Ive got a headache Headache David Kernick Exeter






")


")




 n Tension")

 Secondary")
















 n Primary or secondary (vascular,")










 Risk %")

 Weber 2006 n 93% normal (25% variations of norm) n 6.")










 n Postdrome")
")












 n Peri-menopausal")





 n 10%")





 n 28% nausea and")







- Slides: 99
I’ve got a headache ? ? ? Headache David Kernick Exeter Headache Clinic
Migraine impact n Headache in top 10 of WHO disability index. n 20% population – headache impacts on their quality of life (adults and children) n £ 3 billion per year in economic terms
When people come to see you what do they think they have?
When people come to see you what do they think they have? n Need glasses n Blood pressure n Brain tumour
What do patients have when they present to GP with headache?
What do patients have when they present to GP with headache? Landmark Study n 85% migraine n 10% Tension type headache n 5% secondary headache n <1% other types of headache
What do GPs think when patients present with headache? (Kernick 2008)
Headache consultations in primary care n Consultation rates are low. 50% of migraine sufferers have never seen a doctor n 10% are under continuing care n One third of headaches will be incorrectly diagnosed.
What is happening in primary care? n Less than 20% will receive Triptan Walling 2006 n 10% of those who would benefit from prevention receive it Rahimtoola 2005
Headache referral patterns n 9% GP presentations are referred to secondary care (25% children) (Loughey) n 20 - 30% of neurology referrals are for headache (Hopkins)
What do patients have when they present to A and E with headache? Valade 2000 n – 9480 Average 37 250 admitted (3%)
n Migraine n TTH n Cluster n Trauma n Trig Neuralgia n Sinusitis n Vascular disorders n Low Pressure n Meningitis n Tumour n Other Misc 55% 25% 7% 1. 6% 1. 2% 0. 35% 0. 17% < 5%
Case 1 n 35 year old male n Three week history n Sharp, severe pain bilaterally and posteriorly lasting 10 seconds repetitively. n One question? n Two examinations? n Would you investigate?
Classifying headache
Where does the pain come from? Intra – cranial (dural pain fibres) n Tension – raised intracranial pressure n Compression – tumour n Inflammation - migraine, meningitis, blood
Where does the pain come from? Extra - cranial n Arteritis n Neuralgia n Muscle tension n Facial structures
IHS Headache classification Primary n Migraine n Tension type n Autonomic cephalalgias (cluster) Secondary n n n n Traumatic Vascular Non-vascular (SOL) Substance induced Infection Disturbed homoestasis Facial structures
Activation anywhere in the system can lead to output in any other part of the system and vici versa
