Urologic Diseases and Nephrolithiasis Victor Politi M D










 xage < 35")






















- Slides: 37
Urologic Diseases and Nephrolithiasis Victor Politi, M. D. , FACP Medical Director, St. John’s University -School of Allied Health Professions, Physician Assistant Program
Urologic Diseases z Testicular torsion z Epididymitis/orchitis z Hernias z Incontinence z Phimosis/paraphimosis z Prostatitis
Acute Scrotum
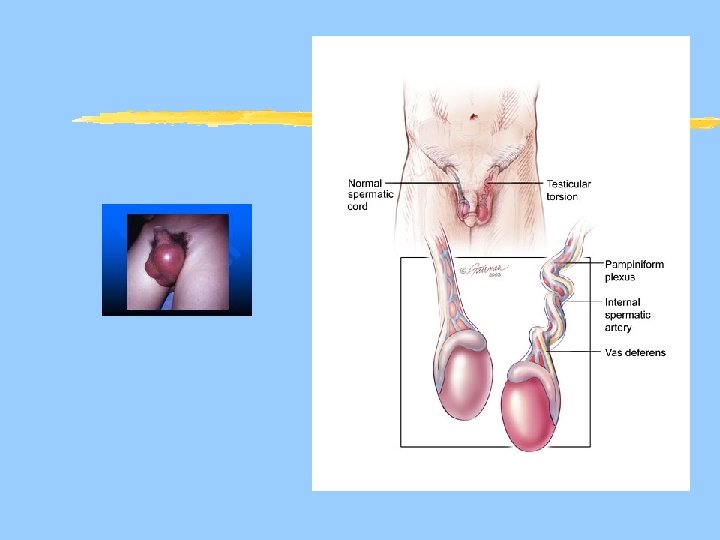
Testicular Torsion z. Twisting of the testes and spermatic cord around a vertical axis z. Leads to venous obstruction, progressive swelling, arterial compromise and eventually testicular infarct
Testicular Torsion z. Must be considered initial diagnosis of scrotal pain! z. Exam: yreveals painful testi that may have a high lie
Testicular Torsion z. Epidemiology: Usually young males z. Presentation: Sudden onset of scrotal pain, PMH of cryptorchidism, red, swollen scrotum, negative Prehn’s sign (relief of pain by elevation of testicles) zmanagement: Emergent surgical detorsion
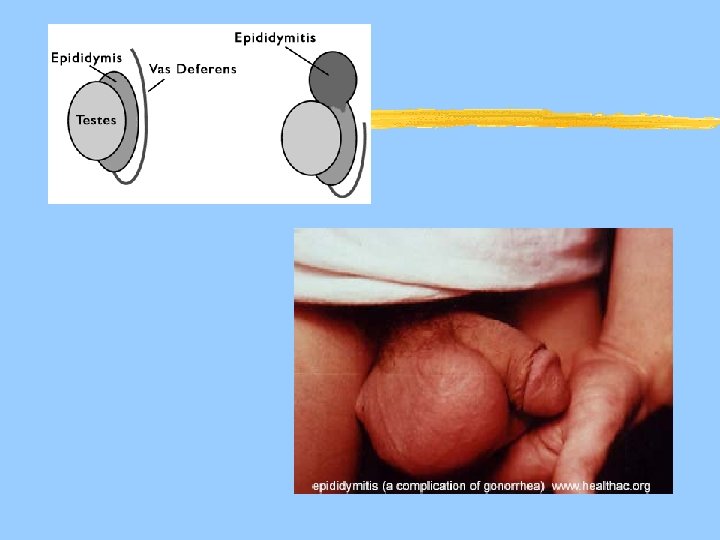
Epididymitis z. Infection of the epididymis acquired by retrograde spread of organisms via the urethra to the ejaculatory duct, then down the vans deferens to the epididymitis z. Acute infectious process associated with painful enlargement of epididymis
Epididymitis z. Most cases of acute epididymitis are infectious ztwo categories ysexually transmitted -typical with C. trachomatis or N. gonorrhoeae ynon-sexually transmitted (typically older men) associated with UTI prostatitis, caused by gram negative rods ytx with amiodarone has been associated with epididymitis
Epididymitis z. Symptoms may follow acute physical strain, trauma, or sexual activity, usually associated with urethritis z. Fever and scrotal swelling are common z. The epididymis is located posterior lateral to the testis
Epididymitis z. Presentation: ycoexisting UTI or prostatitis yusually adult males yheaviness and dull aching discomfort in affected hemiscrotum which can radiate to flank yepididymis indistinguishable from testis yerythematous scrotum ypositive Prehn’s sign (pain relief by elevation of scrotum in supine patient)
