Acute Aortic Syndrome Firas F Mussa MD FACS



 Shock Malperfusion Uncontrolled")
 • Diagnosis is missed on initial evaluation in 38% of")


 Inflammatory • Cardiac Stress/Damage – C reactive protein")











- Slides: 21
Acute Aortic Syndrome Firas F Mussa, MD, FACS Vascular Surgery Columbia University Medical Center
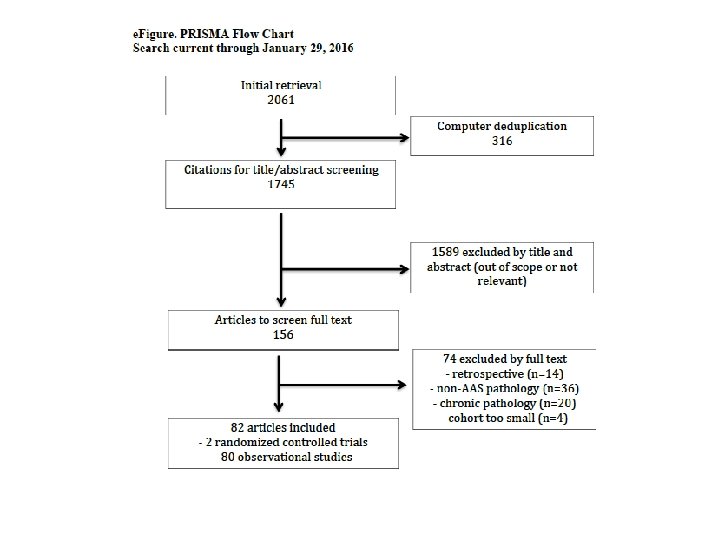
Definitions Mussa FF et al, JAMA, August 16 2016
Type B Dissection-Background Definition of COMPLICATED dissection: Rupture (free or contained) Shock Malperfusion Uncontrolled pain or hypertension
Acute Aortic Dissection (AAD) • Diagnosis is missed on initial evaluation in 38% of patients. (Spitell PC. Mayo Clinic Proc. 1993; 68: 642 -651) Consider AAD in all patients presenting with chest, back or abdominal pain High risk (1) Marfan FH of aortic disease Known AVD Rec. Ao. intervention Known TAA High risk pain (2) features Abrupt onset Severe “Ripping/tearing” High risk exam (3) Pulse deficit Syst BP diff. Focal neurol deficit EDM
An algorithm for the identification and treatment of aortic dissection in patients presenting with chest pain Nienaber, C. A. et al. (2016) Aortic dissection Nat. Rev. Dis. Primers doi: 10. 1038/nrdp. 2016. 53
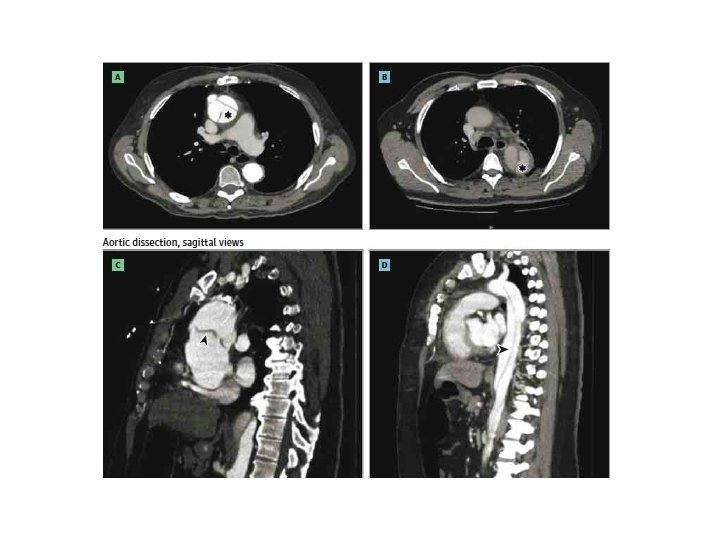
Diagnosis
Diagnose • Novel Tests (Biochemical Markers) Inflammatory • Cardiac Stress/Damage – C reactive protein – IL-6 • Smooth muscle damage – Smooth muscle myosin heavy chain – Calpronin • Thrombosis/ Fibrinolysis – D- dimer – Cardiac troponins – Creatinine kinase – Pro-brain naturetic peptide • Extracellular Matrix damage – MMPs – Soluble elastin fragments
Treatment
Zone 0 – proximal anastomosis If the root is torn or dilated then replace root Surgical Options to Manage aortic root Valve sparing aortic root replacement Bentall Modified Cabrol Aortic root surgery was not associated with increased in hospital mortality, but decreased the likelihood of re-intervention due to late aortic root intervention (Di Eusanio M et al. Ann Thorac Surg 2014; 98: 2078– 85)
Zone 1 or 2 If If a tear is in Zone 1 or 2 you need to replace the Arch Elephant Trunk Frozen Elephant Trunk (FET) Elephant trunk technique for replacement of the aortic arch was advocated by Miyamoto S. et. al (Ann Thorac Cardiovasc Surg. 2006; 12: 412 -6. ) FET combines conventional surgical replacement of the ascending aorta and the aortic arch with endovascular repair of the descending aorta. Associated with similar satisfactory early and mid-term outcomes. Leads to single-stage treatment in a significant number of patients aortic disease. Facilitates endovascular second-stage treatment in patients with residual DTA disease (Di Eusanio M. Ann Thorac Surg 2015; 100: 88– 94. )
Protocol for u. TBAD 14 Safi, MD Courtesy of Hazim
Trial TEVAR for u. TBAD? !!! • • • Consecutive patients in 7 centers in Germany, France, and Italy, uncomplicated dissection 2 -52 weeks 11/2003 -12/2005. Patients were followed up until September 2010 (min 5 years, max 8 years) Median interval until death or latest follow up was 69 months (IQ range 62 -83). No patient lost to follow up Median time between dissection and enrollment 45 days in OMT (20 -252), 39 days in TEVAR (18 -252) Median time between enrollment and TEVAR was 12 days (1 -29) Nienaber CA, et al, Circulation. 2009; 120(25): 2519 -2528
Trial INSTEAD Trial Primary Endpoint §All cause mortality at 2 years §Secondary Endpoints §False lumen thrombosis (FLT) §Degree of aortic expansion §Cardiovascular morbidity §QOL §Length of ICU and hospital stay §Crossover 16
KM estimates of all-cause mortality and progression with landmark analysis 17
So Far… The effectiveness of the current standard medical therapy is unacceptable over the long term (aneurysmal degeneration over 5 years in >60%) The FDA approved TEVAR for all aortic dissections regardless of symptoms The role of TEVAR in reducing overall mortality or major aortic complications have never been conclusively demonstrated (P=NS-INSTEAD-XL) TEVAR induces aortic remodeling (P<0. 001 -INSTEAD-XL, ADSORB) 18
In conclusion………. Type A is best served by Surgery Type B complicated TEVAR unless patients with collagenopathy Type B uncomplicated Medical management followed by TEVAR in sub-acute phase BUT regardless of the treatment path the key is early detection and identification of patients at risk
INTACT-AD Uncomplicated Type B Aortic Dissection TEVAR + Medical Therapy TEVAR/Surgery reserved for complications during follow-up Primary endpoint: Major Aortic Complications-Free Survival over median follow-up of 5 yrs
God created the aorta with ONE lumen…. it should stay that way… 21