Sjogrens Syndrome Pathogenesis and New Directions for Therapy



 • Aggressive lymphocytes (interstitial pneumonitis,")


![Sjogren’s Syndrome[1] Incidence: is only 0. 5% of the global population [2] About 90%](https://slidetodoc.com/presentation_image_h2/64c73d14c14ada2e49dab859ac426592/image-7.jpg "Sjogren’s Syndrome[1] Incidence: is only 0. 5% of the global population [2] About 90%")


 characteristic of Sjogren’s")
 with dry tongue")
")









 interfere with release of")
 • Production of autoantibodies •")

 • Natalizumab (Tsabri)- cell adhesion")


, CTLA")


-ACR 2012")









 (Tsp-/Tsp- mouse has Sjogren’s) NGF TGFb IL-1 b TNF")


 Immune and exocrine secretory functions (dryness)")


- Slides: 50
Sjogren’s Syndrome: Pathogenesis and New Directions for Therapy Robert I. Fox, M. D. , Ph. D. Scripps Memorial Hospital Scripps/Xi. MED Medical Center La Jolla, California robertfoxmd@mac. com
Why has it been so hard to develop successful therapies for Sjogren’s or SLE?
Roadblocks to Treatment of Dry Eyes and Dry Mouth • Problems with study design • Poor correlation with objective clinical and laboratory values • Concept of “functional circuit” not recognized by immunologists or Pharma— while it is the basis for neurologists and pain therapy
Therapy for Extraglandular Manifestations • Lupus-like vasculitis (immune complex) • Aggressive lymphocytes (interstitial pneumonitis, nephritis, lymphoma) • Responds to rituximab or cyclophosphamide • This is area where usually can show benefit with rituximab and otherapies
Goals for Therapy Fatigue, Myalgias and Cognitive Impairment • This is the “holy grail” of neuro-immunology to solve in the next decade. • Flu-like symptoms, “ jet lag, ” or after treatment of hepatitis C with IFN. • We have animal models from duloxetene (now for back pain) or modafinil (jet lag) • Molecular targets such as m. TOR.
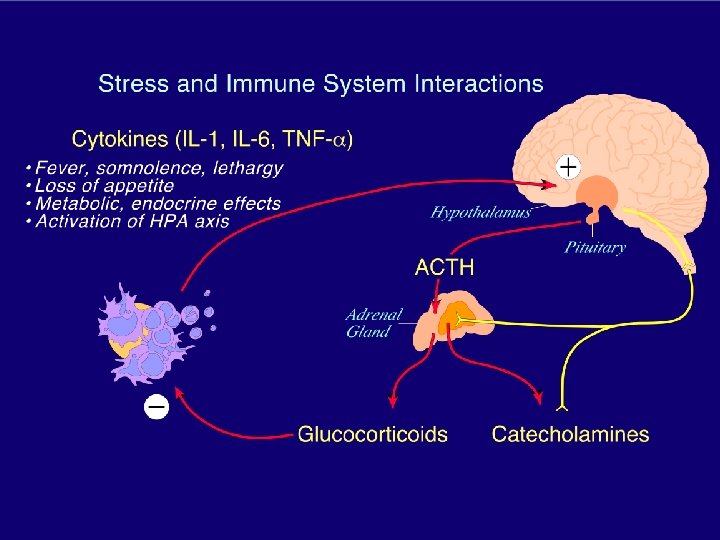
Fatigue and Cognitive Impairment • Much more common in SS or SLE than in RA What is that telling us about pathogenesis? • Involves the neuro-endocrine-immune axis associated with “stress” response (hypothalamic-adrenal axis) which we must add to innate and acquired responses as targets
Sjogren’s Syndrome[1] Incidence: is only 0. 5% of the global population [2] About 90% of S. S. patients are FEMALE Considered an “unmet need” by FDA and ACR Strong support from patient groups and Congress (key in approval of SLE therapies such as belumimab)
“QUALTITY OF LIFE”SS patients equated the impact of DRYNESS from SS on their quality of life at same level of limitation as patients with moderate angina (chest pain). They are willing to GIVE UP 2 YEARS OF LIFE to not have SS !!!
Factors NOT generally considered or able to be measured with blood / lab tests: • “DISABILITY” that is most commonly due to fatigue and cognitive impairment • “LIMITATIONS” on Activities of Daily Living (ADLs): ü dry eyes -- limits work--- (especially on computer) ü dry mouth -- interferes with sleep, occupational and social interactions (talking, eating) ü extra-glandular manifestations -(see next slides) • “Financial and emotional expense” of frequent need for “artificial tear” drops and dental decay treatment
EYE DRYNESS results in the clinical appearance of keratoconjunctivitis sicca (KCS) characteristic of Sjogren’s Syndrome The upper lid literally sticks to the Epithelial surface and pulls surface mucin layers off. The Rose Bengal dye retention test is like “rain water pooling in a street pothole” This test can be done at bedside and allows “triage” and rapid referral of patients to Ophthalmology
Severe “Xerostomia” (dry mouth) with dry tongue
Sjogren’s Syndrome-caused Cervical Dental Caries (cavities)
