Abnormal Uterine Bleeding Anisa SsengobaUbogu M D BCM

Abnormal Uterine Bleeding Anisa Ssengoba-Ubogu, M. D. BCM Kelsey- Seybold Clinic Family Medicine Residency Program

Goals l Review causes of Abnormal uterine bleeding l Management

l Menstrual disorders accounted for 19. 1% of 20. 1 million visits to physician offices for gynecologic conditions over a two-year period l 25% of gynecologic surgeries involve abnormal uterine bleeding

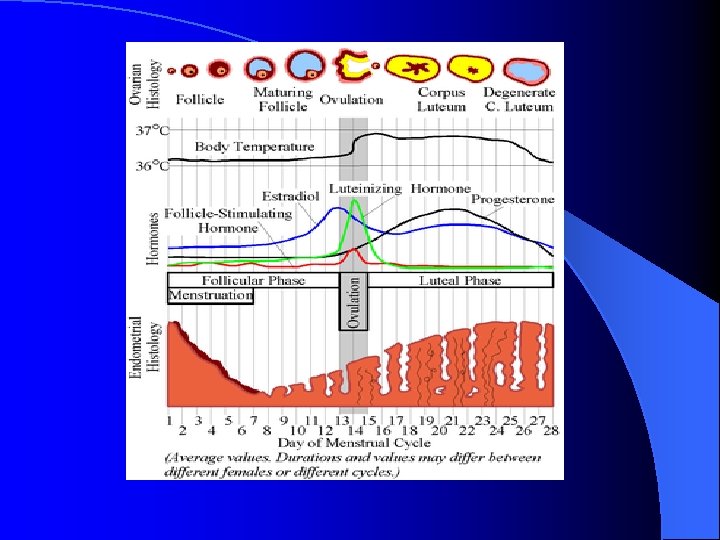
l NORMAL MENSTRUAL CYCLES OCCUR AT 28 DAY INTERVALS l 21 -35 DAY RANGE IS NORMAL l 400 -500 CYCLES OCCUR BETWEEN THE FIRST AND LAST PERIODS l 70% OF THE BLOOD LOSS FROM A MENSTRUAL CYCLE OCCURS IN THE FIRST TWO DAYS
 but with heavy")
l Menorrhagia- Bleeding occurs at normal intervals (21 to 35 days) but with heavy flow (>=80 m. L) or duration (>=7 days l Metrorrhagia-Irregular, frequent uterine bleeding of varying amounts but not excessive l Menometrorrhagia-Bleeding occurs at irregular, noncyclic intervals and with heavy flow (>=80 m. L) or duration (>=7 days).

l Polymenorrhea-Regular bleeding at intervals of less than 21 days l Oligomenorrhea-Bleeding at intervals greater than every 35 days l Amenorrhea-No uterine bleeding for at least 6 months l Acute emergent abnormal uterine bleeding - significant blood loss that results in hypovolemia (hypotension or tachycardia) or shock.

Differential Diagnosis l Medications l Systemic Disease l Infection l Trauma l Complications of Pregnancy l Benign Pelvic Pathology l Neoplasm

Medications/iatrogenic l l l Anticoagulants Antipsychotics Corticosteroids Herbal and other supplements: ginseng, ginkgo, soy Hormone replacement Intrauterine devices OCPs, including progestin-only pill l SSRI’s l Tamoxifen (Nolvadex) l Thyroid hormone replacement l

Systemic disease l l l l l Blood dyscrasias, including leukemia and thrombocytopenia Coagulopathies Hepatic disease Polycystic ovary syndrome Renal disease Adrenal hyperplasia and Cushing's disease Hypothalamic suppression (from stress, weight loss, excessive exercise) Pituitary adenoma or hyperprolactinemia Thyroid disease

l

Infection l Cervicitis l Endometritis l Myometritis l Salpingitis

Trauma l Laceration l Abrasion l Foreign body l Sexual Abuse/ Assault

Complications of Pregnancy l Intrauterine pregnancy l Ectopic pregnancy l Spontaneous abortion l Gestational trophoblastic disease l Placenta previa

