Migraine and Headaches Anish Bahra Headache Service NHNN

Migraine and Headaches Anish Bahra Headache Service NHNN

Migraine vs Headache

Classification of Head and Facial Pain Disorders Part II The Primary Head and Facial Pain Disorders The Secondary Head and Facial Pain Disorders

Classification of Head and Facial Pain Disorders Part I The Primary Head and Facial Pain Disorders Part II Primary Care 0. 1% A&E ~ 8%`

Primary Headaches Prevalence Tension-Type headache 20 -87% Migraine 12% Cluster headache & related disorders ≤ 0. 2% Other Primary headaches Uncommon

Normal Prodrome Aura Resolution Normal Headache Appetite Awake/sleep g vin a r C ing wn a Y ed Tir a use a ia N x e or g An nin w Ya y p e Sle Vomiting Deep Sleep Photophobia Phonophobia Osmophobia Smell Fluid balance Tire d Fee Hig ling h/L ow Light tolerance Noise Lim ite tole d food ranc e ed ten n h g i o He cepti r pe Appetite Awake/sleep Light tolerance Noise Smell id Flu Diu resi s tion n e ret Blau, Lancet 1992 Fluid balance

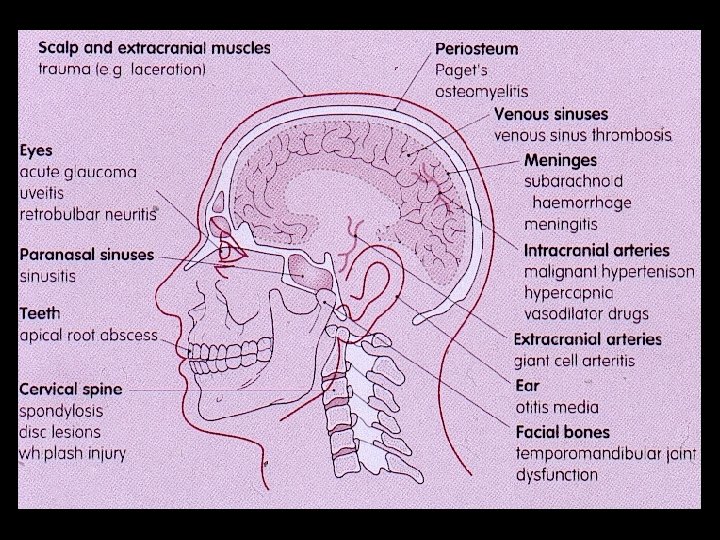
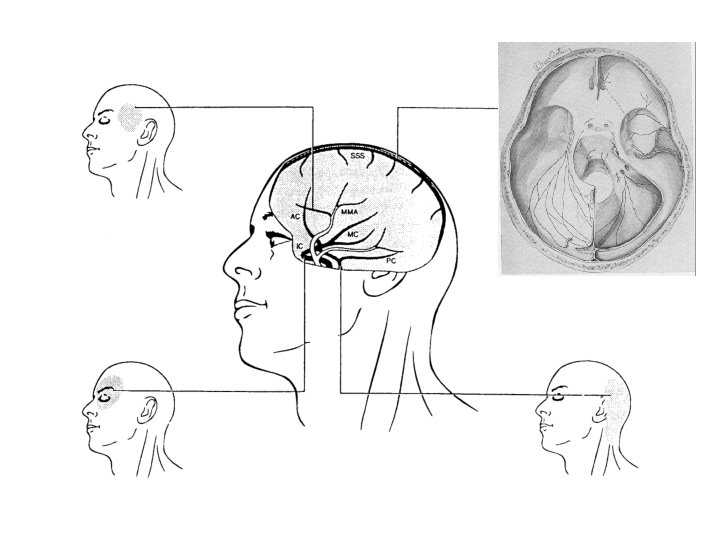
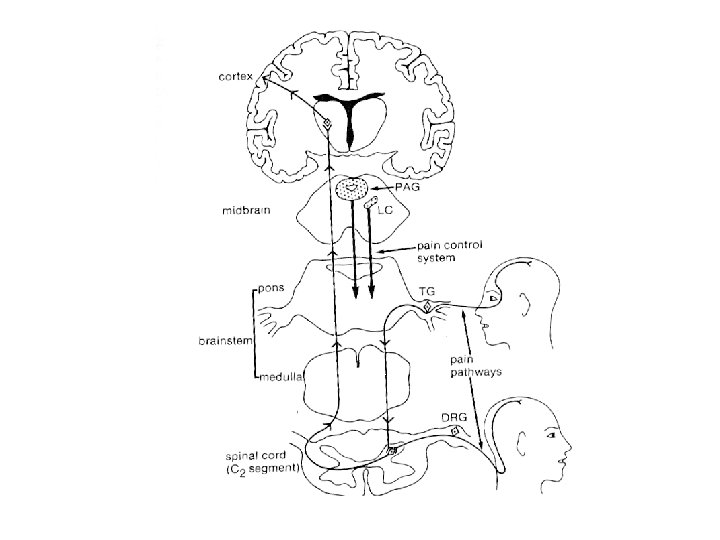
Cause of Headache