Secondary Headaches AURA Thalamus + Mid Brain structures Medication overuse headache Tension type headache Hypothalamus CLUSTER CERVICAL NUCLEI MIGRAINE CENTRE Headache model Primary Headaches
Case 1 n 35 year old male n Three week history n Sharp, severe pain bilaterally and posteriorly lasting 10 seconds repetitively. n One question? n Two examinations? n Would you investigate?
Two examinations n Fundoscopy n BP n iles Elrington neurological examination
Case 1 n 35 year old male n Three week history n Sharp, severe pain bilaterally and posteriorly lasting 10 seconds repetitively. n One question? n Two examinations? n Would you investigate?
Headache Pathway EXCLUDE A SECONDARY HEADACHE n Do something now n Do something soon n DIAGNOSE A PRIMARY HEADACHE n Exclude medication overuse and manage the primary headache
Case 2 You are called out to a 21 year old female who has had severe sudden onset headache. She is lying in a darkened room vomiting and is unable to move. What is the differential diagnosis?
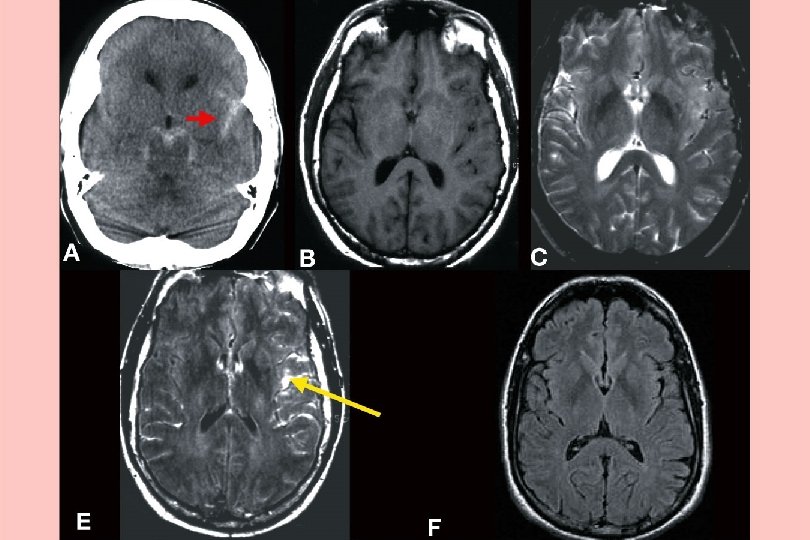
Sub Arachnoid - thunderclap headache
Thunderclap headache - RVS n lasts 1 -3 mths. n Primary or secondary n Normal CT, LP. Needs CT angio. n Can get complications
Meningitis
Malignant hypertension
Migraine - The emergency call out n Injectable sumatriptan n I. M. Diclofenac and anti-emetic n Avoid opiates n Sort out the migraine
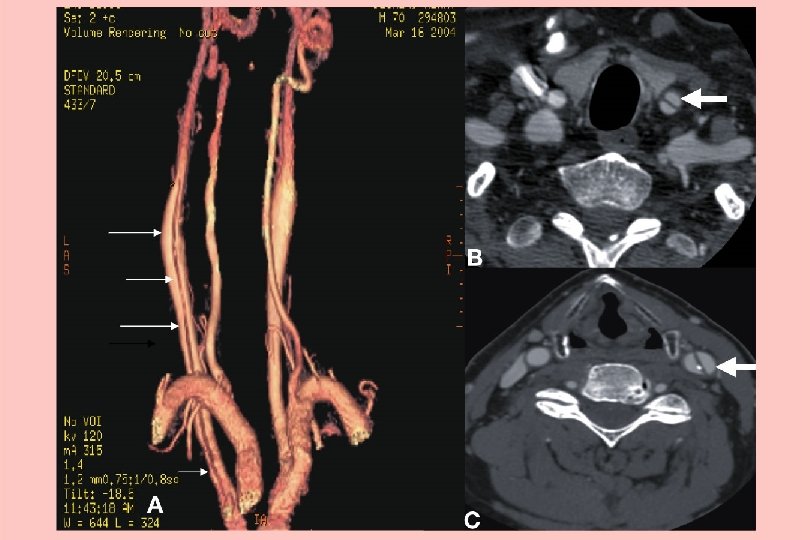
Case 3 n 55 year old male. n New headache. L temporal. Fluctuating in intensity. Featureless. Examination normal. n What would you do?
Temporal arteritis • Can be bilateral • Systemically unwell • Tender artery with allodynia • CRP better than ESR • Problem with skip lesions
CASE 4 • 26 year old pole dancer • Headache with intercourse • What questions would you ask her? • Any investigations? • Treatment?
Sex headache n Pre orgasmic or orgasmic (10% SAH) n Primary or secondary (vascular, tumour, Arnold Chiari) n Low threshold for investigation n Treatment n n Technique B blocker Indometacin Avoid recreational drugs
n Non specific headache n Tinnitus n Two examinations n What is most likely diagnosis?
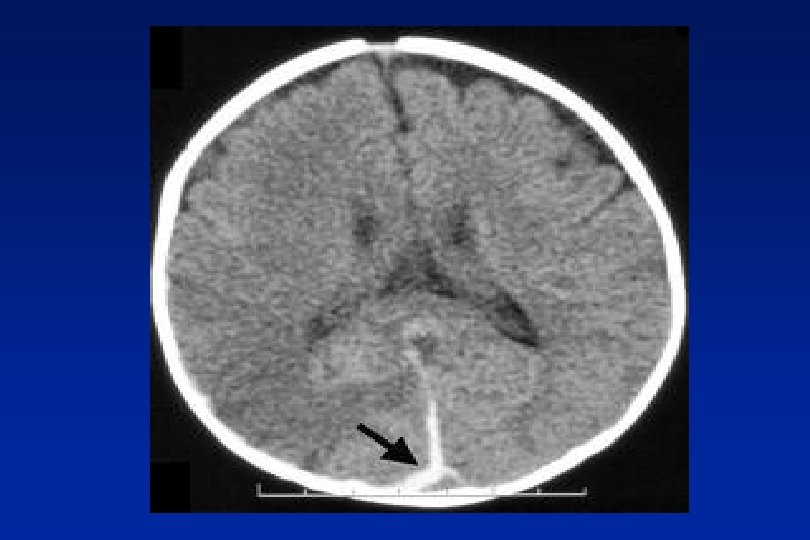
Low Pressure Headache
Case 5 A 34 year old man presents with pain around his left eye that he describes like a “red hot poker”. He has had a number of attacks over the last few weeks. With this presentation, what are the key questions you need to ask him to establish a diagnosis? What investigation will you do?
Cluster - Autonomic Cephalopathy n High impact ++ n Peri-orbital clusters 15 mins - 3 hours n Cluster attacks and periods n Unilateral autonomic features n Acute or chronic
Cluster treatment n Injectable Sumatriptan n Nasal Zolmitriptan n Short term steroids n Oxygen 100% n Verapamil
