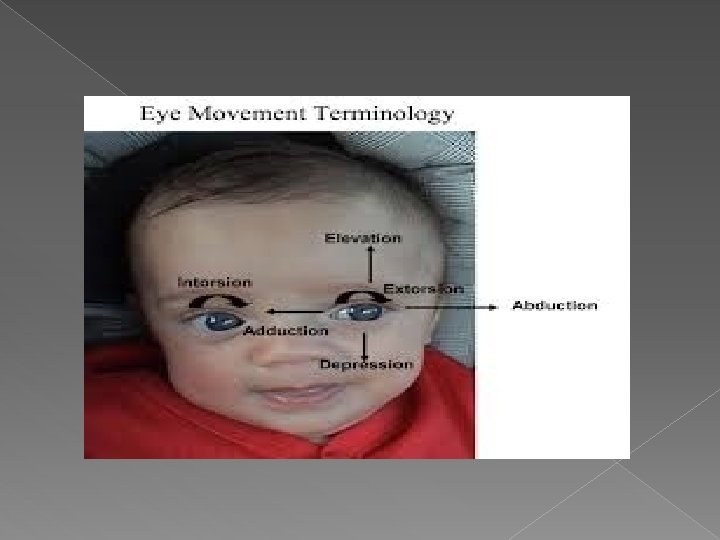

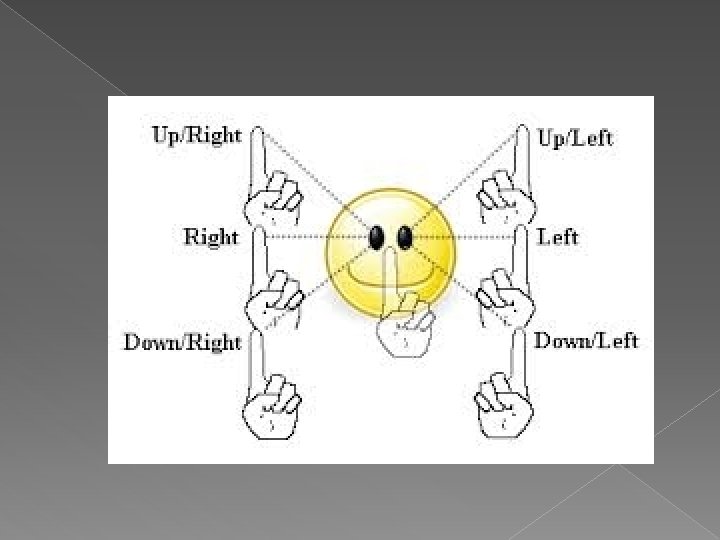
Testing
: in the same")
Agonist and antagonist equal and reciprocal innervation � Direct agonist (synergist): in the same eye with the same action. SR & IO in elevation of Rt eye. � Indirect synergist (Yoke muscles): in the Opposite eye with the same direction of action ( 6 pairs). � Direct antagonist: in the same eye with opposite action : Rt LR and Rt MR. � Indirect antagonist: in the opposite eye with opposite direction of action
 Pseudo or apparant Manifest (heterotropia) Concomitant Inconcomitant Paralytic Resterictive (kinetic)")
Squint True Latent (heterophoria) Pseudo or apparant Manifest (heterotropia) Concomitant Inconcomitant Paralytic Resterictive (kinetic)

A. Normal Orthotropia. B. Lt esotropia. C. Lt exotropia. D. Lt hypertropia.


Angle of squint

Pseudostrabismus Appearance of ocular deviation but the visual axes of both eyes are normally directed (far and near). Causes: Pseudo-esotropia: 1. Epicanthus: (skin fold covering the inner canthus). 2. High myopia: negative angle alpha. 3. Narrow interpupillary distance

Epicanthus
. Wide interpupillary distance.")
Pseudoextropia High hypermetropia (large angle alpha). Wide interpupillary distance.