Normal Prodrome Aura Resolution Normal Headache Appetite Awake/sleep g vin a r C ing wn a Y ed Tir a use a ia N x e or g An nin w Ya y p e Sle Vomiting Deep Sleep Photophobia Phonophobia Osmophobia Smell Fluid balance Tire d Fee Hig ling h/L ow Light tolerance Noise Lim ite tole d food ranc e ed ten n h g i o He cepti r pe Appetite Awake/sleep Light tolerance Noise Smell id Flu Diu resi s tion n e ret Blau, Lancet 1992 Fluid balance

New onset Migraine coinciding with new area of inflammation MS : Haas, Headache 1993

Hypothalamic Neurostimulation in Cluster Headache : Leone,
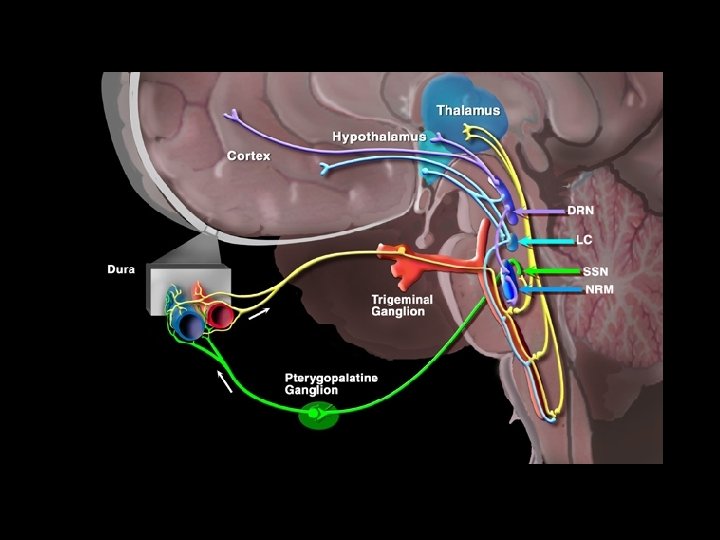

