Dr Haroon urRashid Assistant Professor Radiotherapy Oncology Sargodha

")


 starts in the colon or rectum CRC is the")


 Sporadic (average risk) (75 -80%) Rare syndromes (<0. 1%) Familial adenomatous")

 • Racial, ethnic factors –")



















 1998")
 Cetuximab")
















 · Flexible Sigmoidoscopy every 5")

 chemical test for blood in a")

- Slides: 58
Dr Haroon –ur-Rashid Assistant Professor Radiotherapy/ Oncology Sargodha Medical College
Colorectal cancer (CRC)
Today we will discuss… Understanding colon and rectum cancer Partnering with your medical team Making treatment decisions Managing side effects Screening and early detection Coping with life after treatment
Lung/bronchus 88, 629 Prostate 28, 590 Men 285, 900 Women 270, 600 67, 650 Lung/bronchus 40, 590 Breast Colon & rectum 28, 590 29, 766 Colon & rectum Pancreas 14, 295 16, 236 Pancreas Non-Hodgkin lymphoma 11, 436 13, 530 Ovary Leukemia 11, 436 10, 824 Non-Hodgkin lymphoma Esophagus 11, 436 10, 824 Leukemia Liver/intrahepatic 8, 577 bile duct Urinary bladder 8, 577 Kidney 8, 577 All other sites 62, 898 8, 118 Uterine corpus 5, 412 Brain/ONS 5, 412 Multiple myeloma 62, 238 All other sites ONS=Other nervous system. *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2003.
Understanding CRC Colorectal cancer (CRC) starts in the colon or rectum CRC is the 3 rd most common form of cancer diagnosed in men and women in the US (148, 000 new cases in 2010) CRC is the 2 nd leading cause of cancer deaths in the US. (48, 000 deaths in 2010) The number of people dying from CRC has declined over the past 20 years with better screening, diagnosis and treatments Screening for/removing polyps early is the best way to prevent and cure CRC
Signs and Symptoms could include: A change in bowel movements (diarrhea, constipation, never feeling “relieved”, narrower stools) Blood in the stool (dark red) Abdominal discomfort Loss of appetite Weight loss for no known reason Constant fatigue Nausea and vomiting Many people have no symptoms - encourage those close to you to get screened