Interpupillary distance

Pseudohypertropia � With ptosis

Pseudohypotropia � With lid retraction

Diagnosis of pseudostrabismus � Diagnosis of the cause. � Central corneal reflex in both eyes (normally directed visual axes). � Negative cover test. treatment of pseudostrabismus � TTT of the cause.
 � Tendency of the eyes to deviate but alignment is maintained")
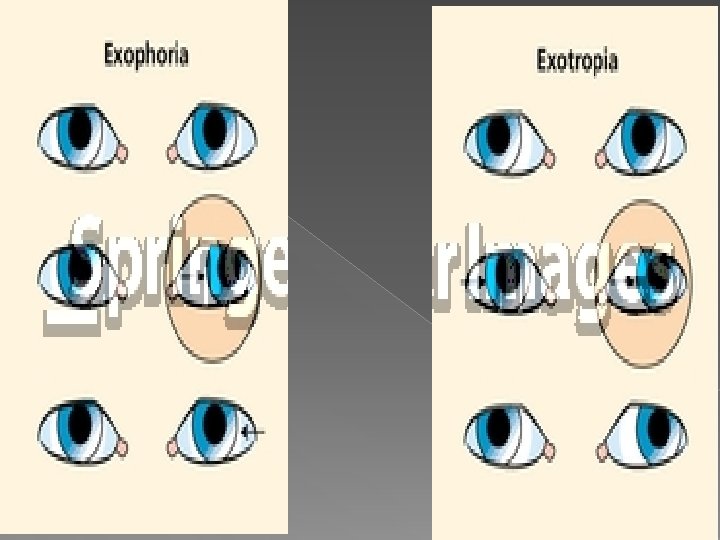
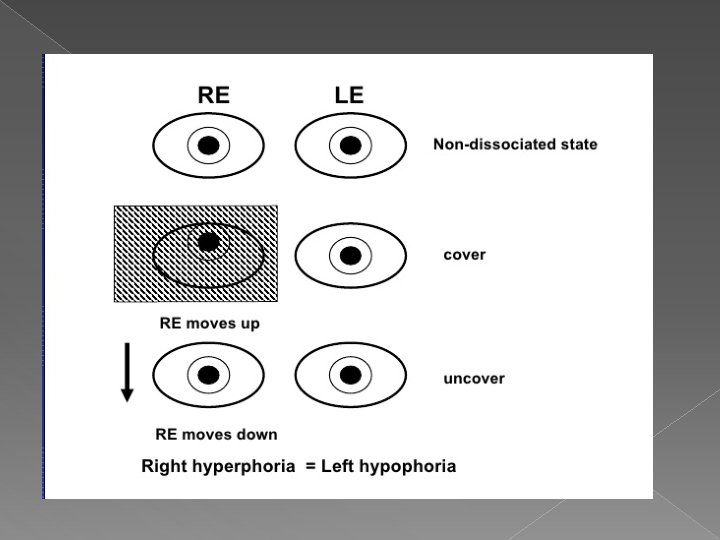
Heterophoria (latent squint) � Tendency of the eyes to deviate but alignment is maintained by effort. � Ocular deviation with abnormal direction of visual axis of one or both eyes when the binocular vision is dissociated as by fatigue or covering one eye.

Types of heterophoria Esophoria: tendency of both eyes to deviate in. Exophoria: tendency of both eyes to deviate out. Hyperphoria: tendency of one eye to deviate up. Hypophoria: tendency of one eye to deviate down. Cyclophoria: tendency of one or both eyes to rotate (incyclophoria, excyclophoria)
")
Causes of heterophoria � Uncorrected refractive error: (due to dissociation between accomodation and convergence) 1. Myopia leads to exophoria. 2. Hypermetropia leads to esophoria Slight weakness of one or more of the extraocular muscles. � Over-straining of the eyes: excessive close work lead to esophoria �
")
Accomodation and convergence (Near reflex)

