Migraine and other headaches Dr David Kernick Exeter







 n Tension")
















")


 (Loughey)")






 Secondary")


























 Muscle tension Mandibular Anxiety-depression")






. n Triptan n Not opiates")












 Keep constant n")









- Slides: 101
Migraine and other headaches Dr David Kernick Exeter Headache clinic
Outline n Where does headache come from? n Epidemiology n Classification n Management
HEADACHE – pain from cranium that can be reffered to or from the neck and face
Extra cranial origin
Where does the pain come from? Extra - cranial n Arteritis n Neuralgia n Muscle tension n Facial structures
Intra cranial pain
CSF – 20 mls/hr, 150 mls capacity
Where does the pain come from? Intra – cranial (dural pain fibres) n Tension – raised intracranial pressure n Compression – tumour n Inflammation - migraine, meningitis, blood
From neck
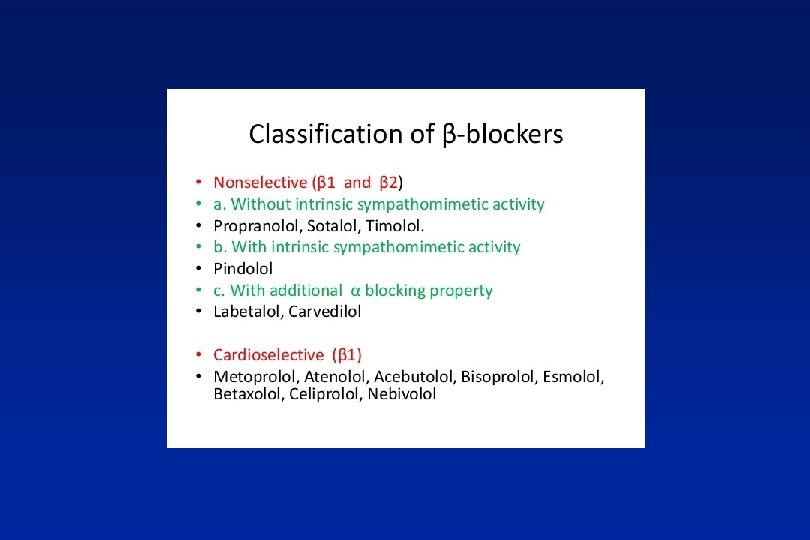
Migraineur on metopralol. Uses salbutamol inh 5 times a week.
Respiratory effect of beta-blockers in people with asthma and cardiovascular disease: population-based nested case control study Daniel R. 2017
35, 502 with active asthma and CVD 14. 1% and 1. 2% were prescribed cardioselective and non-selective beta-blockers Results Beta-blocker use was not associated with a significantly increased risk of moderate or severe asthma exacerbations. Conclusion Cardioselective beta-blockers in asthma and CVD were not associated with a significantly increased risk of moderate or severe asthma exacerbations and potentially could be used more widely when strongly indicated.
Outline n Where does headache come from? n Epidemiology n Classification n Management
Epidemiology n Prevalence n Incidence n Impact – Qo. L, Economic n Health seeking behaviour
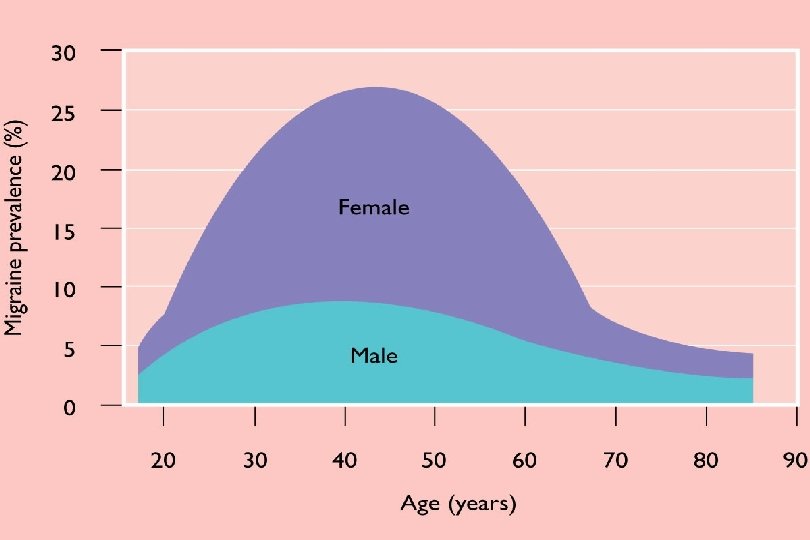
Headache annual prevalence n Population: n Tension type 70% n Migraine 12%, n Cluster 0. 1%
Annual Migraine incidence
Epidemiology n Prevalence n Incidence n Impact – Qo. L, Economic n Health seeking behaviour
National Challenge Reference Approximately 9 million people live with migraine in the UK Migraine: the seventh disabler (Steiner et al 2013) Migraine is the second leading cause of years lived with disability Global Burden of Disease (The Lancet 2016) 25 million days lost from work or school each year in England because of migraine alone The prevalence and disability burden of adult migraine in England their relationships to age, gender and ethnicity. (Steiner et al 2003)
