Renal osteodystrophy chronic renal insufficiency GFR 60 mlmin
2 D 3")








D control q 3 -6 months GFR 60")

 polimer: Renagel® Mechanism of")

2 D 3 Calcitriol OH HO")








 Water po: Out (ml) 1400 Urine: 1500 Food: 850 Skin:")

![Hyponatremia [Na] ~ (Na content + K content) / TBW [Na] determines the volume](https://slidetodoc.com/presentation_image/2770e7522750971d2a8a961e81fc3dc8/image-26.jpg "Hyponatremia [Na] ~ (Na content + K content) / TBW [Na] determines the volume")



![Hyponatremia: therapy I Acute symptomatic hyponatremia • Stop water intake • Rise se [Na]](https://slidetodoc.com/presentation_image/2770e7522750971d2a8a961e81fc3dc8/image-30.jpg "Hyponatremia: therapy I Acute symptomatic hyponatremia • Stop water intake • Rise se [Na]")


![se[Na]=115 mmol/l, TBW= 40 L. Infuse 2 L normal saline/10 h, diuresis: 1, 2](https://slidetodoc.com/presentation_image/2770e7522750971d2a8a961e81fc3dc8/image-33.jpg "se[Na]=115 mmol/l, TBW= 40 L. Infuse 2 L normal saline/10 h, diuresis: 1, 2")