Epididymitis z. Management: yrule out torsion yantibiotics (directed toward identified pathogen) xage < 35 chlamydia (sexual partner treated also) xage > 35 E. coli y. Urine culture ybed rest w/scrotal elevation in acute phase
Orchitis z. Inflammation of the testes due to STD or inadequate immunization zepidemiology: manifestation of STD gonorrhea or chlamydial infection, non STD with viral mumps or rarely filariasis
Orchitis z. Presentation: y. Painful testes y. Hx of postpubertal mumps ytender, swollen testis ydifficult to distinguish epididymis yparotid swelling (with mumps)
Orchitis z. Management: yantibiotics if bacterial ysymptomatic if viral
Inguinal hernias z Direct Hernia y. History: xmen over 40 xlarge, painless groin mass for many years z Indirect hernia y. History: x. Most common xpainless scrotal mass
Inguinal hernias z Direct hernia y. Physical Exam x. Palpable mass at side of finger outside of inguinal canal z Indirect hernia y. Physical Exam x. Palpable mass at tip of finger in inguinal canal x. Large mass in scrotum
Inguinal Hernias z. Management: y. Avoid strangulation or incarceration, otherwise elective surgical repair
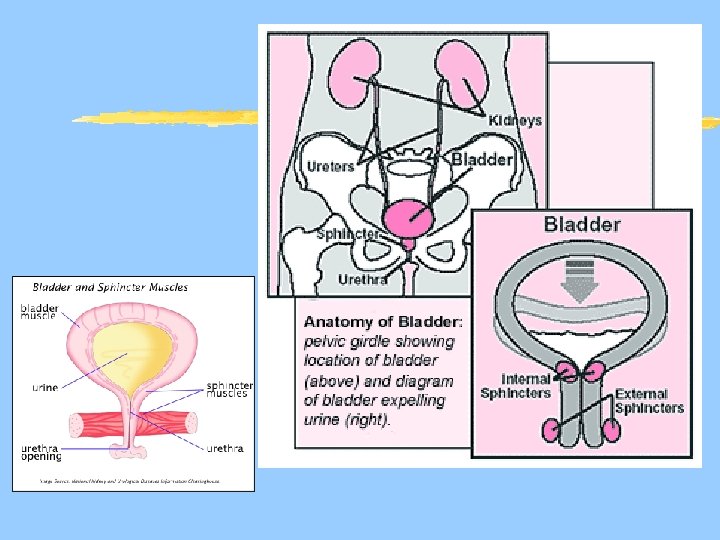
Interstitial Cystitis z. Pain with full bladder relieved by emptying associated with urgency and frequency. z Dx of exclusion z no other cause of cystitis I. E. radiation cystitis, chemical cyctitis (cyclophosphamide), vaginitis, urethral diverticulum
Interstitial Cystitis z. Etiology is unkown z assoc with irritable bowel dz, or inflammatory bowel dz and persons with severe allergies. z. Dx made with cystoscopy after hydrodilitation to detect submucosal hemorrhage.
Interstitial Cystitis z. There is no cure for IC z. Tx includes hydrodistention for symptomatic relief z. Amitriptyline, calcium channel blockers z. DMSO, intravesical instillation of dimethyl sulfoxide, heparin or. BCG z. Surgery as last resort.