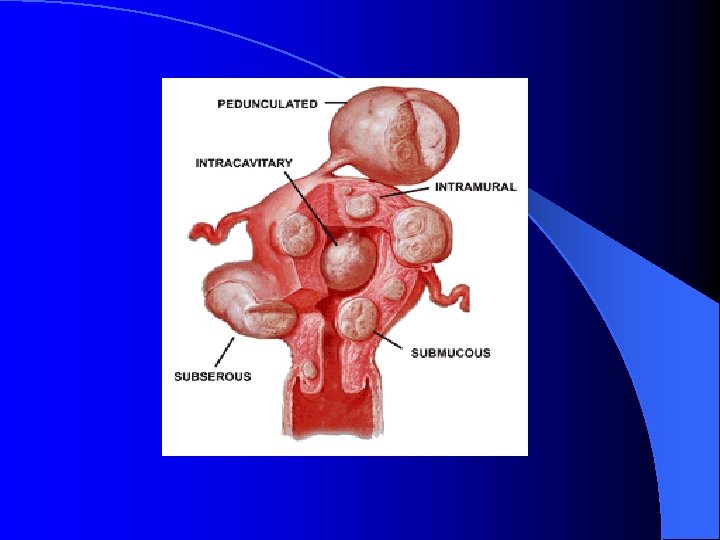
Benign pelvic pathology l Cervical polyp l Endometrial polyp l Leiomyoma l Adenomyosis

Endocervical polyp

Endometrial Polyp

Leiomyoma


Malignant neoplasm l cervical squamous cell carcinoma l endometrial adenocarcinoma l estrogen-producing ovarian tumors l testosterone-producing ovarian tumors l leiomyosarcoma l 1 IN 5 WOMEN OLDER THAN 45 WILL HAVE A MALIGNANT OR PREMALIGNANT CAUSE OF BLEEDING

Endometrial Cancer

Risk Factors for Endometrial Cancer l l l l Chronic anovulatory cycles Obesity Nulliparity Age > 35 years Diabetes Tamoxifen therapy H/o unopposed estrogen use

Labs l Pregnancy l l l l test! Cbc- access anemia/ platelet dysfunction STD check (GC/CT/trich) PAP LFT’S/INR TSH Prolactin Blood glucose DHEA-S, free testosterone, 17 alphahydroxyprogesterone

Imaging/ tissue sampling l EMB l TVUS l Saline-infusion l Hysteroscopy sonohysterography

Bleeding pattern l Severe acute l Ovulatory l Anovulatory l Related to contraception

Severe Acute Bleeding l Premarin 2. 5 mg qid plus promethazine 25 mg l D &C if no response after 2 -4 doses of Premarin l Switch to OCP (Lo. Oval qid x 4 d, tid x 3 d, bid x 2 d, qd x 3 wks, 1 wk off then cycle for 3 mo

Dysfunctional Uterine Bleeding l Abnormal uterine bleeding not caused by pelvic pathology, medications, systemic disease or pregnancy. l Can be ovulatory or anovulatory.

Causes of DUB l Estrogen breakthrough bleeding l Estrogen withdrawal bleeding l Progesterone breakthrough bleeding

Medical Management l Anovulatory- OCP’s/patch/ring or cyclic progestins if contraindication to OCP’s NSAIDS, levonorgestrelreleasing intrauterine system (Mirena) OCPs, Depo, patch, ring, Implanon l Ovulatory-

Ortho Evra

Mirena Nuva Ring Implanon

Abnormal bleeding w/ OCPs l Low dose OCPs – increase estrogen Necon 1/35, Demulen 1/50, Lo. Ovral l -check STDs l - imaging

Abnormal Bleeding with Depo l 1 st 4 -6 mo? Observe, add OCP, inc injection freq q 2 mo l Premarin recurs 1. 25 mg qd x 7 d, repeat if bleeding OTHER OPTIONS: -Ethinyl estradiol (Estinyl)- 20 mcg per day for 1 to 2 weeks –Estradiol (Estrase)- 0. 5 to 1 mg per day for 1 to 2 weeks

Abnormal Bleeding with IUD l Observe if mild for 4 -6 mo l OCP for one cycle if Mirena l Provera 10 mg for 7 days if Paraguard

Surgical Management l Hysterectomy l Uterine artery embolization l Endometrial ablation l Myomectomy l Operative hysteroscopy

Case #1 l 18 year old female h/o Depo x 4 years, complains of heavy bleeding and cramping l (give estradiol 1 mg daily x 2 wks, Motrin, check cbc, calcium+D, consider other birth ctl options)

Case #2 l 25 year old female with complaint of heavy menses lasting 10 days+ dysmennorhea, hct 30. l (regulate with birth ctl, tx anemia, NSAIDS)

Case #3 l 59 year old widowed female with 2 episodes of spotting. l (check cultures, refer to Gyn)

Case #4 l 30 year old female complains of lack of menses for 3 months l (trial of Provera 10 mg daily x 10 days for withdrawal bleeding)

Case #5 l 19 y/o female with severe bleeding, 1 tampon/hr. BP stable. l (Premarin OCP) 2. 5 qid with antiemetic, then
- Slides: 41