Colorectal Cancer ¤ 80% present with early disease ¤ 20% present with metastatic disease. Stage at Diagnosis Distant (Stage IV) 20% ¤ Among patients diagnosed with early-stage disease, 40% will suffer recurrence. Regional (Stage III) 30% Localized (Stage I/II) 50%
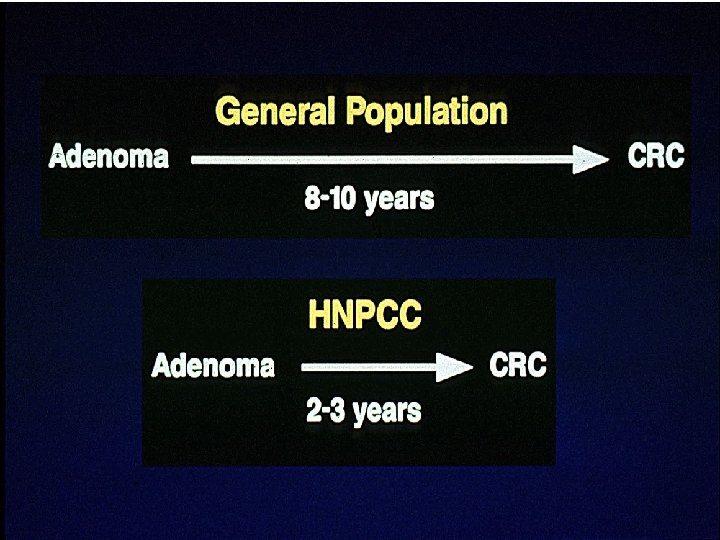
Colorectal Cancer (CRC) Sporadic (average risk) (75 -80%) Rare syndromes (<0. 1%) Familial adenomatous polyposis (FAP) (1 -2%) Family history (10 -15%) Hereditary non-polyposis colorectal cancer (HNPCC) (3 -5%)
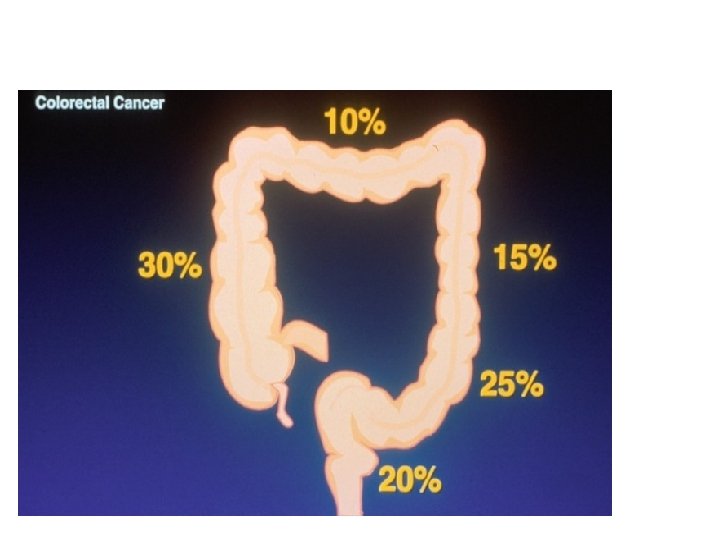
common sites of incidence & symptoms of colon cancer
Risk Factors for CRC • Age >50 (average risk) • Racial, ethnic factors – African-Americans have increased risk • Dietary factors – high animal fat, low fiber diet • Lifestyle – Sedentary – Obesity – Smoking – Alcohol
Risk Factors for CRC • Family or personal history of CRC • HNPCC – Lynch syndrome I, II • Polyposis syndromes – FAP, Gardner’s syndrome, Turcot’s syndrome, juvenile polyposis • Inflammatory bowel disease – chronic ulcerative colitis, Crohn’s disease
Lifestyle Risk Factors for Colorectal Cancer · Decrease Risk - Exercise Folic acid Aspirin Calcium, vitamin D Screening · Increase Risk - Obesity Red meat Alcohol Smoking
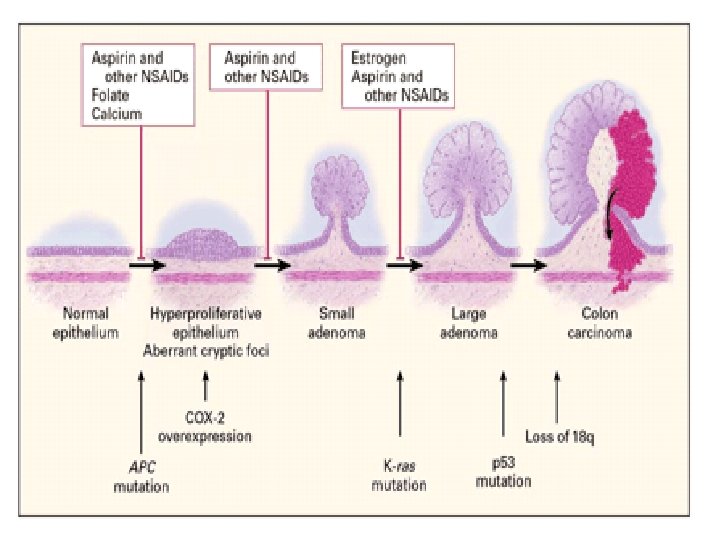
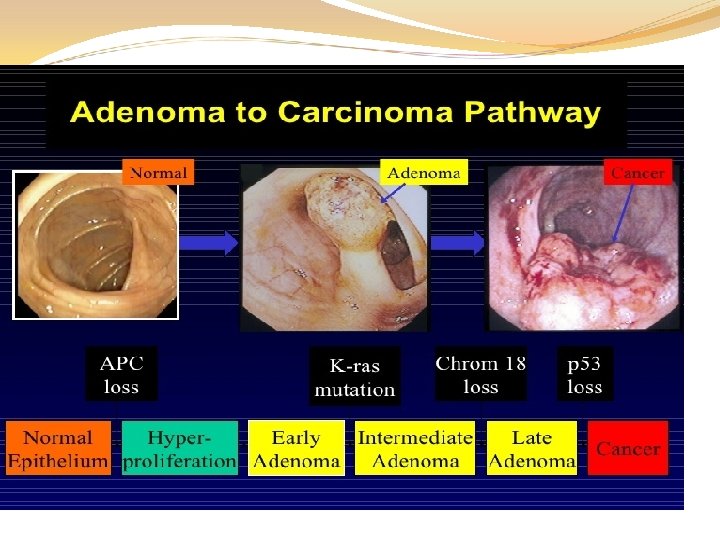
Natural History Polyp Advanced cancer • Age 50, 25% risk of developing polyps • Age 75, 50 -75% risk of developing polyps
Diagnosing CRC A colonoscopy looks at the entire colon to identify problems Blood tests help to categorize your overall health a CEA test is often used to follow the presence of CRC Imaging tests will identify if cancer exists in other parts of your body CT scan, MRI, PET scan Surgery will remove tumor(s), tissue and lymph nodes which will be tested by a pathologist to determine the type and stage of cancer present