In order to understand why therapies used in RA are not “effective” We need to review the “functional” circuit which is recognized by Ophthalmologists and Pain Specialists (i. e. , phantom pain) but not by rheumatologists
Normal Tearing or Salivation Secretion requires a functional unit 5. gland water nutrients hormones 4. blood vessel water mucin protein 1. mucosal surface afferents efferents 2. lacrimatory or salivatory nuclei 3. cortical input central nervous system
Sjogren’s Syndrome affects functional unit Gland cytokines, Autoantibodies metalloproteinases ocular surface (cytokines, MMP, growth factor) Cholinergic efferents lymphocytes blood vessel Chemokines CAMs i. NOS adrenergic central nervous system (HPA axis)
Pathogenesis current interest usually concentrates on salivary biopsy as the model of inflammation. Misconceptions: a) The salivary gland is not destroyed in “dry” patients, but only about 50% of the ducts/acini are destroyed. b) The gland destruction is only mildly progressive with time (although symptoms may progress). c) Although subtle markers of biopsy predict lymphoma— this will not be “measurable” during clinical study.
In Sjogren’s Syndrome, many acini and ducts are spared Sjogren’s Normal
In Sjogren’s Syndrome 1. The residual glandular cells are partly paralyzed by the local immune reaction. 2. The sensation of dryness is a cortical event and poorly correlates with tear film (even with topical anesthetic).
Sensation of dryness at level of gland at CNS • Neural fibers (PGP 9. 5) still innervate residual gland including sympathetic and VIP/substance P
Normal Tearing or Salivation Secretion requires a functional unit 5. gland water nutrients hormones 4. blood vessel water mucin protein 1. mucosal surface (topical anesthesia) afferents efferents 2. lacrimatory or salivatory nuclei 3. CNS central nervous system
Reasons for Glandular Dysfunction in Sjogren’s 1. Cytokines inhibit neural transmission— (as we know from multiple sclerosis). 2. Metalloproteinases destroy matrix necessary for gland orientation.
Reasons for Glandular Dysfunction in Sjogren’s Cytokines (esp. IL-1, TNF) interfere with release of Ach/VIP from nerve endings and response to Ach by glandular cells
Steps in Pathogenesis • Homing to specific tissues (glands) • Production of autoantibodies • Pathogenesis of salivary gland lesions
Part of the cause of Sjogren’s is that lymphocytes “home” to the glands 3. When the homing receptor encounters vascular adhesive molecules, the lymphocyte enters tissue. CD 4+ Blood 2. Lymphs B cell 1. migrate through blood to tissues. Lymphocytes have surface “homing receptors” when generated in node or marrow.
Interfere with homing (obligate apoptosis if not bind “addressin”) • Natalizumab (Tsabri)- cell adhesion a 4 -integrin • Odulimomab (ICAM, CD 54, LFA-1)adhesion and migration • Fingolimod (Gilenya)sphingosine-1 receptor • CD 22 (Epratazumab)
Time course of autoimmune response* 1. Genetic factors predispose to Sjogren’s 2. Environmental factors such as a viral infection may lead to formation of autoantibodies. 2. Antibodies precede disease. 3. However, presence of antibody does not necessarily mean disease. Environmental Factor (virus-such as EBV) (apoptotic fragment) Innate (Toll receptor) Type I IFN Genetic Factors (includingsex) (including sex) (HLA-DR) Autoantibodies Immune system Immune complex Acquired Immune system (HLA-DR) T/B-cells Disease Manifestations Time period of years Ref. 32 -33
Gene expression profiling of minor salivary glands clearly distinguishes primary Sjögren's syndrome patients from healthy control subjects Arthritis & Rheumatism Volume 52, Issue 5, pages 1534 -1544, 5 MAY 2005 DOI: 10. 1002/art. 21006 http: //onlinelibrary. wiley. com/doi/10. 1002/art. 21006/full#fig 1