Phimosis/Paraphimosis z. Presentation: y. Uncircumcised male ypainful penis or foreskin yhx of catheterization yinflamed retracted foreskin yerythematous, edematous glans
Phimosis/Paraphimosis z. Management: ycompression of the glans with forward traction on the foreskin may reduce paraphimosis, phimosis may resolve, if not prompt circumcision required
Prostatitis z. Presentation: ysuprapubic or pudendal pain yfever ydysuria yhematuria ytender, fluctuant prostate
Prostatitis z. Management: y. E. Coli most common bacterial- treat with antibiotics 30 days if acute, 6 -8 weeks is chronic y. Chlamydia is typical “non bacterial” agent, yalso prostatic massage, diet
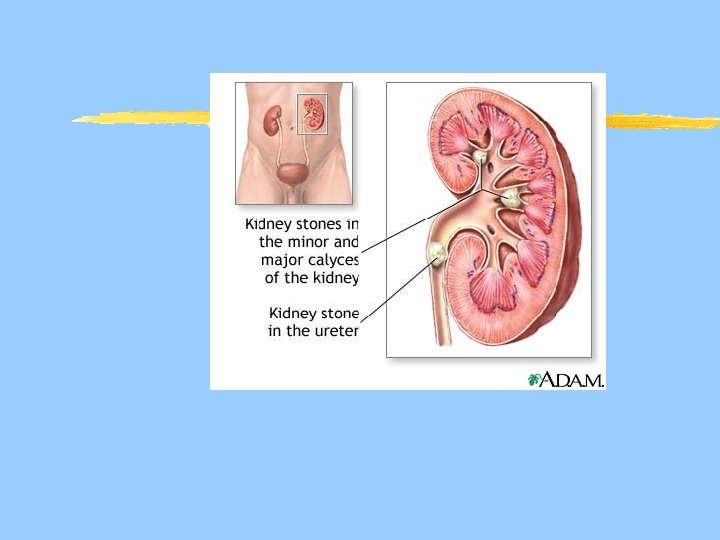
Nephrolithiasis z. Renal stones occur throughout the urinary tract - common causes of pain, infection, obstruction z. Formed in proximal tract and pass distally, lodging at ureteropelvic junction, ureter at iliacs, and ureterovesical junction
Nephrolithiasis z. Four Basic Types: y. Calcium phosphate/oxalate 80% y. Uric acid 5% y. Cystine 2% y. Struvite <2% y. Calcium stones are radiopaque, uric acid stones are radiolucent
Nephrolithiasis z Presentation yback pain and renal colic that waxes and wanes, may awaken from sleep ypain radiates to groin, testicles, suprapubic, patients constantly moving ymay be asymptomatic (non obstructing stones) yhematuria, dysuria, urinary frequency ydiaphoresis, tachycardia, tachypnea yfever and chills, hypertension, CVAT, nausea and vomiting
Nephrolithiasis z. Evaluation: y. CBC w/diff, BUN/creatinine, Ca, Po 4, uric acid y. Urinalysis, urine culture, 24 hr urine y. Plain film of abdomen (90% radiopaque)KUB y. Intravenous urogram y. Retrograde urography y. Ultrasound-- CT w/o contrast best choice yobtain strained urinary sediment for analysis
Nephrolithiasis z. Patients are encouraged to increase fluid intake particularly 2 hours after meals when the body is most dehydrated and before bedtime.
Nephrolithiasis z. Management: y. Stones< 5 mm likely to pass spontaneously xtreat as outpatient; drink y. Stones > 10 mm not likely to pass spontaneously and more likely to have complications xtreat as inpatient; vigorous fluids, IV antibiotics if signs of infection, ureter stent or nephrostomy, IM analgesia
Nephrolithiasis z. Stones 5 -10 MM less likely to pass spontaneously, should be considered for early selective intervention if no complicating factors (infection, high grade obstruction, solitary kidney) z. Larger stones may require ureteroscopic stone extraction ( basket) or extracorporeal shock wave lithotripsy ESWL
Nephrolithiasis z. Patients with renal stones in the renal pelvis without pain, obstruction or infection need not be treated. z. Larger stones that might present a future problem can be removed by percutaneous nephrolithotomy
Questions ?