Error of refraction Normal Myopia Hypermetropia
")
Causes of heterophoria � Uncorrected refractive error: (due to dissociation between accomodation and convergence) 1. Myopia leads to exophoria. 2. Hypermetropia leads to esophoria weakness of one or more of the extraocular muscles. � Over-straining of the eyes: excessive close work lead to esophoria �

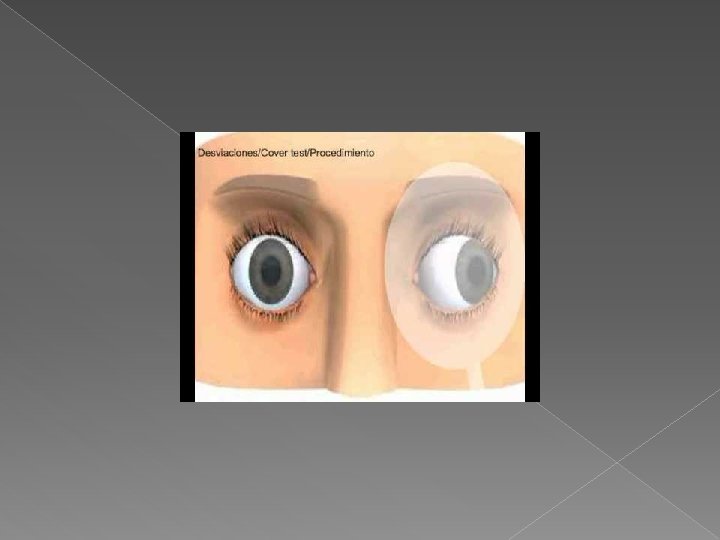
Diagnosis of heterophoria Symptoms: 1. Compensated heterophoria: no symptoms. 2. Decompensated heteropgoria: � Muscular athenopia (eye strain). � Blurring of vision and running of letters. �Intermittent diplopia. Signs: No ocular deviation if binocular vision is maintained. 2. Coveruncover test 1.


TTT of heterophoria Compensated heterophoria: no TTT. II. Decompensated heterophoria: A. Correction of the refractive error if present. B. Orhtoptic exercise: - to strenght the weak muscle. I. 1. Pencil-nose exercise in exophoria with convergence insuffiiciency.

TTT of heterophoria Compensated heterophoria: no TTT. II. Decompensated heterophoria: A. Correction of the refractive error if present. B. Orhtoptic exercise: - to strenght the weak muscle. I. 1. Pencil-nose exercise in exophoria with convergence insuffiiciency. 2. Exercising prisms: base of prism in the direction of latent squint e. g. base-in in esophoria.

TTT of heterophoria Compensated heterophoria: no TTT. II. Decompensated heterophoria: A. Correction of the refractive error if present. B. Orhtoptic exercise: - to strenght the weak muscle. I. 1. Pencil-nose exercise in exophoria with convergence insuffiiciency. 2. Exercising prisms: base of prism in the direction of latent squint e. g. base-in in esophoria. 3. Synoptophore.

TTT of heterophoria Compensated heterophoria: no TTT. II. Decompensated heterophoria: A. Correction of the refractive error if present. B. Orhtoptic exercise: - to strenght the weak muscle. I. 1. 2. 3. C. Pencil-nose exercise in exophoria with convergence insuffiiciency. Exercising prisms: base of prism in the direction of latent squint e. g. base-in in esophoria. Synoptophore. Relieving prism in spectecle: to neutralize deviation and relieve diplopia if orthoptic exercise fail (the base is against the direction of the latent squint e. g. base-out in esophoria)