Headache impact n 20% adult population – headache impacts on their quality of life Kernick 2001
Impact upon children Kernick BJGP 2009 n 20% - 1 or more headaches each week, significant impact home or school
University new entrants Kernick 2002 n 1124 students n 21% headache that impacted on life n 13% > 15 days of the month n 45% seen a GP n <5% prescribed medications for headache
Epidemiology n Prevalence n Incidence n Impact – Qo. L, Economic n Health seeking behaviour
When people develop headache what do they think they have? What do GPs think they have? What do they actually have?
When people come to see you what do they think they have? n Need glasses n Blood pressure n Brain tumour
What do GPs think when patients present with headache? (Kernick 2008)
What do patients have when they present to GP with headache? Landmark Study n 85% migraine n 10% Tension type headache n 5% secondary headache n <1% other types of headache
What happens? n Less than 50% migraineurs will see GP n Less than 10% will receive Triptan Walling 2006 n 10% of those who would benefit from prevention receive it Rahimtoola 2005
What happens? n 3% GP presentations are referred to secondary care (25% children) (Loughey) n 30% of neurology referrals are for headache (Hopkins)
What do patients have when they present to A and E with headache? Valade 2000 n n n Migraine TTH Cluster Trauma Trig Neuralgia Sinusitis Vascular disorders Low Pressure Meningitis Tumour Other Misc 55% 25% 7% 1. 6% 1. 2% 0. 35% 0. 17% < 5%
What is the unmet need in primary care? Kernick Journal of Headache and Pain 2008 n < 50 % adults, <10% children see GP
Why don’t people seek help?
Why don’t people seek help? n Can’t measure n Only a headache n Everyone gets them – natural n No one takes me seriously n Parents don’t want to reinforce illness behaviour - pattern their health seeking behaviour
How should we deliver headache services n Self management n GPs first line management n GPSI support n Tertiary headache centres
Outline n Where does headache come from? n Epidemiology n Classification n Management
IHS Headache classification Primary n Migraine n Tension type n Autonomic cephalalgias (cluster) Secondary n n n n Traumatic Vascular Non-vascular (SOL) Substance induced Infection Disturbed homoestasis Facial structures
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
70 year old drug review n Simvastatin n Thyroxine n Amlodipine n Bendrofuazide n Developed dull L sided headache. Gets pain in his jaw on eating. Should he see the dentist?