- Slides: 42
Renal osteodystrophy chronic renal insufficiency – GFR < 60 ml/min 1, 25(OH)2 D 3 VDR-binding VDR-number Ca Ca sensitivity PARATHORMON Osteitis fibrosa – high turnover Therapy P Ca Al PTH P Diab Vit D Adynamic bone Osteomalacia Low turnover
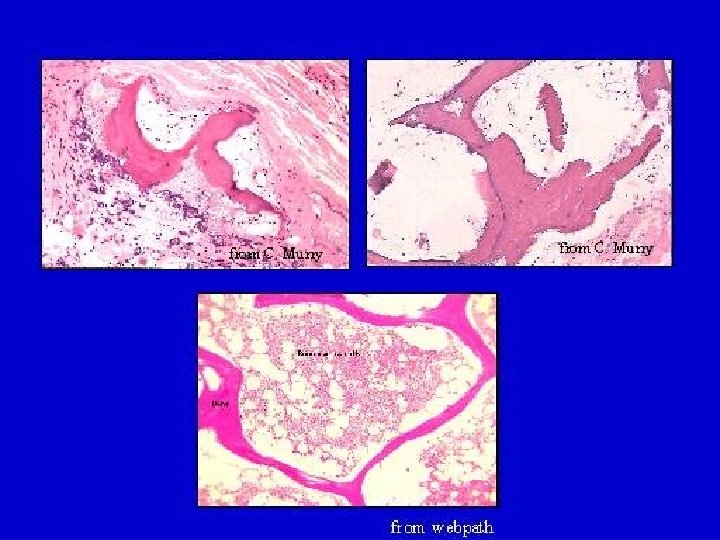
ROD - natural history • 176 patients, creatinin clearance: 50 -15 ml/min • Untreated • No complaints • Dg. : Bone biopsy • 56%: Osteitis fibrosa • 14%: Osteomalacia + osteitis fibrosa • 5%: Adynamic bone • 25%: Normal Hamdy et al. , BMJ, 1995
RENAL OSTEODYSTROPHY • Disease of bone remodelling - Abmormal structure - Low mineral content - Increased fracture risk - Bone pain - Proximal muscle weakness • Accelerated atherosclerosis • Calciphylaxis - Soft tissue calcification - Calcification of small vessels, nerves
Ca - deposition calcium . CRF ROD Ca content Plasma: 0, 025% Interstitial: 0, 075% Intracellular: 0, 9 % Bone 99% Kidney
Macroangiopathy, coronaria sclerosis
Bone mineralization vs vascular calcification • Bone density and vascular calcium content as measured by electron beam CT are inversely related. • Proteins characteristic of bone are also present in arteries: osteopontin, osteonectin, bone sialoprotein, matrix gla protein, osteocalcin
Se P, Ca x P product, PTH and mortality 6400 HD pts, age: 53 yrs, 30% Diabetic (Block et al. , AJKD, 1998. ) p < 0, 0001 p<0, 01 Mortality, RR p = 0, 03 1, 451, 75 1, 76 - 2, 11 - > 2, 53 2, 10 2, 52 Se P (mmol/l) 4352 Mortality is increased if PTH 53617360 72 132 Ca x P (mg 2/dl 2) < 65 pg/ml > 500 pg/ml
Calciphylaxis
ROD – therapy I During therapy, awareness is necessary to avoid atherosclerosis progression. Target values: • Calcium: 2, 1 -2, 39 mmol/l • Foszfor: 1, 13 -1, 8 mmol/l • Ca x P: < 4 mmol 2/l 2 • PTH: GFR 15 -60 ml/min: 65 -100 (? ? ) pg/ml Dialysis: 150 -300 pg/ml • 25(OH) D 3: 30 -50 ng/ml (75 -125 nmol/l)
ROD: therapy II Ca, P, PTH, 25(OH)D control q 3 -6 months GFR 60 -30 ml/min: Phosphate restriction: 800 -1000 mg/nap Ca CO 3: 700 -1400 mg/d (1 -2 t) D vitamin: 400 -800 IU/d P Ca CO 3 PTH > 65 -80 pg/ml: GFR 30 -15 ml/min: PTH > 100 pg/ml: Calcitriol 0, 25 μg daily or every other day Increasing P, Ca CO 3 Ca, Ca x P: Sevelamer, Paracalcitol, Calcimimetics Calcitriol 0, 25 μg daily or every other day
ROD – therapy III Applying current therapeutic approach, an increase in Ca x P product cannot be avoided in 10 -15 % of patients. What to do? • Aluminum- and calcium free phosphate binders • New vitamin D analogues that suppress PTH effectively but does not increase Ca- and phosphate absorption • Calcimimetics
Aluminum- and Ca free phosphate binder: Sevelamer: cross-bound (allylamin hydroclorid) polimer: Renagel® Mechanism of action Amine groups gain protons and bind phosphate by ion exchange and hidrogen bondage. Indications: Adynamic bone (ESRD: PTH < 150 ng/ml) Hypercalcemia (Ca > 2, 55), high Ca x P Severe vascular / soft tissue calcification
Sevelamer inhibits vascular calcification in hemodialysis patients Randomised study, sevelamer vs Ca-acetate, 200 patients p=0, 02 p=0, 04 sevelamer Change 0 -52 months % p<0, 0001 calcium mg/dl coronary score Ca x P hypercalcemia Chertow GM et al. : Kidney Int. 2002 Jul; 62(1): 245 -52. chol LDL
CH 3 OH OH CH 2 HO 1, 25(OH)2 D 3 Calcitriol OH HO OH 19 -nor-1, 25(OH)2 D 2 Paracalcitol
Comparison of Paracalcitol and Calcitriol Biologic action Effektivity vs Calcitriol PTH suppression 1/3 Ca absorption 1/10 Paracalcitol is three times more selective than calcitriol in terms of PTH suppression
Calcitriol resistant hyperparathyreosis treated by Paracalcitol 24 HD patients, PTH: 600 -800 pg/ml, calcitriol dose: 3, 2 µg/HD Paracalcitol starting dose: {calcitriol dose} x 3 PTH pg/ml 750 500 250 7 (Llach et al. AJKD, 2001) 4 2 1, 5 Paracalcitol: µg / HD
Calcimimetics • Ca receptor: low affinity, non-specific • Expression: parathyreoids, C cells, nephron, bone, brain • Secunder hyperparathyroidism: low Ca. R expression • Calcimimetics: increase Ca sensitivity of Ca. R • Indications: primary- and secundary hyperparathyroidism - Effects of 50 -100 mg/d AMG 073 : Decrease (%) PTH Ca Ca x P 25 -30 3 -5 10 -15
Calcimimetics in clinical practice • Randomized, placebo controlled, 18 wk study, 78 HD patients • AMG 073: 20 -50 mg/d vs placebo • Otherapy: Calcitriol: 64%, phosphate binder 87% • Baseline PTH: 623 pg/ml p<0, 001
