Treatment of acute coronary syndrome MUDr Denisa Jahnlov









 in the Czech Republic Population")
")




 –")

 Keeley EC. Lancet 2003")










 – in patients undergoing PCI")



- Slides: 40
Treatment of acute coronary syndrome MUDr. Denisa Jahnlová Department of Cardiology FN Motol and 2 nd Medical Faculty of the Charles University
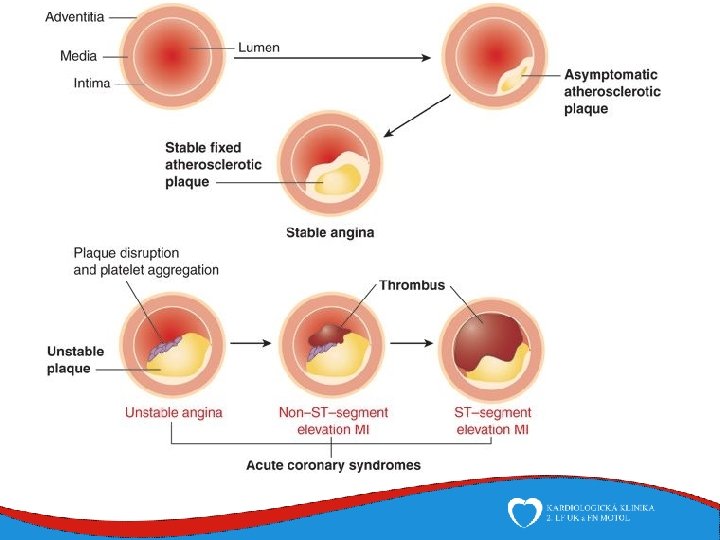
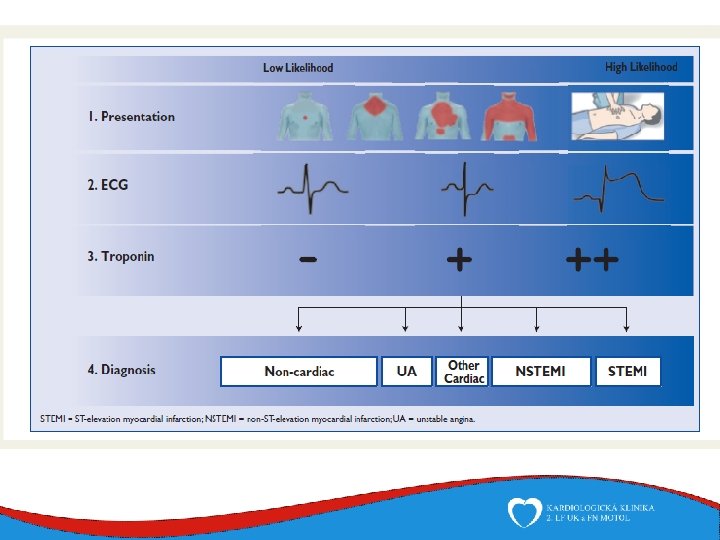
Acute coronary syndromes • Pathophysiologic mechanism – vulnerabile plaque disruption with superimposed thrombus and subsequent coronary blood flow cessation with reduced myocardial supply → acute ischemia → necrosis • Leading symptom - chest pain • 2 groups according to ECG • Patients with acute chest pain and persistent (20 min) ST-segment elevation – This condition is termed ST-elevation ACS and generally reflects an acute total coronary occlusion – Most patients will ultimately develop an ST-elevation myocardial infarction (STEMI) – Immediate reperfusion by primary angioplasty or fibrinolytic therapy • Patients with acute chest pain but no persistent ST-segment elevation – ECG changes may include transient ST-segment elevation, persistent or transient STsegment depression, T-wave inversion, flat T waves or pseudo-normalization of T waves or the ECG may be normal – NSTEMI - myocardial necrosis – NAP - myocardial ischemia without cell loss, lower risk of death
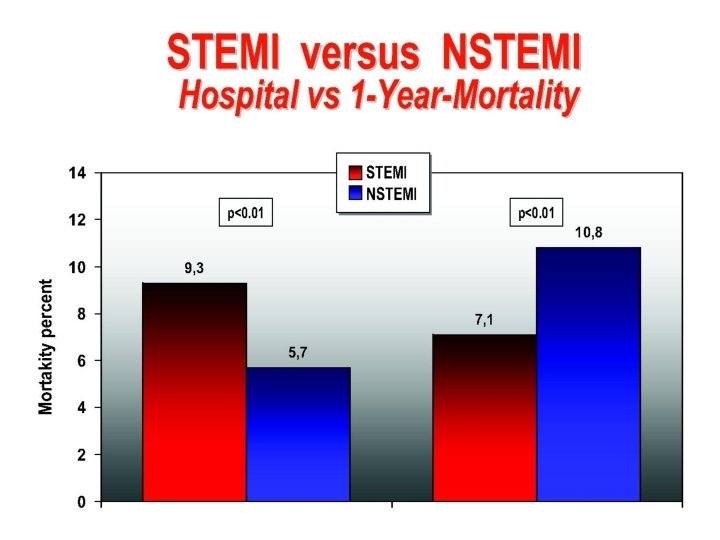
Epidemiology • Incidence of NSTEMI higher than incidence of STEMI In-hospital mortality - Higher in STEMI patients vs. NSTEMI (7 vs. 5%) STEMI - mortality 25 -30% (1960 s) → 10% (nowadays) - Similar in both groups (12 vs. 13%) 6 month mortality Long-term follow-up - Higher in NSTEMI patients - Older patients Comorbidities (diabetes mellitus, renal insuficiency) Generalized atherosclerosis including multivessel coronary disease • Sex differences – men account for more than 90% of patients with AMI at the age under 40 y (a hormonal profile of woman has a protective effect) • Age differences – in patients aged under 40 years only one coronary artery is affected