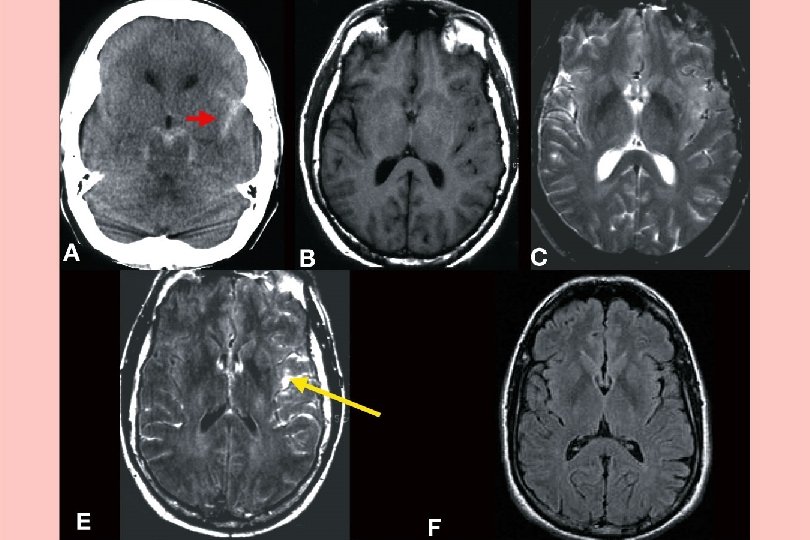
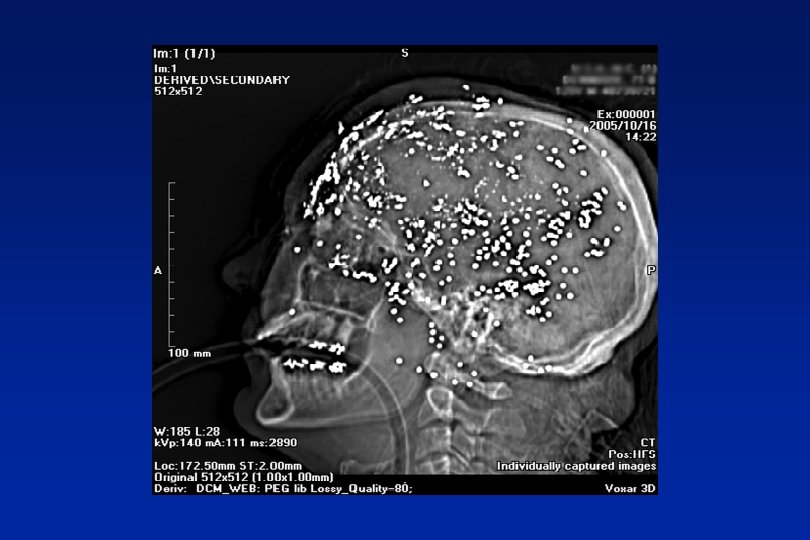
Sub Arachnoid - thunderclap headache
Reversible vasoconstriction syndrome Vasoconstrictor drugs, SSRIs, Cannabis
Thrombophilia
Meningitis
Malignant hypertension
Temporal arteritis • Can be bilateral • Systemically unwell • Tender artery with allodynia • CRP better than ESR • Problem with skip lesions
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
Exercise headache 1/3
Pressure – too high. Idiopathic intracranial hypertension n Non specific headache n Tinnitus n Visual field/acuity defect n Papilloedema
CSF – 20 mls/hr, 150 mls capacity
Pressure too low
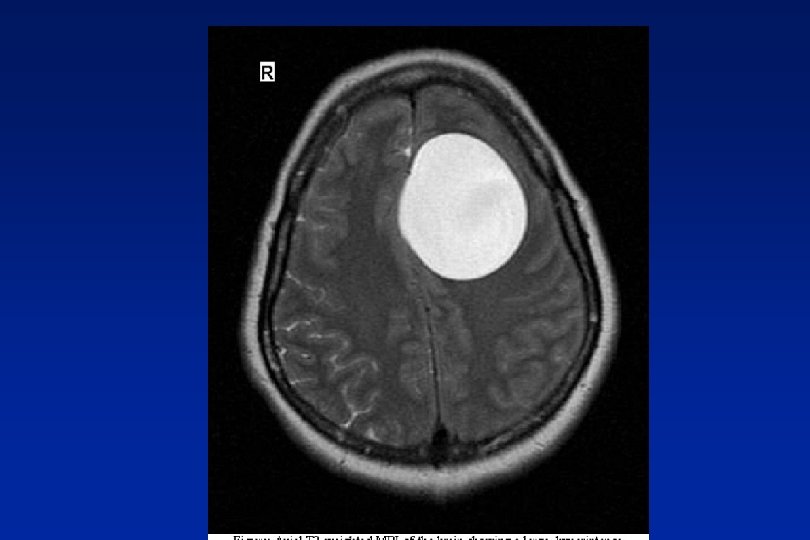
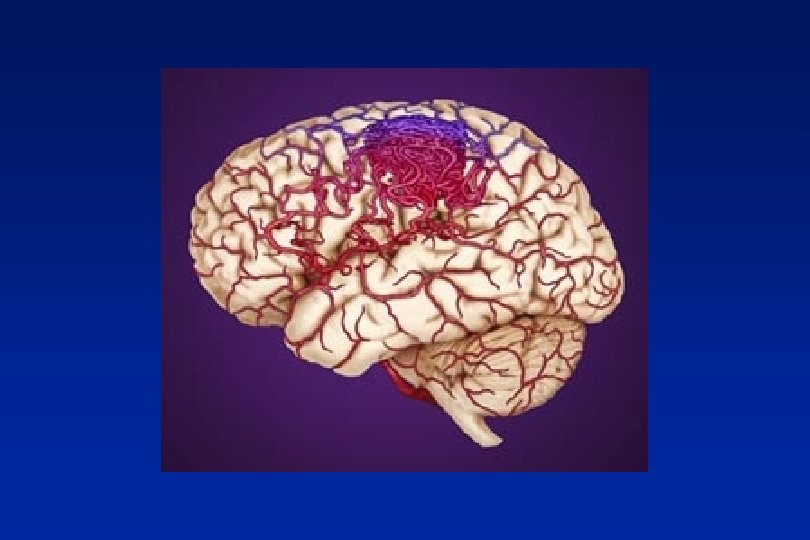
Space occupying lesions Stretch, compression, blockage n Benign – cysts, A-V malformations n Malignant – primary secondary
Red Flags n Abnormal neurological symptoms or signs n History of cancer elsewhere
Orange Flags n Aggregated by Valsalva manoeuvre n Headache with significant change in character n Awakes from sleep n New headache over 50 years n Memory loss n Personality change
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
Drug review n 1. Paracetamol, co codeine or Ibuprofen on 17 days of month n 2. Sumatriptan 8 days of month n Is he likely to have MOH, from 1 or 2? Which drug is most likely to cause a problem?
Medication overuse Headache n 3% of population n Analgesics > 15 days of month n Triptans > 10 days of month
Medication overuse headache Headache intensity Withdrawal of all analgesia Increased frequency of headache, associated with increased frequency of analgesia use. Daily headache with spikes of more severe pain Migraine attacks Frequent ‘daily’ headaches Return of episodic headache Management?
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
Primary Headaches n Migraine n Tension Type n Cluster n n n Paroxysmal hemicrania Hemicrania continua SUNCT Primary cough headache NPDH ect