Invasive therapy 30 -40 mg > 500 mg Indications - Symptoms: severe hypercalcemia severe bone disease calciphylaxis pruritus myopathy - PTH > 1000 pg/ml Surgery: total parathyreoidectomy + autotransplantation Ethanol / calcijex infiltration
Water: 60%body. WT Posm= 275 -290 m. Osm/kg Eff Posm= 270 -285 m. Osm/kg Extracellular: ECF 20% Body Wt H 2 O No of particles constant : ICF • Water and sodium balance maintains normal tonicity of body fluids and normal effective circulating volume. • Tonicity = effective osmolality resulting from the restriction of particles to a compartment. It determines the volume of a compartment. • Effective circulating volume maintains normal perfusion of tissues. • Control of sodium- and water balance is independent.
Na/ K/ 2 Cl
Regulation of water balance Interplay of ADH and thirst Regulation: • tonicity ~ se Na. tonicity: ADH + thirst tonicity: no ADH, water diuresis • effective volume: ADH + thirst even in the presence of tonicity ! • Drugs • Nausea, pain Expected urine Osm during hyponatremia: 20 -80 m. Osm/kg
Water balance In (ml) Water po: Out (ml) 1400 Urine: 1500 Food: 850 Skin: 500 Oxidation: 350 Respiration: 400 Stool: 200 Total: 2600 [Na] ~ (Na content + K content) / TBW 2 x [Na] ~ Eff Posm 2 x [Na] x TBW = total effective osmoles 2600
Regulation of sodium balance Effective circulating volume effective circulating volume: Angiotensin II Aldosteron Na conservation ADH/Thirst effective circulating volume: No Angiotensin II No aldosteron ANP BNP Natriuresis Low effective circulating volume: high urine Osm UNa < 10 mmol/l
Hyponatremia [Na] ~ (Na content + K content) / TBW [Na] determines the volume of the ICF. Na content determines ECF. Hyponatremia: [Na] < 136 mmol/l and low plasma Osm: Posm< 275 m. Osm/kg Low [Na] but plasma Osm not low: Pseudohyponatremia: hyperproteinemia, hyperlipidemia Hyperglycemia: elevation of [glu] by 4 mmol/l will reduce [Na] by 1 mmol/l Expected renal response: maximally dilute urine: Uosm 20 -80 m. Osm/kg Normal kidneys can make 12 l electrolite free water / day. Development of hyponatremia requires: ADH Renal failure- low GFR Depletion of osmoles (min U-Osm: 20 -80 m. Osm/kg H 2 O) Vurine = Excreted osmoles / Uosm
Causes of hyponatremia ECF Low Not low Effective circulating volume Primary Na loss Urine Na < 10 mmol/l Low > 20 mmol/l Heart failure Non-renal loss (burns, sweat) Not low Urine K High Low Remote diuretic Remote vomiting Vomit. Diur. Renal Na wasting Addison`s SIADH: Liver cirrhosis CNS lesion Low albumin Lung cc, inf. i. e. edema states Drugs Low cortisol Post surgery Hypothyroidism Nausea Reset osmostat
Drugs affecting ADH action Stimulate secretion Potentiate action Inhibit nicotine caffeine ethanol morphine aminophyllin haloperidol tricyclic antidepressants aspirin carbamazepine vincristine NSAIDs clonidine cyclophosphamide glucocorticoids
Consequences of hyponatremia • Cell swelling- cerebral edema • Brain cells are the only ones that regulate their volume by changing the number of intracellular particles (osmolytes) - it takes several days to adapt. • Acute (whithin 1 -3 days) hyponatremia: symptomatic Symptoms: nausea headache lethargy, obtundation seizures, permanent neurological deficits death
Hyponatremia: therapy I Acute symptomatic hyponatremia • Stop water intake • Rise se [Na] until symptoms stop or by 6 mmol/l whichever comes first. • Use 3 % Na. Cl for replacement. 3 % Na. Cl = 30 g/l = 513 mmol/l • To rise [Na] by 6 mmol/l in a 70 kg patient: 42 L TBW. Needs 42 x 6 = 252 mmol Na. Cl = 490 ml 3% Na. Cl • Reduce rate of rise to 0, 5 mmol/l/hr, limit daily rise to 12 mmol/l.
Hyponatremia: therapy II Chronic, asymptomatic hyponatremia • Beware of acute recognition of a chronic problem! • Too fast rise of se[Na] will cause central pontine myelinolysis. • Do not permit se[Na] to rise more than 0, 5 mmol/l/hr and 12 mmol/l/day. • Administration of KCl to treat hypokalemia will rise se[Na]: Na leaves cells as K enters. There is 13, 5 mmol K+ in 10 ml 10% KCl. • To determine the impact of urine excretion on se[Na], measure urinary Na + urinary K! Potassium in the urine eventually comes from cells. As K leaves the cell Na enters. If (U[Na] + U[K ]) > se[Na] : se[Na] decreases If (U[Na] + U[K ]) < se[Na] : se[Na] rises Electrolite free water clearance = V [1 - (UNa + UK)/se. Na]