TTT of heterophoria I. II. A. B. Compensated heterophoria: no TTT. Decompensated heterophoria: Correction of the refractive error if present. Orhtoptic exercise: - to strenght the weak muscle. 1. 2. 3. Pencil-nose exercise in exophoria with convergence insuffiiciency. Exercising prisms: base of prism in the direction of latent squint e. g. base-in in esophoria. Synoptophore. Relieving prism in spectecle: to neutralize deviation and relieve diplopia if orthoptic exercise fail (the base is against the direction of the latent squint): base bown on hyperphoria (used only in hyperphoria) D. Surgical TTT: if all above fail, we strenghten the weak muscle or weaken the overacting muscle C.
 Pseudo or apparant Manifest (heterotropia) Concomitant Inconcomitant Paralytic")
Manifest Squint squint True Latent (heterophoria) Pseudo or apparant Manifest (heterotropia) Concomitant Inconcomitant Paralytic Resterictive (kinetic)

Inconconitant paralytic squint Definition: ocular deviation with abnormal direction of visual axes of one or both eyes due to paralysis of one or more of the extraocular muscles in which the angle of deviation is variable in different direction of gaze.

Clinical picture Symptoms: � Binocular diplopia: in the direction of action of paralysed muscle. � Ocular deviation: in opposite direction to that of the paralysed muscle. � Vertigo, dizziness, uncertain gaze, nausea and vomiting.

Signs: 1 - Ocular deviation: -

Limitation of ocular motility: - Occurs in the same direction of action of paralyzed muscle e. g. outwards in LR paralysis. - It can be detected by asking the patient to follow the examiner's finger in the 6 cardinal directions. 2.

3 - binocular diplopia: � It is double vision when both eyes are opened.

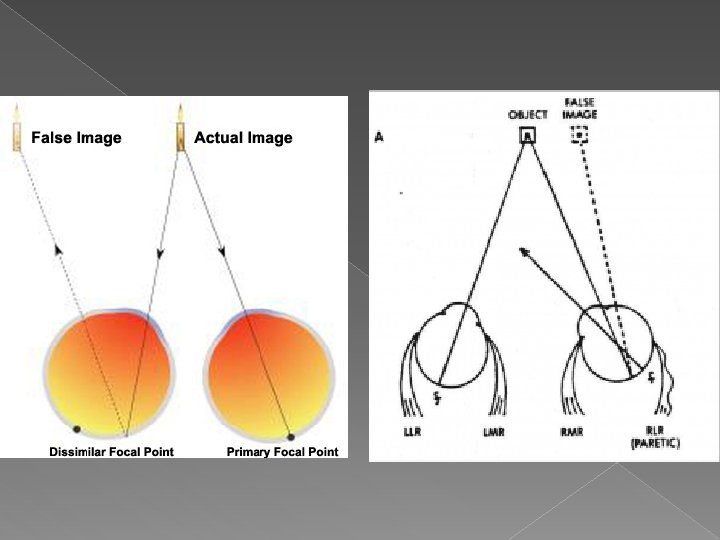
Cause of binocular diplopia: the 2 retinal images fall on non-correxponding points of the retina.
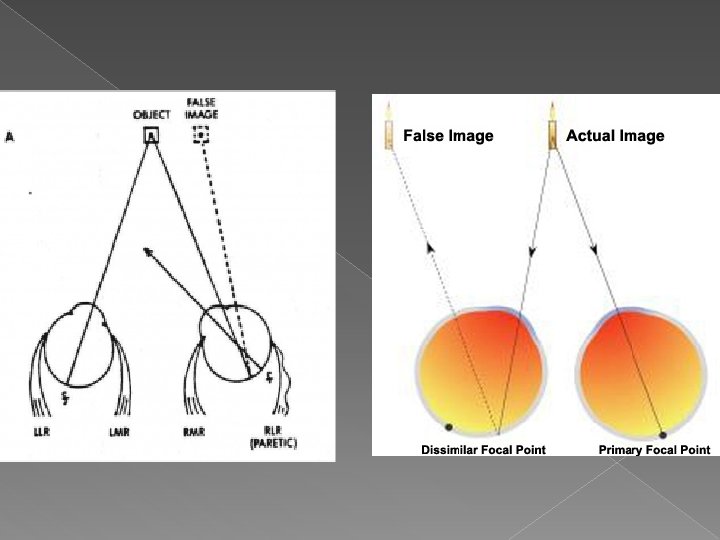

Criteria if binocualr diplopia: It disappears when one eye is covered unlike uniocular diplopia. 2) 2 different images are seen: 1) �True clear image seen by fovea of the normal eye. �False blurred image seen by point outside the fovea of the paralyzed eye and seen in the direction of action of the paralyzed muscle.

