ALEXANDRE ALESSI Educao Mdica Continuada Atualizao HIPERTENSO ARTERIAL





















, incluindo")
, incluindo com Diabetes com")




















 should")









- Slides: 55
ALEXANDRE ALESSI Educação Médica Continuada Atualização HIPERTENSÃO ARTERIAL
CONSIDERAÇÕES GERAIS • HAS é o fator mais comum passível de prevenção para causar doença ou morte • Há suficiente evidência científica para seu tratamento e redução do risco cardiovascular • Diretriz ou guidelines são a interelação entre a pesquisa e a atuação clínica para melhorar a sobrevida dos pacientes
Dados Mundiais Mortes em 2000 atribuíveis à fatores de risco selecionados Hipertensão Tabagismo Colesterol elevado Baixo Peso Sexo não-seguro Baixo consumo de vegetais Obesidade Sedentarismo Alcoolismo Água imprópria Fumaça de combustível sólido (indoor) Deficiência de ferro Poluição urbana do ar Deficiência de zinco Deficiência de vitamina A Injeções não-seguras no cuidado à saúde Fatores de risco ocupacionais 0 1. 000 2. 000 3. 000 4. 000 5. 000 6. 000 7. 000 8. 000 Número de mortes WHO 2002
Continuum Cardiovascular Adapted from Dzau V, Braunwald E. Am Heart J. 1991; 121: 1244 -1263.
O risco de mortalidade CV dobra a cada aumento de 20/10 mm. Hg da PA* 8 7 6 Risco de 5 Mortalidade 4 CV 3 2 1 0 115/75 135/85 155/95 PAS/PAD (mm Hg) 175/105 *Indivíduos com 40 -70 anos, iniciando com PA de 115/75 mm Hg. Lewington S, et al. Lancet. 2002; 60: 1903 -1913. JNC 7. JAMA. 2003; 289: 2560 -2572.
Prevalence % Epidemiologic impact on mortality of blood pressure reduction in the population After Intervention Before Intervention Reduction in BP % Reduction in Mortality Reduction in SBP (mm. Hg) Stroke CHD Total 2 -6 -4 -3 3 -8 -5 -4 5 -14 -9 -7 Adapted from Whelton, PK et al. JAMA 2002; 288: 1882 -1888
e
CARACTERÍSTICAS Clinical Guidelines We Can Trust ISENTO E INDEPENDENTE “ Wait “ JNC!!!
8 JNC – 2014 – Guideline for the management of High Blood Pressure in Adults • 10 anos após 7 JNC – último foi 2003 !! • • • • Participantes: 14 HIPERTENSÓLOGOS 6 PRIMARY CARE 2 GERIATRAS 2 CARDIOLOGISTAS 3 NEFROLOGISTAS 1 ENFERMEIRA 2 FARMACOLOGISTAS 6 EXPERTS EM ESTUDOS CLÍNICOS 3 EXPERTS EM MED BASEADA EM EVIDÊNCIAS 1 EPIDEMIOLOGISTA 4 EXPERTS EM INFORMÁTICA 4 EXPERTES EM DESENVOLVIMENTO E IMPLEMENTAÇÃO DE DIRETRIZ OU GUIDELINES REVISADO POR 20 MEMBROS – NHBLI REVISADO POR 16 AGÊNCIAS REGULADORAS FEDERAIS • •
CARACTERÍSTICA SIMPLES E DIRECIONADO AO MÉDICO NA PRIMEIRA LINHA DE ATENDIMENTO RESPONDER 3 PERGUNTAS
CARACTERÍSTICA RESPONDER 3 PERGUNTAS
S
S
METODOLOGIA
CARACTERÍSTICA RESPONDER 3 PERGUNTAS 8 JNC FEZ: 9 RECOMENDAÇÕES
Recomendações 1. Na população geral acima de 60 anos – iniciar o tratamento farmacológico com pressão arterial maior ou igual 150/90 mm. Hg. Meta de tratamento abaixo de 150/90 mm. Hg. Recomendação A – forte recomendação