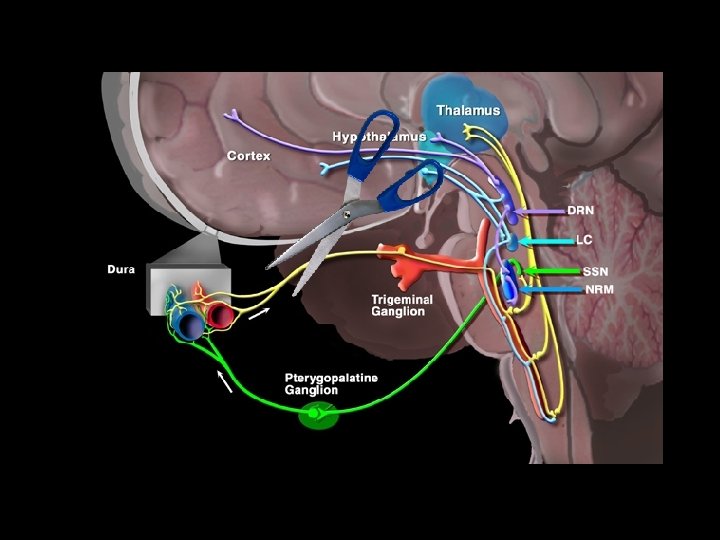
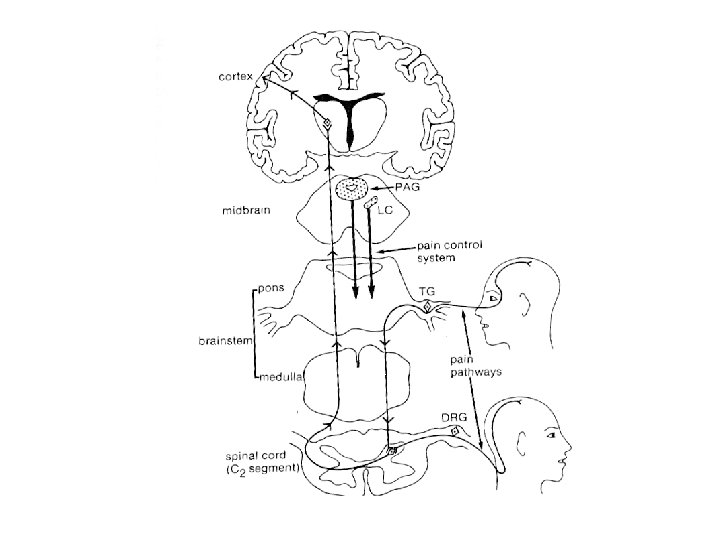
Brainstem Activation in Migraine Headache Weiller et al. Bahra et al. Afridi et al. Nat. Med. 1995 Lancet 2001 Brain 2005

Craniovascular Activation in Primary Headaches Cluster Headache MRA Migraine

Primary Headaches FH Tension-Type headache 3 fold Migraine 50% Cluster headache & related disorders 14 fold Other Primary headaches Anecdotal

Familial Hemiplegic Migraine

Familial Hemiplegic Migraine Pathogenic mutations in three genes → CACNA 1 A, ATP 1 A 2 & SCNA 1 genes 1. FHM 1 – CACNA 1 A gene → P/Q-type voltage-gated neuronal Ca 2+ channels 2. FHM 2 –ATP 1 A 2 gene → Na+ -K+ pump ATPases 3. FHM 3 – SCNA 1 gene → Voltage-gated Na+ channels Genetically predisposed dysfunction of ion-channels within the nervous system

Functional Consequences of Gene Mutations FHM-2 FHM-3 ATP 1 A 2 Gene SCN 1 A Gene Ca Channel Na/K ATPase Pump Na Channel Gain of function Loss of function FHM-1 CACNA 1 A Gene Gain of function Cortical Hyperexcitability

Cortical Spreading Depression in Aura Hadjikhani, Proc Natl Acad Sci U S A, 2001

Genetic Neurological Disorder

Focus on Migraine
 Lipton RB, Stewart WF. Neurology. 1993.")
Migraine Prevalence (5) Lipton RB, Stewart WF. Neurology. 1993.

Normal Prodrome Aura Resolution Normal Headache Appetite Awake/sleep g vin a r C ing wn a Y ed Tir a use a ia N x e or g An nin w Ya y p e Sle Vomiting Deep Sleep Photophobia Phonophobia Osmophobia Smell Fluid balance Tire d Fee Hig ling h/L ow Light tolerance Noise Lim ite tole d food ranc e ed ten n h g i o He cepti r pe Appetite Awake/sleep Light tolerance Noise Smell id Flu Diu resi s tion n e ret Blau, Lancet 1992 Fluid balance

Migraine : Location of Pain • Eye 67 % • Frontal 56 • Temporal 58 • Vertex 24 • Occipital 40 Kelman, Headache 2005 • Neck 40 • Diffuse 18

Aura in Migraine • Visual only • Sensory • Aphasia 99 % 39 54 32 • Visual & sensory • Visual & aphasic • All 3 28 25 6 Eriksen ( Cephalalgia 2004) N=362

Migraine and ‘Headaches’