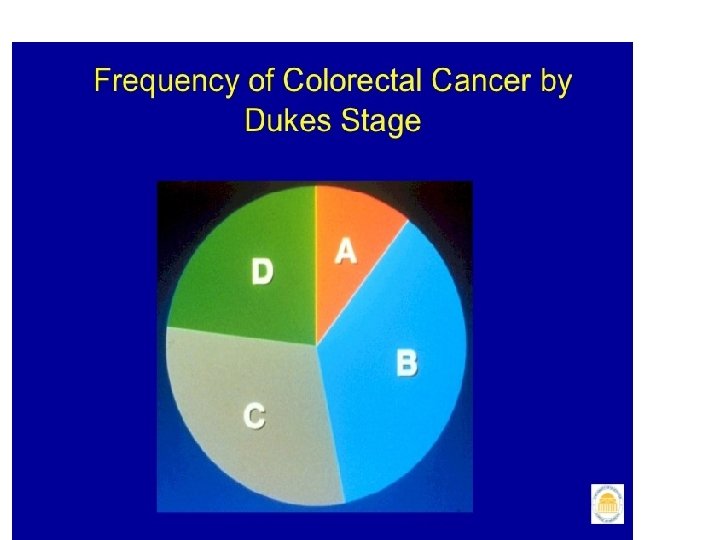
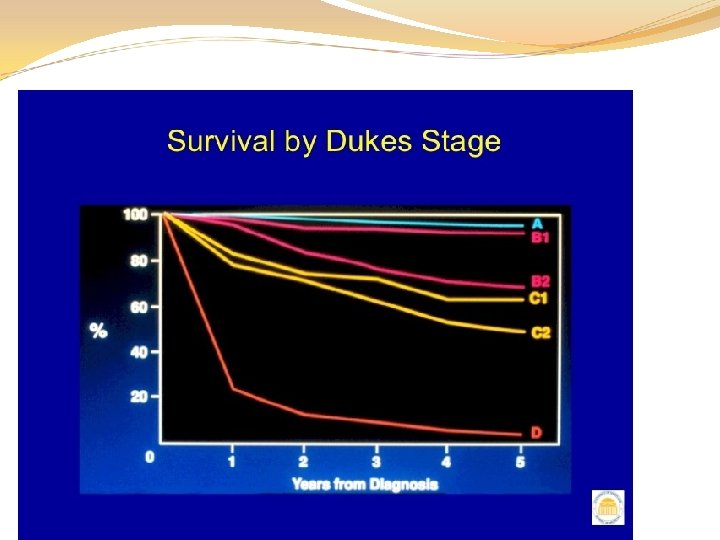
Staging of CRC Dukes staging system A B C 1 C 2 D Mucosa Into or through M. propria Into M. propria, + LN ! Through M. propria, + LN! distant metastatic spread 80% 50% 40% 12% <5%
Staging of Colorectal Cancer Stage Extent of tumor 5 -year survival Mucosa Muscularis mucosa Submucosa Muscularis propria Serosa Fat Lymph nodes C 2 C 1 A Not throug Through No deeper B 1 B 2 D bowel wall: than lymph Not Through lymph Distant submucos node through bowel wall node metastases > 90 A bowel wall 70– 75% metastases < 5% % 25– 45% 80– 85% 50– 65%
Stages of CRC
Sites of metastasis Via blood Liver Via lymphatics Lymph nodes Per continuitatem Lung Abdominal wall Brain Nerves Bones Vessels
Factors Associated with CRC Screening · · · Higher socio-economic status Higher education White Older age (>50 years) Men Married
Stages of CRC Three elements: T = Tumor How large is the tumor? N = Node Are cancer cells in the lymph nodes? M = Metastases Has the cancer spread to other organs? Four stages: Stage I Spread to the middle layers of the colon or rectum Stage III Stage IV Advanced disease, spread to other organs
Consider a second opinion… You have the right to get a second, and even a third, opinion It is very common and accepted It’s never too late to get another opinion There is no one “right” way to treat CRC Talking with different experts can help you feel more confident in your course of action A second opinion might introduce you to a clinical trial or targeted treatment you didn’t know about
Making Treatment Decisions
Goals of Treatment is defined by stage and type of cancer present Goals of Treatment for Early Disease Remove cancer cells Kill cancer cells Keep the cancer cells from returning Goals of Treatment for Advanced Disease • Slow or stop the growth of cancer cells • Manage quality of life concerns Every person responds differently to treatment, so communication is key!