Recomendações obs. Na população geral acima de 60 anos – se o tratamento farmacológico da pressão arterial sistólica é menor que 140 mm. Hg, e o tratamento é bem tolerado e sem efeitos colaterais, não há necessidade de ajuste de dose. Recomendação E – opinião de experts
Recomendações 2. Na população geral abaixo de 60 anos – iniciar o tratamento farmacológico da pressão arterial diastólica com valores maiores ou igual a 90 mm. Hg. Meta do tratamento menor que 90 mm. Hg. Idade 30 -59 anos -Recomendação A – forte recomendação Idade 18 -29 anos –Recomendação E – opinião de experts
Recomendações 3. Na população geral abaixo de 60 anos – iniciar o tratamento farmacológico da pressão arterial sistólica com valores maiores ou igual a 140 mm. Hg. Meta do tratamento menor que 140 mm. Hg. Recomendação E – opinião de experts
Recomendações 4. Na população com 18 anos ou mais com Doença Crônica Renal – iniciar o tratamento farmacológico com pressão arterial maior ou igual 140/90 mm. Hg. Meta de tratamento abaixo de 140/90 mm. Hg. Recomendação E – opinão de experts
Recomendações 5. Na população com 18 anos ou mais com Diabetes – iniciar o tratamento farmacológico com pressão arterial maior ou igual 140/90 mm. Hg. Meta de tratamento abaixo de 140/90 mm. Hg. Recomendação E – opinão de experts
Recomendações 6. Na população geral não da raça negra ( não afroamericano ), incluindo com Diabetes com 18 anos ou mais– iniciar o tratamento farmacológico com diurético tiazídico, bloq canal de cálcio, inibidor da enzima conversora de angiotênsiva ou bloq do receptor de angiotênsina II. Recomendação B – moderada evidência científica
Recomendações 7. Na população geral da raça negra (afroamericano ), incluindo com Diabetes com 18 anos ou mais – iniciar o tratamento farmacológico com diurético tiazídico e bloqueador do canal de cálcio Raça negra -Recomendação B – moderada evidência científica Raça negra e diabetes – Recomendação C – fraca evidência cienetífica
Recomendações 8. Na população com 18 anos ou mais com Doença Crônica Renal –o tratamento farmacológico deve incluir ( iniciar ou associar ) inibidores da enzima conversora de angitênsina ou bloq do receptor da angiotênsina, para melhorar a evolução da DCR. Independemente de raça ou diabetes. Recomendação B – moderada evidência
9. ü ü ü Recomendações Considerar: Atingir as metas em 1 mês Aumentar dose ou associar Ajuste de doses e associação até atingir metas – 2 -3 drogas ü Nunca associar IECA com BRA ü Quarta droga pode ser usada ü Sem controle – indique especialista em HAS Recomendação E – opinão de experts
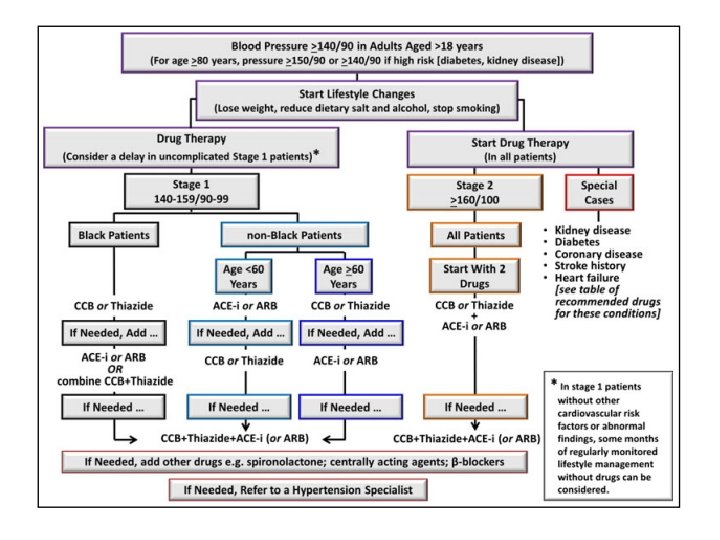
MUDANÇAS • In patients 60 years or over, start treatment in blood pressures >150 mm Hg systolic or >90 mm Hg diastolic and treat to under those thresholds.