90% with disabling headache have a Migraine disorder Disabling tension-type headache is rare % Lipton, Headache 2000

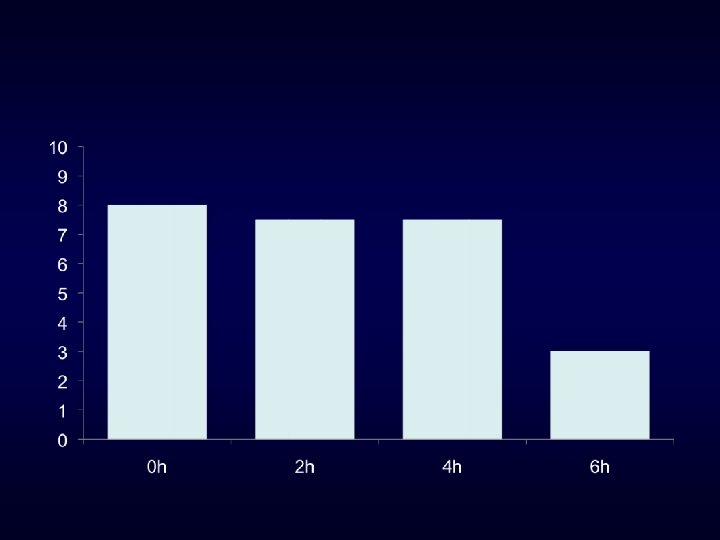
% Response Spectrum Study: Sumatriptan Response

Management of Migraine

Susceptibility to ‘Triggers’ Exogenous Factors • Missed Meal • Too much sleep / too little sleep • Stress / Immediate post-stressful period • Alcohol • Sensory stimuli → Visual and Olfactory • Dietary → Over-estimated • Caffeine and ARM → Under-estimated Endogenous Factors • Hormonal

CHRONIC DAILY HEADACHE % Population Headache > 15 days / month > 3 months 5 USA 4 Other 3 Migraine SPAIN CHINA 2 1 TTH Wang et al. Scher et al. Castillo Neurology 2000 Headache 1998 Headache 1999

% Population Medication-Overuse : 1 -2% 5 USA 4 Other 3 Migraine SPAIN CHINA 2 1 TTH Wang et al. Scher et al. Castillo Neurology 2000 Headache 1998 Headache 1999

Switch from one to the other Caffeine 10 No. subjects with headache Decaffeinated 0 1 6 12 Van Dusseldorp, BMJ. 1990 Week

Switch from one to the other Caffeine 10 No. subjects with headache Decaffeinated 0 1 6 12 Van Dusseldorp, BMJ. 1990 Week
 42% Remission 38% < Frequent 20% CDH Lyngburg, 2005 –")
Prognosis Migraine Prevalence (5) 42% Remission 38% < Frequent 20% CDH Lyngburg, 2005 – Longitiudinal Observation 1989 -2001
 ‘Daily’ headache Medication overuse")
Predictors for Chronic daily headache Older Age Migraine Prevalence (5) ‘Daily’ headache Medication overuse Wang, 2000; Lu, 2001
 ‘Daily’ headache Medication overuse")
Predictors for Chronic daily headache Older Age Migraine Prevalence (5) ‘Daily’ headache Medication overuse Opioids Wang, 2000; Lu, 2001
 ‘Daily’ headache Medication overuse")
Predictors for Chronic daily headache Older Age Migraine Prevalence (5) ‘Daily’ headache Medication overuse Opioids Wang, 2000; Lu, 2001

Management : Acute Attack Treatment Level of effectiveness Side – effects Consistency

Management : Acute Attack Treatment Level of effectiveness → 2 hrs mild / no pain Side – effects → Outweigh benefit Consistency → Adequate dose 3 trials

Management : Acute Attack Treatment Basic Principle: Adequate single abortive dose of the most effective drug Can repeat for recurrence within 24 hours Will not work for initial non-response Maximum use < 6 -8 days / month

