RenalGU ITE Review Michelle Slezak Henry Ford Hospital





 • 90% of acute intrinsic renal failure • Renal tubular")
 • Eosinophilia, granular and white cell casts • Causes •")

 • Vasculitis •")

 • A: acidosis • E: electrolyte abnormalities (resistant hyper. K)")
 • Intoxication (alcohol, PCP)")

 • Can present with nephrotic or nephritic")







 •")




– hesitancy, diminished stream quality, dribbling,")





 and forskin (posthitis) • If recurrent, think")


 • Retrograde urethrogram to")





- Slides: 43
Renal/GU ITE Review Michelle Slezak Henry Ford Hospital Department of Emergency Medicine
Renal Failure
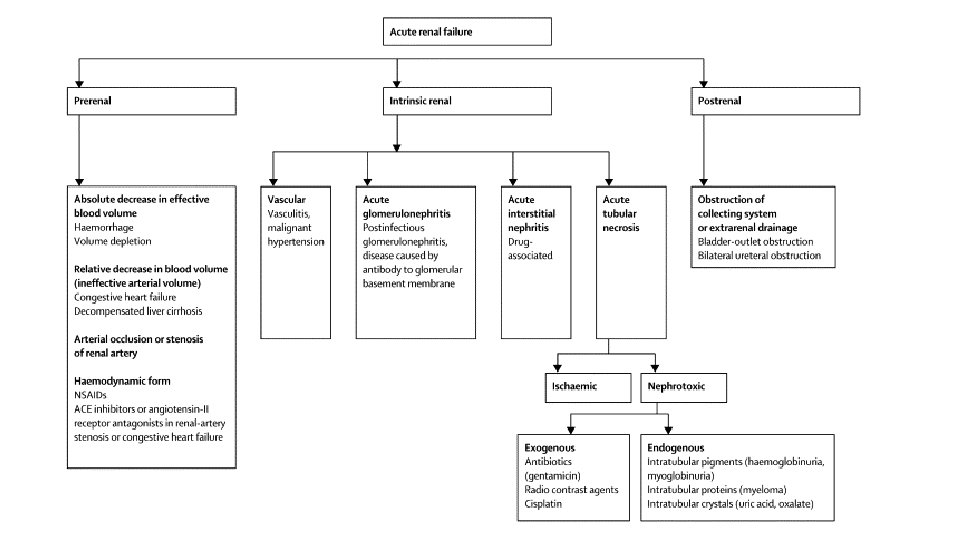
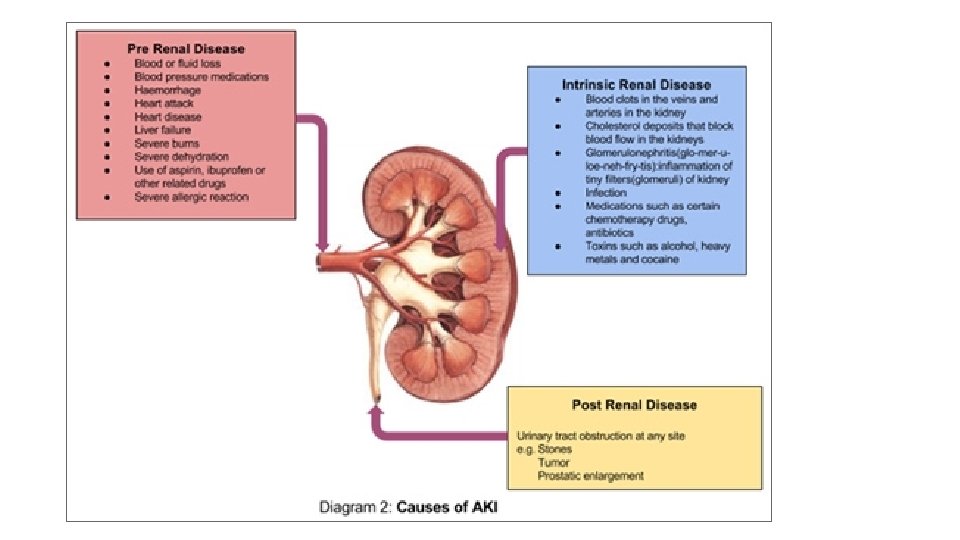
Prerenal azotemia • 60% of AKI • Patients are oliguric • Kidney retains resorptive function and ability to conserve sodium • Urine studies • • • Concentrated (SG >1. 020) Osmolality >500 FENa <1% Urine Na <20 m. Eq/L UA normal or occasional hyaline cast • BUN/Cr >20 • Causes • Hypovolemia (V/D, blood loss, diuretics, skin losses) • Decreased effective blood volume (sepsis, anaphylaxis, third spacing, hypoalbuminemic states, decreased cardiac output) • Treatment- correct hypoperfusion
Postrenal azotemia • 15% of AKI • Obstruction of urine flow at any point from renal collecting system to urethra • Ureteral obstruction must be bilateral • Anuria with complete obstruction to polyuria with partial obstruction • UA normal • Causes • Ureter (crystals, stones, blood clots, malignancy, retroperitoneal fibrosis) • Bladder (BPH-MCC, prostate malignancy, bladder carcinoma, blood clots, neurogenic bladderdrugs, DM, spinal cord injury) • Urethra- stricture, phimosis, meatal stenosis • Treatment- foley catheter
Renal azotemia • 25% of AKI • Pathology of kidney or renal tubule • Tubules lose ability to concentrate and reabsorb sodium • Urine studies • • Dilute (SG 1. 010) Osmolality <300 FENa >2% Urine Na >40 m. Eq/L • BUN/Cr <20
Acute tubular necrosis (ATN) • 90% of acute intrinsic renal failure • Renal tubular cases, muddy brown granular casts • Causes • Ischemia (prolonged hypoperfusion, hemorrhage) • Nephrotoxins (aminoglycosides, ethylene glycol, heavy metals, contrast dye) • Pigments (hemoglobin, myoglobin)