MUDANÇAS • In patients <60 years, treatment initiation and goals should be 140/90 mm Hg, the same threshold used in patients >18 years with either chronic kidney disease (CKD) or diabetes.
MUDANÇAS • In nonblack patients with hypertension, initial treatment can be a thiazide-type diuretic, CCB, ACE inhibitor, or ARB, while in the general black population, initial therapy should be a thiazide-type diuretic or CCB.
MUDANÇAS • In patients >18 years with CKD, initial or addon therapy should be an ACE inhibitor or ARB, regardless of race or diabetes status.
MUDANÇAS • In patients 60 years or over, start treatment in blood pressures >150 mm Hg systolic or >90 mm Hg diastolic and treat to under those thresholds. • In patients <60 years, treatment initiation and goals should be 140/90 mm Hg, the same threshold used in patients >18 years with either chronic kidney disease (CKD) or diabetes. • In nonblack patients with hypertension, initial treatment can be a thiazide-type diuretic, CCB, ACE inhibitor, or ARB, while in the general black population, initial therapy should be a thiazide-type diuretic or CCB. • In patients >18 years with CKD, initial or add-on therapy should be an ACE inhibitor or ARB, regardless of race or diabetes status.
Date of download: 2/27/2014 Copyright © 2014 American Medical Association. All rights reserved.
Date of download: 2/27/2014 Copyright © 2014 American Medical Association. All rights reserved.
ESTRATÉGIAS Figure Legend: Strategies to Dose Antihypertensive Drugsa Date of download: 2/27/2014 Copyright © 2014 American Medical Association. All rights reserved.
Figure Legend: Guideline Comparisons of Goal BP and Initial Drug Therapy for Adults With Hypertension Date of download: 2/27/2014 Copyright © 2014 American Medical Association. All rights reserved.
COMO ERA ATÉ PUBLICAÇÃO DO 8 JNC?
Part 2: Recommendations for Hypertension Treatment 2014 Canadian Hypertension Education Program Recommendations
The full slide set of the 2014 CHEP Recommendations is available at www. hypertension. ca
The Canadian Hypertension Education Program: 2014 Recommendations What’s still important? • Out-of-office blood pressure measurements are important in both the diagnosis and management of hypertension • The management of hypertension is all about global cardiovascular risk management and vascular protection • Single pill combinations help achieve blood pressure control • The most important step in prescription of antihypertensive therapy is achieving patient “buy-in”
Recommendations 2014 Table of contents I. Health behaviours management II. Indications for drug therapy III. Choice of therapy IV. Global vascular protection V. Goal of therapy VI. CV – IHD VII. CHF VIII. Cerebrovascular / Stroke IX. LVH X. Chronic kidney disease XI. Renovascular XII. Diabetes XIII. Adherence strategies for patients XIV. Endocrine
I. Health Behaviours Management 2014 Canadian Hypertension Education Program Recommendations
Health Behaviour Recommendations for Prevention and Treatment of Hypertension To reduce the possibility of becoming hypertensive, Reduce sodium intake towards 2000 mg/day • Healthy diet: high in fresh fruits, vegetables, low fat dairy products, dietary and soluble fibre, whole grains and protein from plant sources, low in saturated fat, cholesterol and salt in accordance with Canada's Guide to Healthy Eating. I. Regular physical activity: accumulation of 30 -60 minutes of moderate intensity dynamic exercise 4 -7 days per week in addition to daily activities; For non-hypertensive or stage 1 hypertensive individuals, the use of resistance or weight training exercise (such as free weight lifting, fixed-weight lifting, or handgrip exercise) does not adversely influence blood pressure. • Low risk alcohol consumption: (≤ 2 standard drinks/day and less than 14/week for men and less than 9/week for women) • Attaining and maintaining ideal body weight (BMI 18. 5 -24. 9 kg/m 2) • Waist Circumference: Men <102 cm Women <88 cm • Tobacco free environment