Severity Ibuprofen 600 mg TIme

Ibuprofen 600 mg

Sumatriptan 50 mg

Simple Analgesia Abortive dose Aspirin 900 mg po Ibuprofen 400 -800 mg po Naproxen 500 mg po Paracetamol 1 g ANTIEMETIC Domperidone 10 -20 mg po / 30 -60 mg PR Metoclopramide 10 mg po/IM/IV

Efficacy Almotriptan Eletriptan Rizatriptan Side-Effect Profile Almotriptan Frovatriptan Naratriptan Formulation : Rizatriptan Wafer Preference Sumatriptan sc / IN Vomiting Zolmitriptan Wafer / IN Recurrence Almotriptan Eletriptan Naratriptan

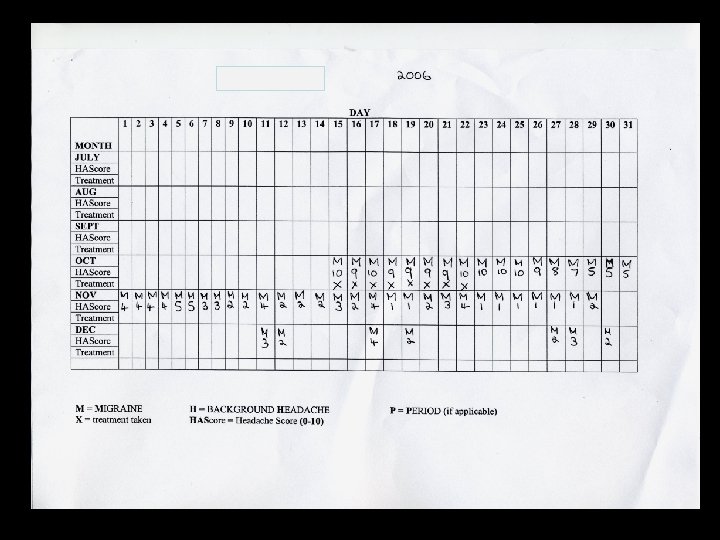
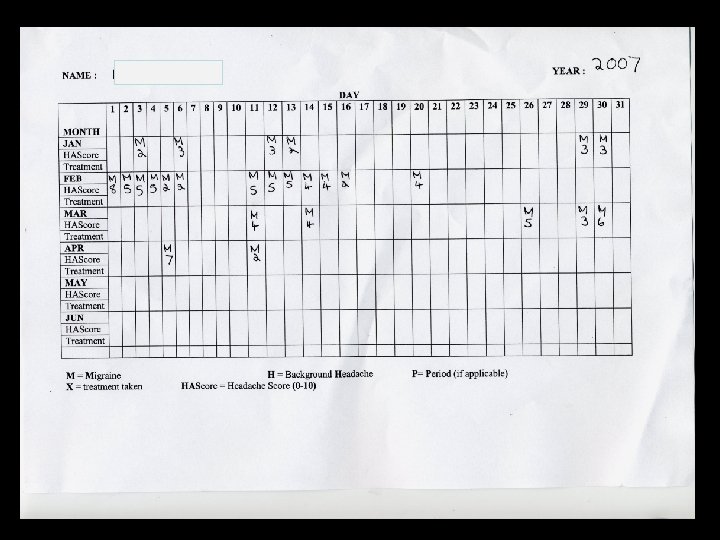
Management • Keep a headache diary • Optimise acute treatment • Frequency < 4 headache days/month → Acute Rx • Frequency > 4 disabling HA days / month → Prevention • Ensure ARM use restricted to < 6 -8 HA days / month • Early introduction of prevention for frequency

PREVENTATIVE START DOSE INCREMENTS MAX DOSES Propranolol* 320 mg Amitriptyline* 200 mg Nortriptyline Pizotifen Start Low Increase Slow Sodium valproate* Gabapentin Topiramate* 150 mg 4. 5 mg 2 g Aim for the Maximum Tolerated (or lower if effective) 3. 6 g 200 mg (can use higher doses)

Severity of Migraine Disorder Propranolol 80 mg bd + 100 mg bd Propranolol 80 mg bd + Topiramate 50 mg bd Propranolol 80 mg bd Propranolol 40 mg bd Propranolol 20 mg bd Time

QUESTIONS Genetic Neurological Disorder
- Slides: 59