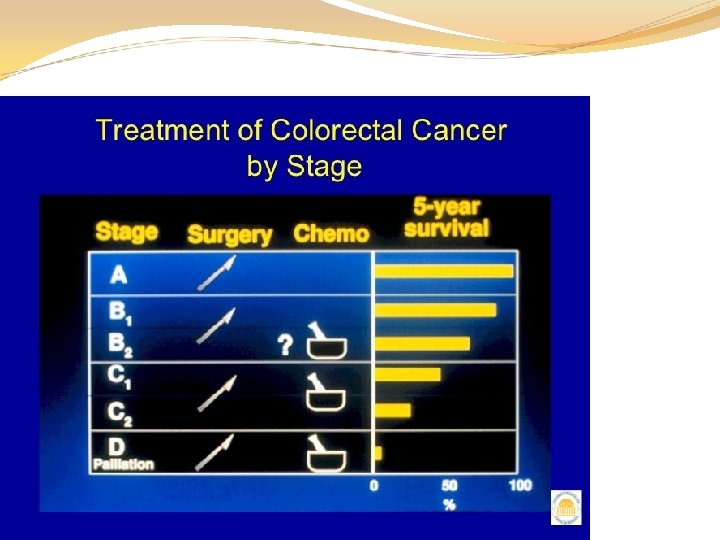
Types of Treatments Surgery Laparoscopy vs. open surgical resection Colostomy: temporary or permanent Chemotherapy Adjuvant, neoadjuvant, and palliative Oral versus intravenous Targeted agents EGFR inhibitors VEGFR inhibitors Chemoradiation (rectal cancer) Clinical trials New agents, combination regimens
Targeted Therapies/ Biologic Agents Targeted therapies work through specific pathways involved in cancer growth to attack cancer cells directly EGFR inhibitors (i. e. : Cetuximab and Panitumumab) VEGFR inhibitors (i. e. : Bevacizumab) Targeted therapies cause fewer side-effects since they attack cancer cells more specifically
Chemotherapy of Colorectal Cancer Agent FDA approval status 5 -FU 1962 Irinotecan (CPT-11) 1998 (second-line) 2000 (first-line) Capecitabine (oral 5 -FU) 2001 (first-line) Oxaliplatin 2002 (second-line) 2004 (first-line)
Targeted Therapy of Colorectal Cancer Agent FDA approval status Bevacizumab 2004 (Anti-VEGF Ab) Cetuximab (Anti-EGFR Ab) 2004 Panitumumab (Anti-EGFR Ab) 2006
Historical Progress of Therapy of Advanced CRC Supportive Care ~4 -6 mo 1 Active Drug (5 -FU/LV, Capecitabine) ~10 -12 mo 2 Active Drugs (5 -FU/LV + Oxaliplatin/Irinotecan; Capecitabine + Oxaliplatin/Irinotecan) ~15 mo ~20 mo 2 Active Drugs + 20. 3 mo bevacizumab >24 -28 mo 2/3 Active Drugs + Targeted/Biologic Agents 0 6 12 18 Median Survival (months) 24
Clinical Trials Clinical trials study promising new drugs and treatment regimens Every CRC treatment regimen that is now “standard” was first developed through a clinical trial Remember that all standard cancer drugs used to treat CRC and other cancer types were studied in clinical trials before being approved by the US FDA
What Affects Treatment Decisions? The type and stage of your disease The specific genetic make-up of your colon cancer Your age and overall health Other medical conditions Whether or not you’ve had cancer and/or cancer treatment in the past Your willingness/ability to tolerate certain side effects Ease and convenience of treatment – oral vs intravenous Insurance coverage and costs
Managing Side Effects
Managing Side Effects You may not experience common side effects Ask about preventing side effects before treatment Having information about short and long term side effects before, during, and after cancer treatment will help you prepare Goal: take control of side effects before they take control of you
Side Effects from Surgery Initial pain and risk of infections Scarring and adhesions Fecal incontinence Ostomy : a procedure to make a new path for stool ostomy pouch is adhered to your skin to collect waste Avoid wearing extremely tight clothes
Side Effects from Chemotherapy Diarrhea Mouth sores Alopecia Neuropathy High blood pressure Skin rash Bowel perforation Allergic reaction
Managing Bowel Issues Obstruction and/or perforation Caused by the cancer itself, or treatment Symptoms include: abdominal pain, nausea and vomiting, bloating, inability to pass gas, constipation or diarrhea, loss of appetite Get suggestions from your medical team for diet and lifestyle changes to help lessen pain and motivate your digestive system