A 30 year old male n Pain in L eye n Lasts 30 minutes, 5 times a day n GP diagnosed migraine given oral sumatriptan 100 mg and propanolol 160 MR but not working?
Cluster - Autonomic Cephalopathy n High impact ++ n Peri-orbital clusters 15 mins - 3 hours n Cluster attacks and periods n Unilateral autonomic features n Acute or chronic
Cluster treatment n Injectable Sumatriptan n Nasal Zolmitriptan n Short term steroids n Oxygen 100% n Verapamil
Tension type headache Cervico-genic (degenerative change, trigger spots) Muscle tension Mandibular Anxiety-depression
Migraine – the default diagnosis
1. 2. 3. 4. 5. Migraine generator – gastric and cervical implications Central and peripheral sensitisation Activation trigeminal nerve Peripheral inflammation Cortical depolarisation and vasoconstriction Classifying headache 2
Implications for gastric stasis and neck pain
Migraine: A Featureful Headache Premonitory Mood changes Fatigue Cognitive changes Muscle pain Food craving Preheadache Early Headache Aura Advanced Headache. Postdrome Dull headache Fully reversible Nasal congestion Neurological changes: Visual Muscle pain somatosensory Mild Unilateral Throbbing Nausea Photophobia Phonophobia Osmophobia Moderate Headache Severe Fatigue Cognitive changes Muscle pain Post headache Time
In practice n Recurrent headache that bothers n Nausea with headache n Light or sound bothers n Invariably a family history
Migraine co-morbidities n Anxiety n Depression n IBS n Asthma n Epilepsy
Migraine Acute treatment n Paracetamol, Aspirin, Prokinetic (Domperidone/metochlorpropramide). n Triptan n Not opiates
Triptans
Triptan Half Life
n Severe nausea, often vomits n Sumatriptan 50 mg only partially effective
Options n Anti emetic n Take early n Change the dose n Change formulation (nasal, wafer, inj) n Change the Triptan (failure not a class effect)
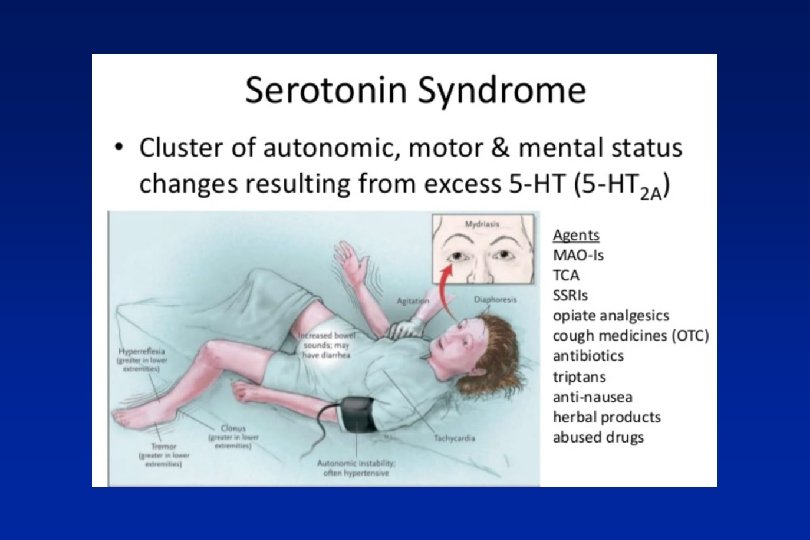
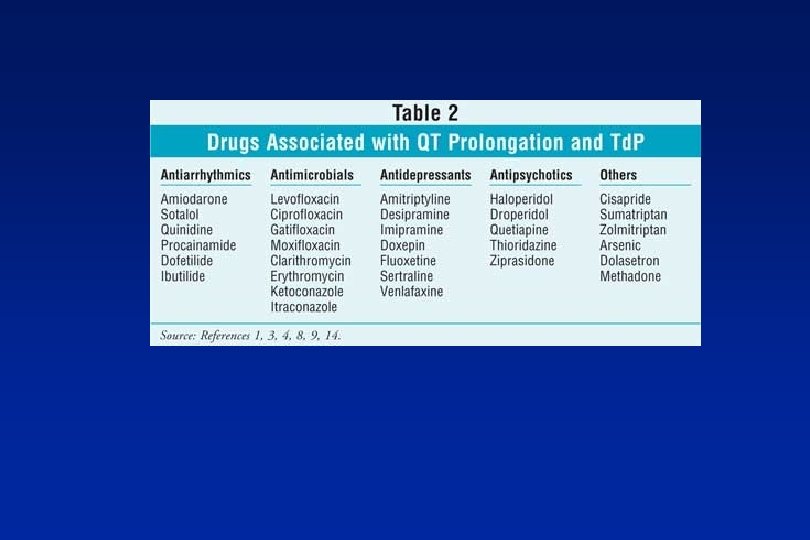