CASE 6 n 45 year old female n Dull continuous bilateral occipital pain n Featureless n Worried as friend had brain tumour and wants a scan n Three questions? n Do you investigate?
n Have you ever had migraine? n Do you have problems with your neck? n What pain killers are you taking? n To scan or not to scan?
Medication overuse headache Headache intensity Withdrawal of all analgesia Increased frequency of headache, associated with increased frequency of analgesia use. Daily headache with spikes of more severe pain Migraine attacks Frequent ‘daily’ headaches Return of episodic headache
Primary Tumours n Meningioma 20% - 10 yr survival 80% n Glioma 70% - 5 yr survival 20% n Misc. 10% - Variable
Headache and tumour n Headache prevalence with tumour 70%+ n Headache at presentation 50% n Headache alone at presentation 10% (Iverson 1987)
Risk of brain tumour with headache presenting to primary care (Kernick 2008) Risk % Undifferentiated headache Primary headache Under 50 0. 09% 0. 03% Over 50 0. 28% 0. 09%
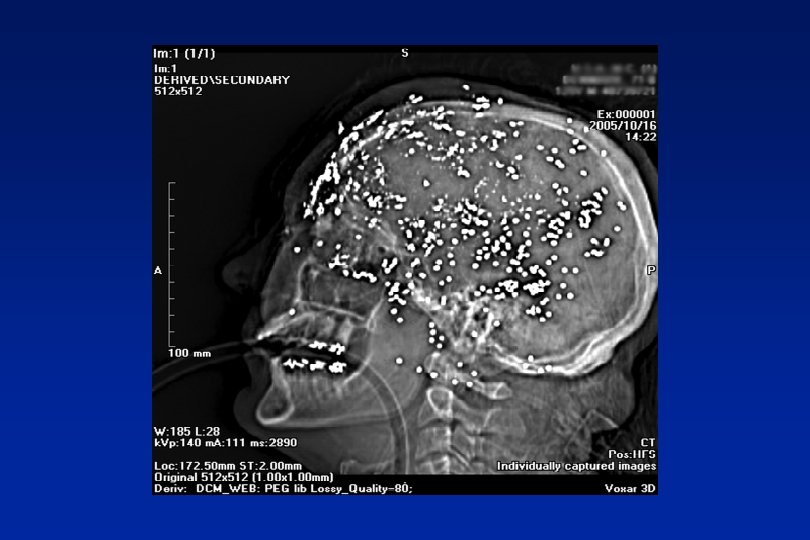
We need to scan when the advantages out way the disadvantages Reassurance, Diagnosis/treatment Cost, exposure incidental pathology (4 -10%)
Luftwaffe pilots (n-2370) Weber 2006 n 93% normal (25% variations of norm) n 6. 7% abnormalities n 56 cysts; 13 vascular abnormalities; 4 adenomas; 4 tumours
In reality the inputs are complex n Limited poor quality evidence base n Expert opinion n Medico-legal case law n Patient-doctor characteristics and approach to uncertainty n Organisational factors
Red Flags Probability of significant morbidity or mortality >1%. Need urgent investigation n Abnormal neurological symptoms or signs n New seizure n History of cancer elsewhere
Orange Flags Headache presentations where probability is likely to be 0. 1% and 1%. Need careful monitoring and low threshold for imaging n Aggregated by Valsalva manoeuvre n Headache with significant change in character n Awakes from sleep n New headache over 50 years n Memory loss n Personality change
The delivery of headache services
Secondary Care “The role of the specialist is to reduce uncertainty, to explore possibility and to marginalise error. Primary Care “The role of the GP is to accept uncertainly, to explore probability and to marginalise danger”.
GPs with special interest n NHS plan calls for GPSIs to provide local, efficient care n Controversy over concept from primary care n Limited evidence base n Substitution, complementation, meeting unmet need
Commissioning headache service delivery BASH 2001, ABN 2010 n GPs first line management n GPSI support n Tertiary headache centres
CASE 7 n Jane is a 28 yr old n Presents with a visual disturbance lasting 30 minutes. No other symptoms n What are the key questions? n What is the differential diagnosis
