ENDOMETRIAL CARCINOMA UPDATES Dr Marco Matos Gold Coast



![Obesity significantly increases the risk of developing cancers including endometrial cancer [TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-4.jpg "Obesity significantly increases the risk of developing cancers including endometrial cancer [TITLE]")
![In 2020, more than 70% of the population of Australia will be overweight [TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-5.jpg "In 2020, more than 70% of the population of Australia will be overweight [TITLE]")
![[TITLE] Non endometrioid (serous, clear cell carcinoma) cancers disproportional contribute to deaths in comparison](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-6.jpg "[TITLE] Non endometrioid (serous, clear cell carcinoma) cancers disproportional contribute to deaths in comparison")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-7.jpg "[TITLE]")

![Carcinogenesis model of type II endometrial cancer: P 53 mutation an early event [TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-9.jpg "Carcinogenesis model of type II endometrial cancer: P 53 mutation an early event [TITLE]")

![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-12.jpg "[TITLE]")















![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-33.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-34.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-35.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-36.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-37.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-38.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-39.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-40.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-41.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-42.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-43.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-44.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-45.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-46.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-47.jpg "[TITLE]")
![[TITLE]](https://slidetodoc.com/presentation_image_h/ed1ec2e59fe1b336d5cf9b41e7bbc8b8/image-48.jpg "[TITLE]")
- Slides: 48
ENDOMETRIAL CARCINOMA UPDATES Dr Marco Matos Gold Coast Cancer Care, Gold Coast University Hospital and Pacific Private Oncology Group
USA. Uterine cancer: new cases and dates ● 1990 33000 4000 ● 2000 36100 6500 ● 2010 43470 7950 ● Ovarian cancer 21880 new cases and 13850 deaths ● Cervical cancer: 12200 new cases and 4210 deaths
● ● In Australia endometrial cancer affects 1 in 69 women before the age of 75. In 2010, 2100 women were diagnosed. 6 /day ● 370 expected deaths a year ● The incidence is increasing
Obesity significantly increases the risk of developing cancers including endometrial cancer [TITLE]
In 2020, more than 70% of the population of Australia will be overweight [TITLE]
[TITLE] Non endometrioid (serous, clear cell carcinoma) cancers disproportional contribute to deaths in comparison with endometrioid histology
[TITLE]
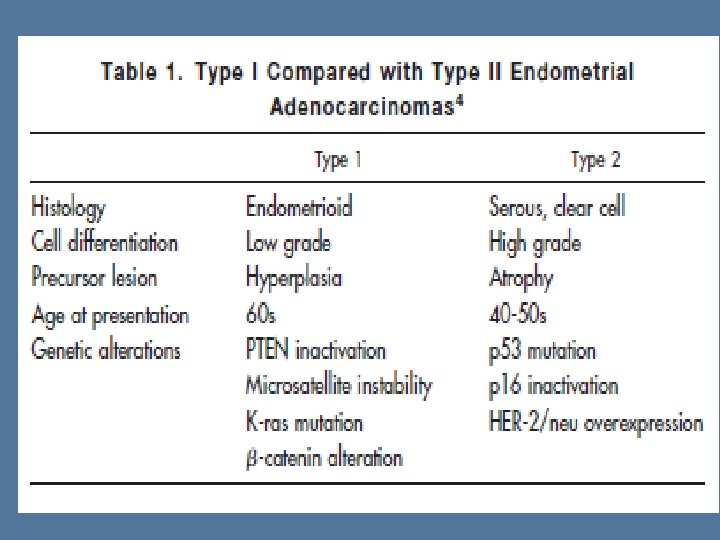
Carcinogenesis model of type I endometrial cancer: PTEN, MSI and Kras alterations playing an earlier important role. P 53 mutations a late event [TITLE]
Carcinogenesis model of type II endometrial cancer: P 53 mutation an early event [TITLE]
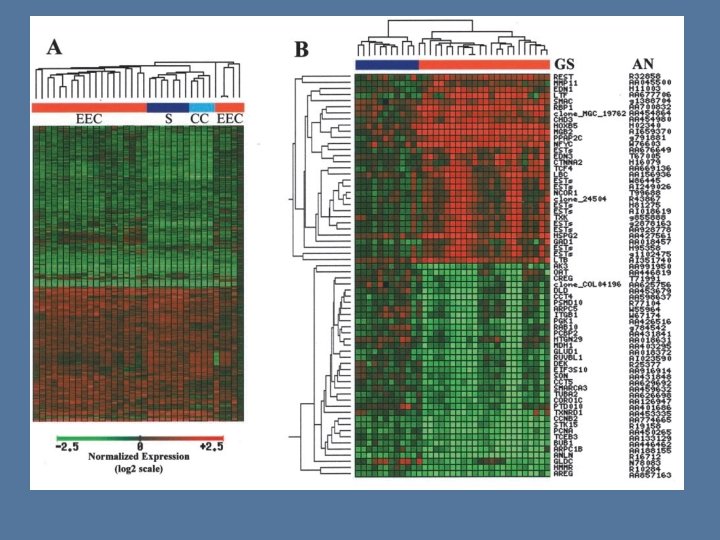
Molecular alterations differ in Type 1 vs type 2 endometrial cancers ● ● Endometrioid adenocarcinoma (Type 1) – PTEN loss of function (up to 60%) – PI 3 KCA mutation (30%) – K ras mutation (10 - 20%) – FGFR 2 mutations (12 - 16%) – Microsatelalite instability (20 – 45%) – Nuclear accumulation of b- cadherin (18 – 47%) Papillary Serous (Type 2) – P 53 mutations (90%)
[TITLE]
MANAGEMENT
Survival improves in the hands of a trained Gynae-oncologist
Hormonal therapy of endometrial cancer Agent Tumour grade Number RR % Medroxyprogesterone 800 mg/d Podratz 1985 1 2 3 14 17 27 40 15 2 Tamoxifen 40 mg/d alternating with medroxyprogesterone 200 mg/d Whitney 2003 1 2 3 15 17 27 33 Medroxyprogesterone 160 mg/d x 3 weeks then Tamoxifen 40 mg /d x 3 weeks Fiorica 2003 1 2 3 16 17 22 38 24 22