ACS with ST-segment elevation Pre-hospital management • Relief of Breathlessness – O 2 only to breathless, hypoxic (Sa. O 2<95%), heart failure patient • Relief of pain – human reasons, sympathetic activation-vasoconstiction, increases workload of the heart – titrated i. v. opioids (Morphine, Fentanyl) + antiemetics • Relief of anxiety • explain the situation to the patient, tranquillizer • BB – hypertensive and tachycardic patient – metoprolol, bisoprolol, esmolol – CAVE contraindication: acute cardiac failure, bradycardia
ACS with ST-segment elevation Pre-hospital management • Nitrate – pain, hypertesion, heart failure – sublingual, intravenous (isosorbide dinitrate 1 -5 mg i. v. in hypertensive patients) – CAVE! Contraindications: hypotense, sildenafil → resistent hypotension • Monitoring vital function and ECG – Cardiac arrest due to ventricular fibrillation!!! • Terminated by defibrillation • Theapeutic hypothermia after resuscitation is indicated • Immediate angiography in patients with CA whose ECG shows STEMI/high suspicion on ongoing infarction
ACS with ST-segment elevation Reperfusion therapy: time is muscle!!! • Indication – within 12 h of symptom onset with persistent STE or new LBBB (later → necrosis) – in patients with ongoing ischemia → later – within 120 minutes of first contact with doctor • Types of RT – mechanical (PCI) • preferred reperfusion strategy • randomized clinical trials → superior to fibrinolysis – pharmacological (fibrinolysis)
Prehospital and in-hospital management
Reperfusion Strategy in Europe Reperfusion therapy 37 -93% p. PCI rate varies between 5 and 92%; Thrombolysis 0 -55% EUROPE IS VERY HETEROGENOUS!!!