Secondary Headaches AURA Thalamus + Mid Brain structures Medication overuse headache Tension type headache Hypothalamus CLUSTER CERVICAL NUCLEI MIGRAINE CENTRE Headache model Primary Headaches
CASE 7 a n Jane develops a pattern of visual disturbance followed by headache n What features would confirm a diagnosis of migraine? n How would you manage the acute attack?
Migraine n Prodrome 60% n Aura 30 % n Headache (30% bilateral) n Postdrome
Formal Migraine n At least 5 attacks n 4 -72 hours (1 -72 hours) n Two of : unilateral, pulsating, moderate or severe pain, aggregation by physical activity. (bilateral) n At least one of: nausea/vomiting, photophobia, phonophobia. (Can be inferred) n Not attributed to another disorder.
In practice n Recurrent headache that bothers n Nausea with headache n Light bothers
Implications for gastric stasis and neck pain
Migraine Acute treatment n Paracetamol, Aspirin, Domperidone. n Triptan
Triptans
Triptan Half Life
Triptans – some practical points n Treat early n Failure not class effect n Not in CVD n SSRIs n Over 65 years
CASE 7 b n Jane’s headaches become more frequent. When would you instigate prevention? n What is your first choice?
Migraine treatment Preventative n When to instigate? n What to use? n How long for to assess an effect? n What rate dose increase? n How long on preventative medication?
Migraine prevention +- evidence and licence • • • Beta blocker Pizotifen Amitriptyline Gabapentin Sodium valproate Topiramate Calcium antagonists Lisinopril, Montelukast Clonidine Methylsergide ++ (L) + - (L) + + ++ +++ (L) ++--++(L)
CASE 7 c n Jane has come for contraceptive advice. n What options does she have?
What about the pill? Ischaemic stroke n Fit women - 5/100, 000 women years n Without aura - 15/100, 000 women years n With aura - 30/100, 000 women years n Avoid if other risk factors Eg smoking n ? POP - probably safe
CASE 7 d n After a few years, the migraines have settled to monthly and associated with menstruation only. She is fed up with taking regular prevention. n How will you manage this?
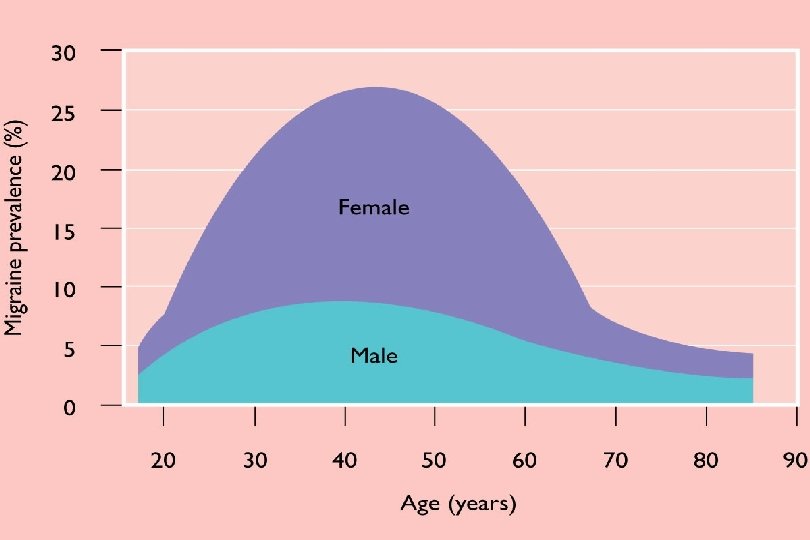
Oestrogen sensitive migraine n Menstrual (pure - 7%, and other times 35%) n Peri-menopausal
Menstrual Migraine n Tricycle OC n Regular NSAI n 100 mcg oestrogen patch n Regular long acting Triptan
Peri-menopausal migraine n Too much oestrogen too quickly - worse n 25 mcg Evoral patch in quarters n Avoid oral oestrogen n Reassure will get better
CASE 8 Jane brings in her 13 year old son who is getting trouble with headache. In view of the family history you suspect migraine. n How do features in children differ from adults? n Would you image? n What treatment would you instigate?
Headache A complex biopsychosocial interaction
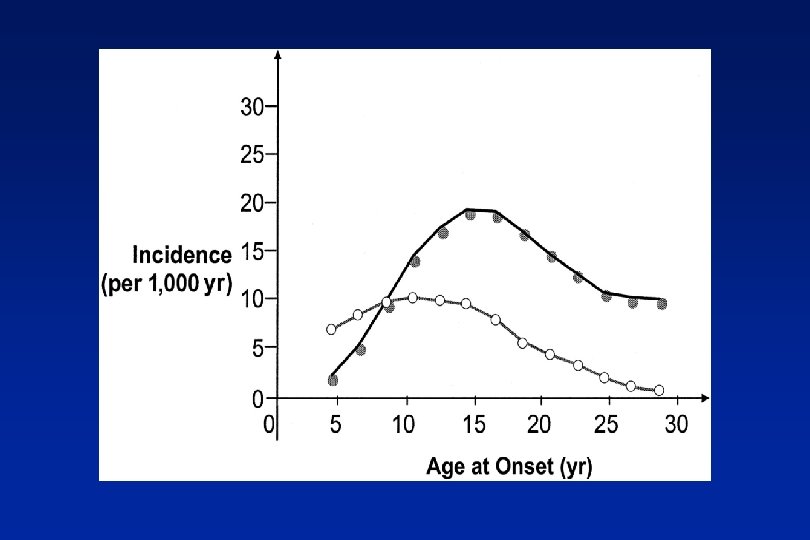