Response rates and survival to single agent chemotherapy AGENT Prior treatment Number RR% Prob PFS (>6 mo) OS months 25 0 0. 08 8. 7 48 25 0. 21 8. 9 Caelyx 43 9 0. 23 8. 2 Topotecan 28 7 0. 25 9 Oxaliplatin 52 13 0, 27 10. 9 27 8 0. 11 6. 4 27 4 0. 28 9. 4 50 12 0. 20 8. 7 Etoposide Paclitaxel Docetaxel No 77% prior Rx Pemetrexed Ixabepilone 94% prior Rx
Biological agents: response rate and PFS Agent N RR % Prob Clinical (PFS> 6 mo) Benefit Ratio (CR + PR +SD) Duration of stability (median months) TKI and VEGF inhibitors Gefitinib 29 3. 8 0. 15 Lapatinib 30 3. 3 0. 10 Bevacizumab 52 13. 5 0. 40 Temsirolimus 18 25 82 6. 7 Temsirolimus 27 7 51 3. 8 Deferolimus 45 7 33 <4 Everolimus 35 0 43 4. 5 MTOR inhibitors
LET’S LOOK AT THE DATA:
GOG 30 Adryamicin in advanced / recurrent endometrial cancer ● Adryamicin 60 mg/m 2 ● N = 43 ● CR= 26 % + PR= 12% = 37% ● Better survival for responders, p<. 05 ● Active agent
GOG 34 Phase III, surgery + radiotherapy +Doxorubicin in stage IC, II and IIIA EC ● Doxo 60 mg/m 2 q 3 /52 up to 500 mg ● No G 3 – 4 cardio toxicity ● Survival 60 vs 66%, p= NS ● “Unable to determine effect” ● Morrow et al Gyn Onc 36: 166, 1990
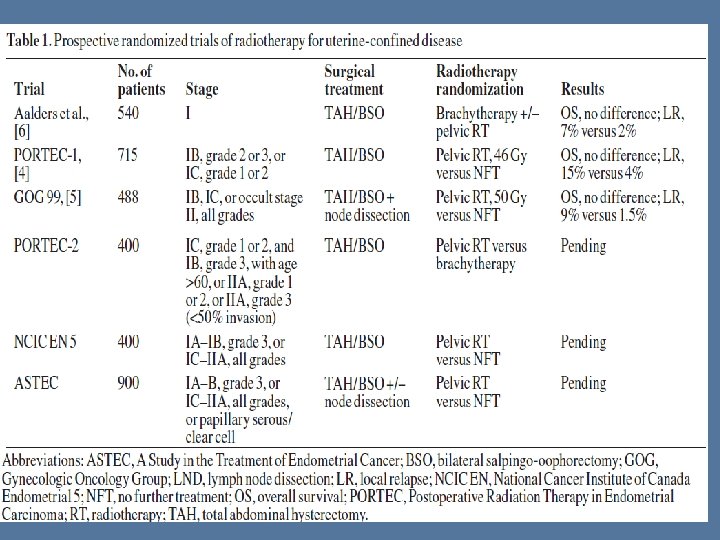
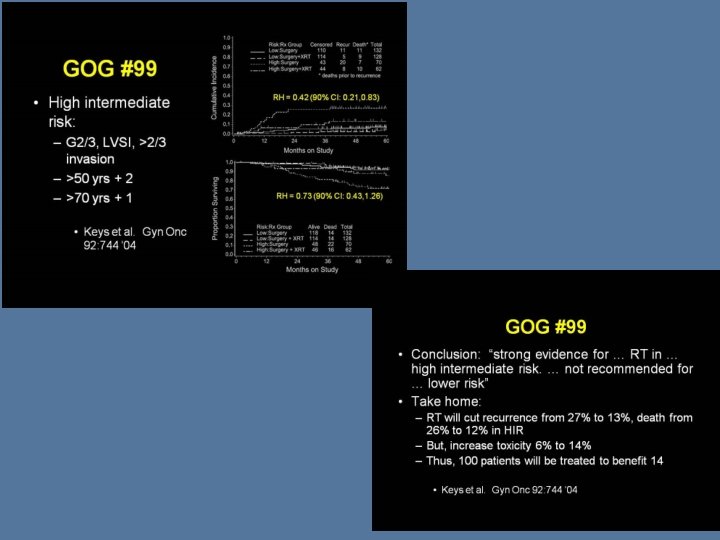
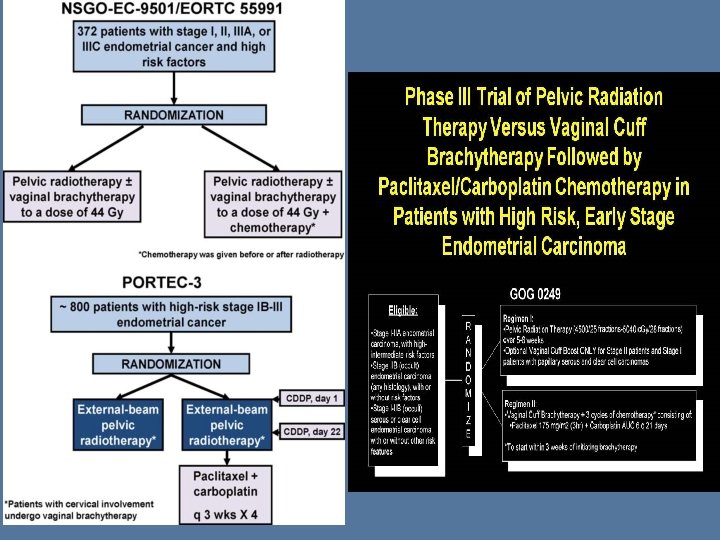
GOG 99 Surgery +- adjuvant radiotherapy
GOG 107 phase III trial, doxorubicin +- cisplatin in stage III/ IV EC ● Doxo 60 +- CDDP 50 mg/m 2 q 3/52 ● N= 281 ● ● G 3 -4 leucopenia (62 vs 40%), anaemia (22 vs 4%), N/V (13 vs 4%) Dox; CR 8%+ PR 17%= 25%, PFS 3. 9 mo, OS 9 mo Dox + CDDP; CR 19% + PR 23% = 42%, PFS 5. 7 mo , OS 9. 2 mo Adding cisplatin improves RR and PFS but not OS at the cost of more toxicity
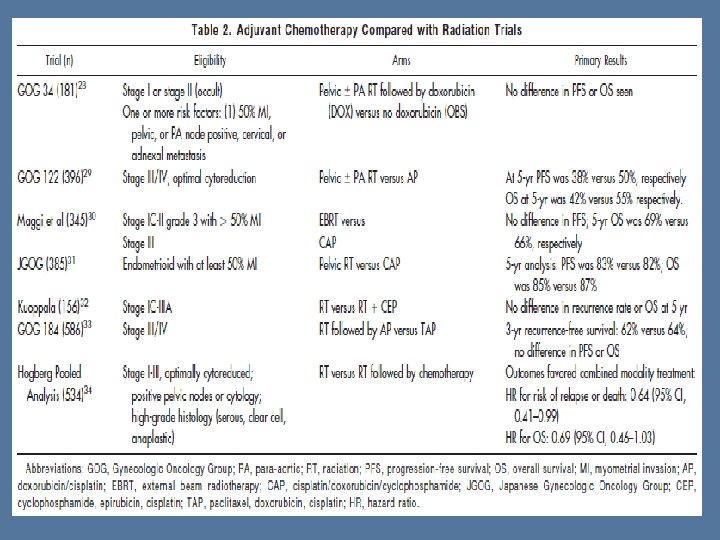
GOG 122 Adjuvant Radiotherapy vs AP
● Adverse events were more common with AP ● At 24 mo: p<0. 01: – DFS: WART 46 vs AP 59%, OS: WART 59% vs AP 70%
GOG 177 RR: 57 VS 34%, PFS 8. 3 vs 5. 3, m. OS 15. 3 vs 12. 3 mo all in favour of TAP but at increased neurotoxicity
GOG 184
OTHER UPDATES
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]