Annual Incidence of Primary PCIs ≥ 600 p-PCI / million / year 400 -599 p-PCI / million / year 200 -399 p-PCI / million / year <200 p-PCI / million / year Data not known
The distribution of the 22 interventional centers working (24/7) in the Czech Republic Population of the Czech Republic is 10 million people
ACS with ST-segment elevation Mechanical reperfusion therapy - PCI • Primary PCI (p. PCI) is reccomended over fibrinolysis within 120 minutes of FMC • In unstable patients (acute heart failure/cadiogenic shock) unless related delay • Stenting (new generation of DES) + tromboaspiration is recommended balloon angiopasty alone • Radial access should be prefered over femoral access – reduces incidence of acute bleeding events (RIVAL trial) • p. PCI should be limited to the culprit vessel – except of patients in cardiogenic shock and persistent ischemia after PCI
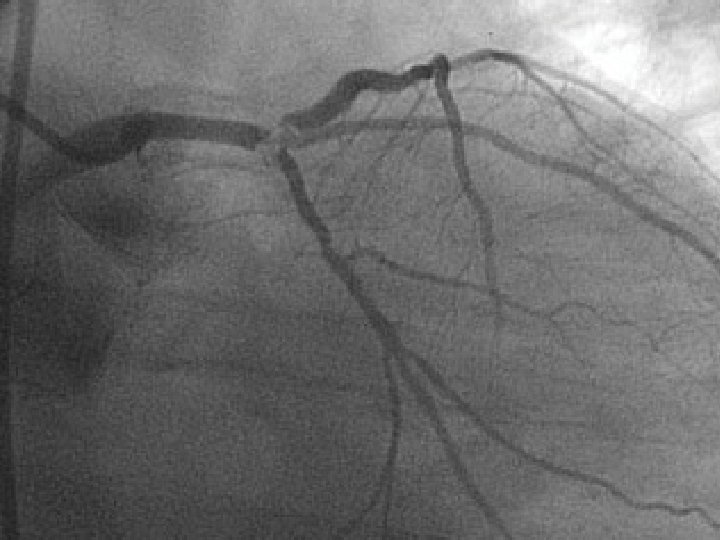
Process of the implantation of stent
Aspiration trombectomy
ACS with ST-segment elevation In-hospital care – periprocedural pharmacotheraphy • DAPT -combination of aspirin + ATP inhibitors – Aspirin • For all patients without contraindications • Initial oral loading dose 150 -300 mg, 75 -100 mg daily – ATP inhibitors • In addition to Aspirin for 12 months unless contraindications • 3 -6 months afted DES implantation in case of high bleeding risk • Ticagrelor – 180 mg loading dose, 90 mg twice daily in all patients with high or intermmidiate ischemic risk • Prasugrel – 60 mg loaging dose, 10 mg daily dose – contraindicated in patients with prior stroke and older > 75 y. and body weight <60 kg • Clopidogrel – 300 -600 mg loaging dose, 75 mg daly dose – Only in patients who cannot recieve ticagrelor or prasugrel or who require oral antikoagulation • PPI inhibitors in patients in risk of gastrointestinal bleeding
ACS with ST-segment elevation In-hospital care – periprocedural pharmacotheraphy • Unfractionated heparin (UFH) – in patients undergoing PCI – 70 -100 IU/Kg i. v. (max. 5000 IU bolus before PCI) – APTT 1, 5 -2, 5 x • LMWH (low molecular weight heparin) – 0, 5 mg/kg i. v. followed by 1 mg/kg s. c. • Fondaparinux is not recommended! • Glykoprotein IIb/IIIa inhibitors – Bailout therapy - only in no-reflow, massive trombus, trombotic complications – Only periprocedural!!!