Colorectal Cancer Survivorship
Quality of Life A colorectal cancer diagnosis raises both physical and emotional issues to manage Feeling sad, alone, angry, anxious, overwhelmed or distressed is very common Know that it is possible to find a balance between medical concerns, relationships, work, finances, and other responsibilities Here are some suggestions …
Strategies for Wellness Physical Activity… elevates mood, combats fatigue, maintains function, promotes rest Healthy Foods… maintains energy, strengthens immune system, avoids/limits symptoms, provides comfort Drink Plenty of Fluids… avoids dehydration, promotes regularity, combats fatigue Pamper Yourself… find time to relax, seek spirituality, enjoy each day Create a personalized care plan… set goals, find resources, use support
Fear of Recurrence Be informed Talk about it with your medical team Allow yourself to feel up and down—it is healthy to express negative emotions Be “Patient Active” – take control of what you can, but know what you can’t control Do not to let anxiety and fear prevent you from seeking medical care
Survivorship Advances are being made, giving more patients the chance for a longer, better quality of life after diagnosis Doctors, nurses, social workers and other survivors can help patients and families cope with the diagnosis Emotional support through treatment and beyond is important: seek-out support
CRC Screening Guideline: Summary · For average risk persons, CRC screening should begin at age 50 · African-Americans should be screened earlier starting at age 45 · CRC screening is cost-effective · CRC is highly curable when diagnosed at an early stage with 90% 5 -year survival
Issues Related to CRC Screening · Practical barriers - System - Cost - Environment/area - Lack of access to healthcare provider · Psychological barriers - Lower knowledge or awareness - Lower perceived risk of CRC - Negative attitudes towards screening - Higher worry or fear of CRC
Screening = Prevention & Early Detection Prevention = polyp removal Decreased Incidence Early Detection Decreased Mortality
Screening Methods · Annual Fecal Occult Blood Test (FOBT) · Flexible Sigmoidoscopy every 5 years · Annual FOBT + Flexible Sigmoidoscopy every 5 years · Colonoscopy every 10 years · Colonoscopy - gold standard
Other Screening Tests · Virtual colonoscopy · · Sensitivity 94%, Specificity 96% – Advantages: no need for sedation, noninvasive, rapid imaging of entire colo rectum, low risk of complications – Especially useful in patients who can not undergo colonoscopy Stool DNA testing Video capsule
Types of Screening fecal occult blood test (FOBT) chemical test for blood in a stool sample. annual screening by FOBT reduces colorectal cancer deaths by 33% Flexible sigmoidoscopy can detect about 65%– 75% of polyps and 40%– 65% of colorectal cancers. rectum and sigmoid colon are visually inspected
THANKS