Potential Benefits of a Wide Spread Reduction in Dietary Sodium in Canada Reduction in average dietary sodium from about 3500 mg to 1700 mg 1, 2 • 1 million fewer hypertensives • 5 million fewer physicians visits a year for hypertension • Health care cost savings of $430 to 540 million per year related to fewer office visits, drugs and laboratory costs for hypertension • Improvement of the hypertension treatment and control rate • 13% reduction in CVD • Total health care cost savings of over $1. 3 billion/year 1. Penz ED. Cdn J Cardiol 2008 2. Joffres MR. Cdn J Cardiol 2007: 23(6)
Health Behaviour Recommendations for Hypertension: Physical Activity Should be prescribed to reduce blood pressure F Frequency - Four to seven days per week I Intensity - Moderate T Time T Type - 30 -60 minutes Cardiorespiratory Activity - Walking, jogging - Cycling - Non-competitive swimming Exercise should be prescribed as an adjunctive to pharmacological therapy
Health Behaviour Recommendations for Hypertension: Weight Loss Height, weight, and waist circumference (WC) should be measured and body mass index (BMI) calculated for all adults. Hypertensive and all patients BMI over 25 - Encourage weight reduction - Healthy BMI: 18. 5 -24. 9 kg/m 2 Waist Circumference Men <102 cm Women <88 cm For patients prescribed pharmacological therapy: weight loss has additional antihypertensive effects. Weight loss strategies should employ a multidisciplinary approach and include dietary education, increased physical activity and behaviour modification CMAJ 2007; 176: 1103 -6
Waist Circumference Measurement Measure here Iliac crest Courtesy J. P. Després 2006
Health Behaviour Recommendations for Hypertension: Alcohol Low risk alcohol consumption • 0 -2 standard drinks/day • Men: maximum of 14 standard drinks/week • Women: maximum of 9 standard drinks/week A standard drink is about 142 ml or 5 oz of wine (12% alcohol). 341 m. L or 12 oz of beer (5% alcohol) 43 m. L or 1. 5 oz of spirits (40% alcohol).
Health Behaviour Recommendations for Hypertension: Stress Management Stress management Hypertensive patients in whom stress appears to be an important issue Behaviour Modification Individualized cognitive behavioural interventions are more likely to be effective when relaxation techniques are employed.
Health Behaviours in Adults with Hypertension: Summary Intervention Target Reduce foods with added sodium Weight loss BMI <25 kg/m 2 Alcohol restriction < 2 drinks/day Physical activity Dietary patterns 30 -60 minutes 4 -7 days/week DASH diet Smoking cessation Smoke free environment Waist circumference Men <102 cm → 2000 mg /day Women <88 cm 2014
IV. Vascular Protection for Hypertensive Patients: ASA Low dose ASA in patients >50 years Caution should be exercised if BP is not controlled. Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet 1998; 351: 1755 -1762. 2014
XIII. Adherence 2014 Canadian Hypertension Education Program Recommendations
Sodium Slide Kit • Tool used to educate the public and patients on dietary sodium. • Annually updated. Download at www. hypertension. ca
Brief Hypertension Action Tool Can by used by a healthcare provider to better inform and engage a hypertensive patient to ultimately become more active in their care. Involves 3 Action Tools: Action Tool # 1 – Explains High BP Action Tool # 2 – Self-management of lifestyle Action Tool # 3 – Proper home measurement & information about medication Download at www. hypertension. ca
Measuring Blood Pressure The Right Way – Poster • Pocket cards can be ordered from our website. • Brief highlights: 1. Preparing to taking your blood pressure 2. Using endorsed BP devices. Posters can be ordered at www. hypertension. ca