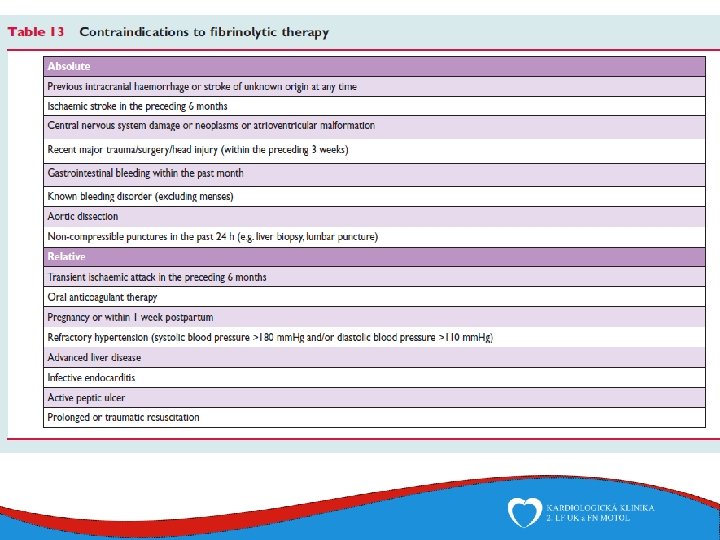
ACS with ST-segment elevation Pharmacological reperfusion therapy: Fibrinolysis • Fibrinolysis is an important in those settings where primary PCI cannot be offered to STEMI patients within the recommended timelines – Higher risk of bleeding, sucesfull only in 70 -80% • Within 12 h of symptom onset if primary PCI cannot be performed within 120 min • Prehospital start – A fibrin-specific agent (tenecteplase, alteplase, reteplase) is recommended – Anticoagulation (UFH/enoxaparin) is recommended until revascularization and for the duration of hospital stay – DAPT (aspirin + clopidogrel) • Transfer to a PCI-capable centre is indicated for all patients following fibrinolysis – Unstable patients - rescue/emergency PCI – Stable patients – PCI in 3 -24 hod
Fibrinolysis x PCI Meta-analysis of 23 trials (n=7739 pts. ) Keeley EC. Lancet 2003
ACS with ST-segment elevation Management during hospitalization • The Coronary Care Unit – Management of arrhythmias, heart failure, mechanical circulatory support and complex (non)invasive and haemodynamic monitoring – Patients should stay on coronary care unit for 2 -3 days (at least 24 hours) • Standard cardiology department – Even after leaving the CCU patients are able to move around the room and in the following days rehabilitate and before discharge they are able to walk up the stairs • The total length of hospitalization is around 1 week • Return to job possible approximately one month after the onset of the symptoms
ACS with ST-segment elevation Management at discharge • Low-risk patients with successful p. PCI could safely be discharged from hospital at day 3 – – – age <70 years LVEF > 45% 1 or 2 VD successful PCI no persistent arrhythmias
ACS with ST-segment elevation Long-term therapies • CAD is a chronic condition and patients who have recovered from a STEMI are at high risk for new events and premature death !!! • Most patients with STEMI who die do so after discharge from the index event!
ACS with ST-segment elevation Long-term therapies- lifestyle interventions and risk factor control - cessation of smoking tight blood pressure control diet and weight control the encouragement of physical activity
ACS with ST-segment elevation Long-term therapies- pharmacotherapy - Antithrombotic therapy - - Beta-blockers - - In all patients without contraindications, especially in patients with heart failure and systolic dysfunction Metoprolol up to 200 mg daily, Carvediol up to 25 mg daily, Bisoprolol up to 10 mg daily Contraindication: in patients in acute phase and heart failure, cardiogenic shock, bradycardia Statins - - DAPT (combination of aspirin + ADP-receptor blocker) for up to 12 months Aspirin indefinitely (75 -100 mg) Tigagrelor/prasugrel is reccomended over clopidogrel for 12 months Lipid-lowering therapy Atorvastatin 40 -80 daily, Rosuvastatin 20 -40 mg daily ACE inhibitors - In all patients without contraindications, especially in heart failure, left ventricular systolic dysfunction, diabetes mellitus Ramipril 1, 25 mg, Lisinopril 2, 5 mg, Enalapril 2, 5 mg In case of intolerance : Valsartan 20 mg twice daily, Losartan, Candesartan is an alternative