4 - binocular diplopia is marked in the direction of action of the paralyzed muscle N. B: in paralytic squint all manifestations occur in the direction of action of paralyzed muscle except for the ocular deviation which occurs in direction opposite to the action of the paralyzed muscle

Signs of paralytic squint Ocular deviation. 2. Limitation of ocular motility. 3. Binocular diplopia. 1.

Treatment of paralytic squint � TTT of the cause: DM, HTN. � Occlusion of one eye to avoid diplopia till the muscle regain its function with recovery within 6 months. � Relieving prisms: to relieve diplopia: Prism placed in front of saquinting eye with base against direction of deviation e. g. base-out in esotropia, base-in in exotropia, base-down in hypertropia.

Relieving prisms

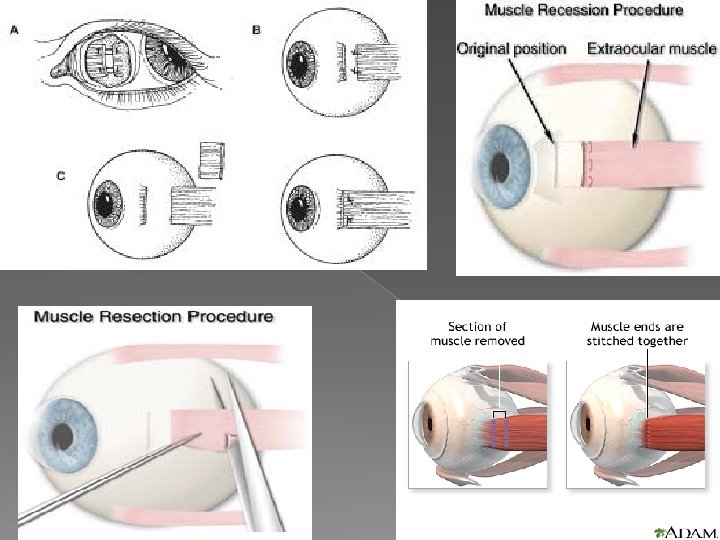
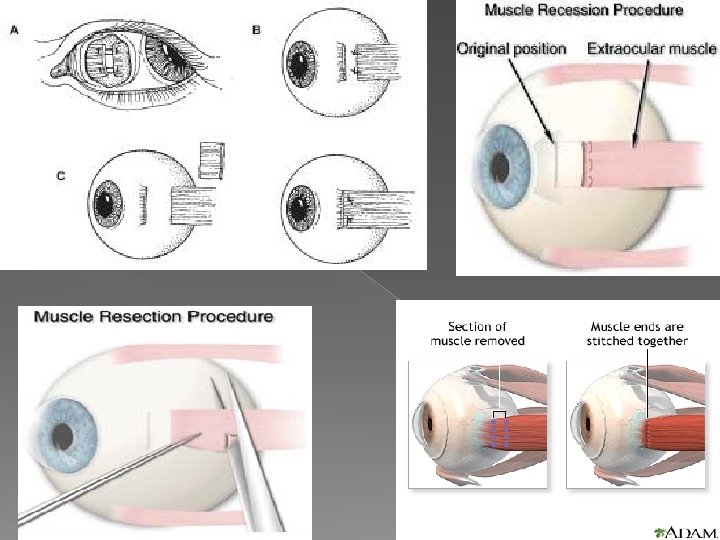
Treatment of paralytic squint TTT of the cause: DM, HTN. � Occlusion of one eye to avoid diplopia till the muscle regain its function with recovery within 6 months. � Relieving prisms: to relieve diplopia � Surgical ttt: 1. Waekening operations: � 1. Recession of direct antagonist. 2. Recession of indirect synergist. 2. Strenghtening operations: 1. Resection of indirect anatgonist. 2. Resection of the paressed (weak) not paralyzed muscle. 3. Muscle transposition: as in LR paralysis