Hyponatremia: therapy III Hyponatremia and a contracted ECF volume • Decifit of Na and water in ECF, surplus of water in ICF • Goal: reexpand ECF by giving Na and move water out of cells. • Do NOT give hypertonic saline!! • 1 mmol Na. Cl / TBW will rise se[Na] by 1 mmol/l and expand ECF by 2%. • For rapid expansion of ECF (shock) use iv solution isotonic to the patient! If se[Na]=115 mmol/l: give 50 -50% of 0, 9% (155 mmol/l) and 0, 45% (75 mmol/l) saline. • For slow expansion of ECF may use 0, 9% Na. Cl. • Correction of ECF blocks ADH and induces water diuresis: danger of too rapid [Na] rise: may have to give aeqous vasopressin (desmopressin).
se[Na]=115 mmol/l, TBW= 40 L. Infuse 2 L normal saline/10 h, diuresis: 1, 2 l/ 10 hr, urine (Na + K) = 40 mmol Total osmoles = 40 L x 230 m. Osm/L = 9200 m. Osm New TBW = 40, 8 L, New total osmoles = 9200+620 -50=9780 m. Osm New se. Osm= 9780 m. Osm / 40, 8 L = 240 m. Osm/L New [Na] = 120 mmol/l Rise of Na = 5 mmol/10 h = 0, 5 mmol/h
Hyponatremia: therapy IV Hyponatremia and expanded ECF volume • Surplus Na and surplus water • Limit intake of water and Na • Augment urinary water- and Na+ loss by loop diuretic • Replace part of Na+ loss if se[Na] rise < 0, 5 mmol/h (use hypertonic solution) • Beware of overexpansion of ECF • Replace part of water loss if se[Na] rise > 0, 5 mmol/h • Replace K+ loss
Hypernatremia Se Na > 144 mmol/l and Posm > 290 m. Osm/kg Expected response: maximal Uosm (> 1000 m. Osm/kg), sg: 1025 -1030 minimal urine volume (~ 0, 5 l/day) THIRST (provoked by 2% elevation of [Na]) Minimum urine volume= osmoles to be excreted / maximum achievable Uosm Eg. : 800 m. Osm to be excreted (urea, Na. Cl, NH 4), max Uosm = 200 Osm/kg Minimum urine volume: 4 L
Causes of hypernatremia Expanded ECF Na gain e. g. iatrogenic U-vol. : min. Uosm: max. Non renal water loss Decreased body weight No change of BW What is Uosm and U-vol? Water shift: seizures, rhabdomyolysis Polyuria, Uosm: not maximal Uosm > 300 m. Osm/kg Osmotic diuresis glucose urea mannitol (UNa: 50 mmol/l UK: 25 -50 mmol/l) Diuretics Uosm < 250 m. Osm/kg Rise of Uosm and decrease of U-vol post ADH? Yes Central DI No Nephrogenic DI
Diabetes insipidus: polyuria and polydipsia - there is no hypernatremia as long as patient has access to water. Central diabetes insipidus Nephrogenic diabetes insipidus • Craniopharingeoma • Congenital • Metastasis • Hypercalcemia • Transsphenoidal surgery • Hypokalemia • Head trauma • Lithium • Hypoxia • Amyloidosis • Sarcoidosis • Pyelonephritis • Encephalitis, meningitis • Polycysitic kidneys • Cerebral aneurism • Sjögren sy
Evaluation of polyuria Water restriction test Measure U-vol, Uosm and body weight hourly Continue test until Uosm reaches a plateau or Posm reaches 295 -300 m. Osm/kg Do not allow more than 3 % decrease of body weight. Normal: U-vol to minimum, Uosm to 1000 m. Osm/kg Diabetes insipidus: no change in U-vol and Uosm Primary polydipsia: decrease of U-vol, increase of Uosm ~ 600 m. Osm/kg Give 10 µg desmopressin nasally: Central DI: Rising Uosm, decreasing U-vol Nephrogenic DI: no change
Symptoms of hypernatremia Cell shrinkage Lethargy, weakness, irritability, twitching, Intracranial hemorrhage, seizures, coma, death Fever, nausea, vomiting Labored respiration Adaptation: accumulation of osmolytes in brain cells takes several days
Therapy of hypovolemic hypernatremia • Estimate ECF volume contraction on clinical grounds: 10% deficit is just detectable, 30 % deficit causes shock. • To replace ECF volume give 0, 9 % saline. • Stop ongoing water loss : ADH replacement in DI, look for osmotic agent • Calculate water deficit: Desired TBW = present [Na] x TBW / desired [Na] Add electrolite free water diuresis • To replace water give water po or D 5 iv or 0, 45% saline. • Rate of D 5 should not exceed 300 ml/h. • 0, 45% saline will only be effective if U[Na] + U[K] > 75 mmol/l - give furosemide if necessary and replace water + K lost in urine. • Rate of [Na] decrease should not exceed 0, 5 mmol/h and 12 mmol / day
Therapy of diabetes insipidus Therapy of central diabetes insipidus: 10 -20 µg / d desmopressin (DDAVP) intranasally Therapy of nephrogenic diabetes insipidus: salt restriction + thiazide diuretic, correction of potassium and calcium
Therapy of hypervolemic hypernatremia Discontinue offending agent Furosemide Replace part of water Replace potassium In case of renal failure: dialysis