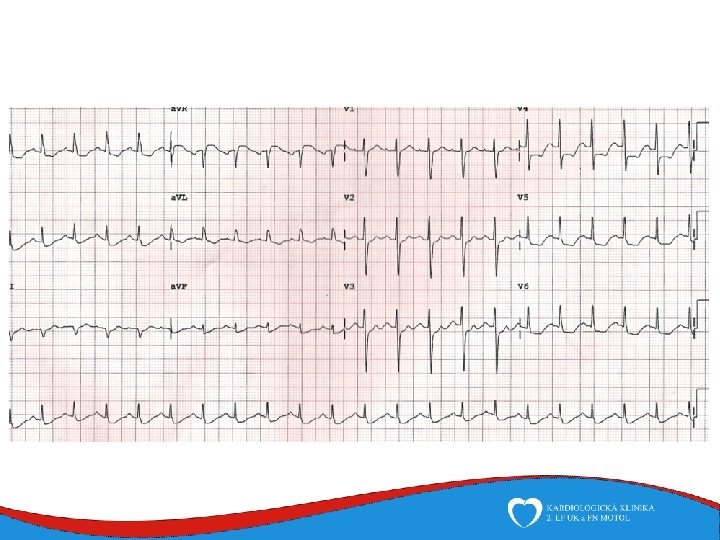
ACS without ST-segment elevation • Patients with acute chest pain but no persistent ST-segment elevation • ECG changes may include – – – transient ST-segment elevation persistent or transient ST-segment depression T-wave inversion flat T waves pseudo-normalization of T waves ECG may be normal • The clinical spectrum of non-ST-elevation ACS (NSTE-ACS) may range from patients – – free of symptoms at presentation individuals with ongoing ischaemia electrical or haemodynamic instability cardiac arrest • The pathological correlate at the myocardial level is – NSTE-myocardial infarction (NSTEMI)- positive hs. Tn. I, cardiomyocyte necrosis – unstable angina –myocardial ischaemia without cell loss, negative hs. Tn. I
ACS without ST-segment elevation Ongoing ischemia • Patients may present with ongoing myocardial ischaemia, characterized by one or more of the following: – – recurrent or ongoing chest pain marked ST depression on 12 -lead ECG heart failure haemodynamic or electrical instability • Immediate PCI is indicated – due to the amount of myocardium in danger and the risk of malignant ventricular arrhythmias
ACS without ST-segment elevation- Risk score and bleeding risk assesment Grace risk score Estimenate the in-hospital mortality, mortality at 6 months, at 1 year and at 3 years The combined risk of death or MI at 1 year Crusade bleeding risk Estimate the patient’s likelihood of an in-hospital major bleeding event baseline patient characteristics Variables : age Systolic blood pressure pulse rate serum creatinine Killip class at presentation cardiac arrest at admission elevated cardiac biomarkers and ST deviation female gender history of diabetes history of peripheral vascular disease or stroke admission clinical variables heart rate systolic blood pressure signs of heart failure admission laboratory values haematocrit calculated creatinine clearance
ACS without ST-segment elevation Pharmacological treatment of ischaemia • Decrease myocardial oxygen demand or increase myocardial oxygen supply • O 2 – only in patients with saturtion less than 90%/in respiratory distress • Beta-blockers – in patients with ongoing ischaemic symptoms and without contraindications • Nitrates – i. v. or sublingual – to relieve angina, uncontrolled hypertension or signs of heart failure – CAVE! Avoid in patients with recent intake of sildenafil • Opiates – only in patients with symtoms despite theraphy with BB and Nitrates • If the patient is not free of signs and symptoms after this treament, immediate PCI is recommended!!!