Primary Headache Epidemiology n Headache most frequent neurological problem in children and commonest manifestation of pain n 50% Childhood migraine becomes chronic and continues into adulthood n n <10% will see their GP
Primary Headache Epidemiology n 10. 6% migraine prevalence (3. 4% age 5) n 10% -24% tension type prevalence n 0. 01% cluster prevalence n Invariably mixed or not well defined
Why don’t children seek help? Mortimer 1992 n Don’t realise its migraine n Only a headache n Parents don’t want to reinforce illness behaviour n Parents pattern their health seeking behaviour
What is happening in primary care? Kernick Cephalalgia 2009 n GPs made diagnosis in 20% n 25% referred to secondary care n 3 in 10, 000 tumour n No tumours if migraine diagnosed
Diagnosis Depression Total in cases 1. 5% Total in controls 0. 67% LR (confidence intervals) 2. 2 (1. 9, 2. 5) Depression in year after headache presentation
Problems with Children under 3 years n Unable to articulate symptoms of raised intracranial pressure n Problem may be suggested by their behaviour in ways that may be relatively subtle
Features childhood migraine n Pain is shorter acting n More likely to be bilateral n Often “mixed” n Associated with other systemic presentations
Presentation of Brain Tumour n 40% headache (<10% headache alone) n 28% nausea and vomiting n 22% motor abnormalities n 17% visual abnormalities n 17% cranial nerve abnormalities n 10% seizures n 3% behavioural change Wilme 2010
Red Flags Discuss with Paediatrician the same day n n n Abnormal neurological sign Confusion or disorientation Visual abnormalities Abnormal head position (double vision or neck pain) Cerebella dysfunction Persistent headache for 4 or more weeks at presentation that awake from sleep or occur on waking n Persistent headache at any time in a child younger than 4 years n Persistent headache for 2 or more weeks with vomiting
Orange Flag presentations Need referral/close monitoring n Headache with behavioural change n Headache with deterioration in school work n Headache with growth arrest or abnormal puberty n A persistent unilateral or occipital headache n A persistent headache in a child with a personal or family history of childhood tumour n Recent change in headache characteristics in a previous diagnosed primary headache
Management n Avoidence of triggers n Analgesia +-Domperidone n Sumatriptan nasal n Pizotifen n Propranolol n Amitrip n Topiramate
School Policy Guidelines. RCGP, Headache UK, RCN
Diagnosing the right headache Three Key Questions 1 - What is the impact? n Migraine - lie down n Tension Type Headache - keep going n Cluster Headache - bang head against wall
Diagnosing the right headache Three Key Questions 2 - How many types of headache do you recognise?
Diagnosing the right headache Three Key Questions 3 - What pain killers are you taking?