The main cytokine targets match those identified in genome wide screens* HLA-DR (T-cell), CTLA and IFN-g NF-K /Ik. B Homing receptor (CXCR 5) Type I IFN –IRF 5, STAT 4, TLR 3/7/9 and pk. R (cytoplasmic sensor) • B-cell activation –BLK, BAFF, IL 12, and A 20 (TNFAIP 3) • • * Most of these targets do not map to the encoded protein but to upstream sites of RNA transcription that are not translated (presumed epigenetic sites such as methylation)
Now we have methylation maps
These methylation maps show different targets
Previously Studied in SS • • Anti-CD 20 –glandular and extraglandular BAFF (Blys)-ACR 2012 abstracts* Abatacept (CD 40 L)-ACR 2012 Allogeneic mesenchymal cells-ACR 2012 abstracts and article in Blood • www. rheumatology. org/wren/acrsearch. asp? zoom_query=acr%20 abstracts%2 02012&st=nocache&actn=search&dt=12/24/2012%202: 29: 59%20 P
Other Inhibitors of IFN a. Initial trials of anti-type 1 IFN had infusion reactions and only modest efficacy b. Medi 546 (type 1 IFN-R antagonists) now in phase 1 (scleroderma) and juvenile SLE phase 2 trial
Rituxan may be back with Cytoxan for SLE…. and Sjogren’s
The true unmet need is the fatigue and myalgias— --this is the cause of disability-a) similar to influenza symptoms b) after hepatitis C, patients get interferon therapy c) “jet lag” symptoms d) depression All of these have been studied, but therapeutic models not applied to Sjogren’s syndrome
Neuropathy • Poor correlation between symptoms and objective findings: – Eye pain- does not correlate with tear flow; – Mouth pain- does not correlate with saliva; – Peripheral neuropathy- does not correlate with nerve biopsy; – Cognitive- does not correlate with acute phase reactants.
Fibromyalgia: The elephant in the room Fatigue Cognitive Dry eyes and dry mouth Nerve pain
Transcriptional Profiling Experiment 1. Challenge mice. Sacrifice 1 or 3 hrs later. Physiological LPS 10 µg/mouse IP Psychological Restraint 30 minutes 50 ml tube Fos immunoreactivity Saline LPS Restraint
Organization of the Paraventricular Nucleus Target Signature Function Median Eminence CRF ACTH secretion Posterior Pituitary OT AVP Pressor, antidiuretic Lactation, parturition, Autonomic CRF AVP OT Transmitter/modulators in central autonomic pathways
Similar pattern of Fos-ir in PVH neurons in response to distinct stressors Emotional Physiological
Therapeutic Models • We need to cross-screen therapeutic agents in our depression and pain models. • There are shared pathways— such as rapamycin (m. TOR) that have been used in models of depression (AKT pathway).
Thrombospondin modulates TGF-b (anti-inflammatory) (Tsp-/Tsp- mouse has Sjogren’s) NGF TGFb IL-1 b TNF
Monoclonals with drugs attached Time to mix immune modulator with neuromodulator How about an anti-cytokine with a neuro-modulator attached ? § Such as anti-lymphocyte plus cevimeline § Such as anti-ICAM plus duloxetene? § Such as anti-cytokine plus inhibitor of TGF-b or up-regulator thrombospondin?
Novel therapies Methylation and histone acetylation patterns — significant changes in Sjogren’s gland including the diurnal variation in saliva Micro-RNA regulation—a realistic possibility due to accessibility of eye and mouth to topical
Summary-1 Sjogren’s syndrome represents the interface of: a) Immune and exocrine secretory functions (dryness) b) Immune and neural function (neuropathy/cognitive) c) Immune and hypothalamic-adrenal axis (endocrine) d) Autoimmune proliferation and lymphoma a) e) Lupus-like features of vasculitis and immune complex
The way we perceive pain and suffering is under our control