ACS without ST-segment elevation Platelet inhibition • DAPT -combination of aspirin + ATP inhibitors – Aspirin • For all patients without contraindications • Initial oral loading dose 150 -300 mg, 75 -100 mg daily – ATP inhibitors • In addition to Aspirin for 12 months unless contraindications • 3 -6 months afted DES implantation in case of high bleeding risk • Ticagrelor – 180 mg loading dose, 90 mg twice daily in all patients with high or intermmidiate ischemic risk • Prasugrel – 60 mg loaging dose, 10 mg daily dose – contraindicated in patients with prior stroke and older > 75 y. and body weight <60 kg • Clopidogrel – 300 -600 mg loaging dose, 75 mg daly dose – Only in patients who cannot recieve ticagrelor or prasugrel or who require oral antikoagulation • PPI inhibitors in patients in risk of gastrointestinal bleeding
ACS without ST-segment elevation Anticoagulation • Unfractionated heparin (UFH) – in patients undergoing PCI – 70 -100 IU/kg i. v. (max. 5000 IU bolus berore PCI), APTT 1, 5 -2, 5 x • Fondaparinux – – – The most favourable efficacy – safety profile in NSTEMI Inhibition of Xa 2. 5 mg s. c. daily (CAVE renal insufficiency) OASIS-5 study – less bleeding events Bolus UFH 70 -85 IU/kg during the procedure (to avoid formation of trombus on cathether) • Low molecular weight heparin (LMWH) – In patients pretreated with LMWH – 1 mg/kg twice daly (CAVE renal insufficiency) • Continuation – after sucesfull PCI for 24 h – in conservative treatment during hospital stay
ACS without ST-segment elevation Reperfusion strategy • PCI + implantation of stent (2 nd generation DES) is the method of choise – Timing of PCI according to the risk stratification • Fibrinolysis is not reccomended at NSTEMI • CABG (surgical revascularization) – More frequently multivessel disease with no culprit lesion – Diabetic patients – Higher proportion of surgical high risk charakteristics (x elective CABG) • • Older age Female gender Left main coronary disease LV dysfunction – Higher bleeding and ischemic risk (timing of surgery x DAPT)
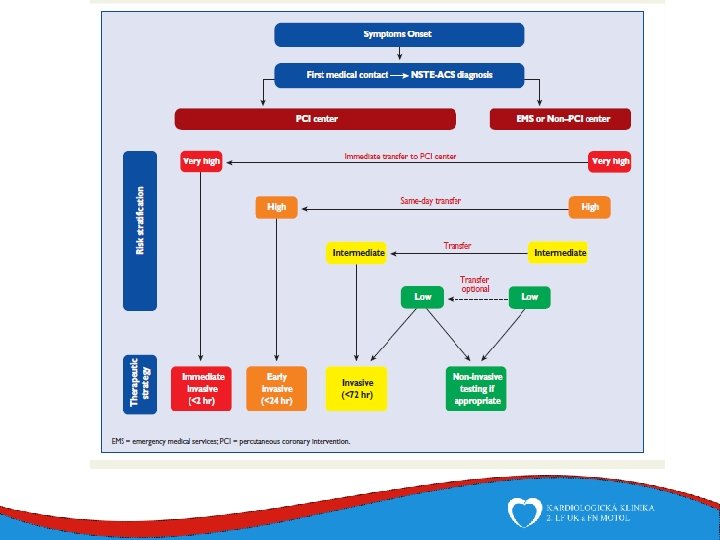
ACS without ST-segment elevation Timing of reperfusion strategy
ACS without ST-segment elevation Long-term therapies- pharmacotherapy - Antithrombotic therapy - - Beta-blockers - - In patients wih heart failure and systolic dysfunction Metoprolol up to 200 mg daily, carvediol up to 25 mg daily, bisoprolol up to 10 mg daily Contraindication: in patients in acute phase and heart failure Statins - - DAPT (combination of aspirin + ADP-receptor blocker) for up to 12 months Aspirin indefinitely (75 -100 mg) Tigagrelor/prasugrel is reccomended over clopidogrel for 12 months Lipid-lowering therapy Atorvastatin 40 -80 daily, Rosuvastatin 20 -40 mg daily ACE inhibitors - Heart failure, left ventricular systolic dysfunction, diabetes mellitus Ramipril 1, 25 mg, Lisinopril 2, 5 mg, Enalapril 2, 5 mg, Valsartan 20 mg twice daily, Losartan, Candesartan is an alternative when intolerance of ACEi is present