Muscle transposition

Restrictive strabismus � It is strabismus characterized by irregular action of extra ocular muscle where there is reduction of the eye movement away from the action of the affected muscle e. g. fibrosis of MR the eye can not fully abducted. � It is confirmed by forced duction test which is positive � Most common causes is thyroid eye disease and orbital blow out fracture.
. Definition: it is ocular deviation with abnormal direction")
Concomitant squint � (concomitant= going together). Definition: it is ocular deviation with abnormal direction of visual axes of both eyes relative to each other in which the angle of deviation (angle of squint) is constant in different directions of gaze.

Types: A. According to direction of deviation: � � B. Esotropia. Exotropia Hypertropia Hypotropia According to laterality of deviation: � Unilateral: if the deviation is always by one eye. � Alternating: if the deviation is by either eye at a time

Aetiology 1. Error of refraction: �Hypermetropia associated with excessive accomodation the stimulate convergence leading to esotropia. �Myopia associated with lack of accomodation and less convergence leading to exotropia. Defective vision in one eye (amblyopia) as in complete unilateral ptosis, corneal opacities, cataract, macular lesion. 3. Weakness of extraocular muscle. 4. Central defect of vision. 5. Idiopathic 2.

Treatment of concomitant squint Aim of TTT: 1. To restore binocular vision. 2. To improve visual acuity. 3. To restore normal appearance (cosmetic).

Lines of TTT: 1. Correction of refractive errors. 2. Orthoptic treatment. 3. Amblyopia therapy. 4. Surgical treatment

Correction of refractive error � Full correction of hypermetropia to prevent use of accomodation so relieve esotropia. � Full correction of myopia to help convergence so relieve exotropia.

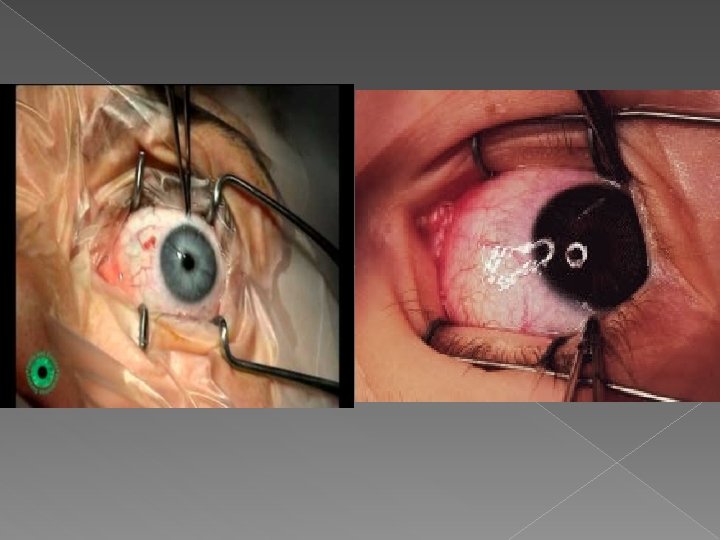
Surgical treatment Indications: 1. Residual angle of deviation after coorection of refractive error. 2. Strabismus with no refractive error. 3. Neglected strabismus above age of 10 years for cosmetic purposes only. Aim: � Strenghthening a muscle: resection. � Weakening a muscle: recession

Types of operation 1. Unilateral strabismus: �Esotropia: recession of MR and resection of LR. �Exotropia: recession of LR and resection of MR. 2. Alternating strabismus: �Esotropia: bilateral MR recession. �Exotropia: bilateral LR receeeion

- Slides: 69