Taking Sumatriptan 100 mg Which cause you concern? n On COC pill n Age 69 n Past history TIA n Started SSRI
Triptans – some practical points n Treat early n Formulation? n Failure not class effect n Not in CVD n SSRIs n Over 65 years
Migraine treatment Preventative n When to instigate? n How long for to assess an effect? n What rate dose increase? n How long on preventative medication? n What to use?
Preventative Medications in Migraine Cupboard 2 Cupboard 1 Gabapentin / Pregabalin Cupboard 3 Propranolol Candesartan Other anti-epileptics Amitriptyline Venlafaxine / Duloxetine Lisinopril Topiramate Flunarizine (requires hospital prescription) Sodium Valproate (not in women of childbearing age) Pizotifen
Migraineur on verapamil, domperidone, Triptan. Just started on Amitriptyline
Patient read in Daily Mail about new “breakthrough” drug. How do you advise?
CGRP antagonists
Non – drug options
Triggers/lifestyle n Triggers – yes n Lifestyle - yes (including hormones) Keep constant n Food allergy - no
Naturally occurring drugs n Magnesium – ? yes n Co Q 10 – ? yes n Feverfew, butterbur, riboflavin – possibly
Needles – occipital nerve injection
Needles - Botox BOTOX® for Chronic Migraine n UK licence for Chronic Migraine, NICE approved n ≥ 15 days headache of which ≥ 8 days are migraine n Rejected by SMC (2011 and 2013) n Starting to be used in patients where most other treatments have failed Double-blind phase: BOTOX® vs. placebo Open-label phase: All patients on BOTOX® Mean change in frequency of headache days from baseline (days/28 -day period) Study week 0 0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 BOTOX® (n=688) Placebo (n=696) -2 -4 -6 -8 -10 -12 -14 p<0. 001 p<0. 001 p=0. 008 p=0. 01 p=0. 047 p=0. 007 p=0. 011 p=0. 019
Needles - accupuncture
Psychological approaches n Cognitive therapy, mindfulness
Electrics
Transcutaneous vagal nerve stimulation
Supra-orbital nerve stimulator
In summary n Lot of it out there n Significant impact n Needs unmet