Acute interstitial nephritis (AIN) • Eosinophilia, granular and white cell casts • Causes • Drugs (PCN, cephalosporins, sulfa, NSAIDs, diuretics, allopurinol) • Infection (bacterial, protozoan, fungal) • Immune (lupus, leukemia, lymphoma, sarcoidosis
Glomerulonephritis • RBCs, RBC casts, proteinuria • Hypertension, edema, CHF from volume overload • Causes • Postinfectious (strep-abx do not decrease incidence) • noninfectious
Other intrinsic AKI • Vascular • Vasoconstrictive disease (malignant hypertension, TTP) • Vasculitis • Thrombosis • Renal artery/renal vein • Treatment for all renal AKI • Remove offending agent • Treat any underlying cause
Complications of AKI • Hyperkalemia • Most immediate life-threatening complication • GET AN EKG! • Calcium onset <3 min; gluconate less toxic than chloride if extravasation but may not be effective in low flow states; chloride contains more calcium than gluconate • Albuterol, glucose/insulin, bicarb, Kayexalate, dialysis • Hypocalcemia • Hypomagnesemia • Anion gap metabolic acidosis • Volume overload
Indications for dialysis (AEIOU) • A: acidosis • E: electrolyte abnormalities (resistant hyper. K) • I: ingestion of toxic dialyzable substance (lithium, methanol, ethylene glycol) • O: overload of fluid • U: uremia (pericarditis, encephalopathy, bleeding)
Myoglobinuric renal failure • Trauma (crush, burn, seizure, prolonged exercise) • Intoxication (alcohol, PCP) • Rhabdo myoglobinemia toxic effect on renal tubules ATN renal failure • Urine is reddish-brown, +blood on dipstick, no RBCs on microscopic, renal tubular casts, brown granular casts, myoglobinuria (not reliable) • Serum myoglobin (not reliable), serum CPK (most sensitive), hypocalcemia, hyperkalemia • Treatment- avoid nephrotoxins, aggressive hydration, mannitol, Lasix, alkalinize urine with sodium bicarb
Other renal failure • Nephrotic syndrome • High urine protein excretion, peripheral edema, metabolic abnormalities (hypoalbuminemia, hypercholesterolemia) • Minimal change disease • Kids; may be preceded by URI or immunization; responds to steroids • Focal segmental glomerulosclerosis (FSGS) • African Americans, sickle cell, IVDU, htn, DM; higher frequency of renal failure • Tx- steroids, immunosuppressants • Membranous nephropathy • • Caucasians (30 -50%); HBV, HCV, syphilia, malaria, gold, penicillamind 24% assoc w/ neoplasm Proteinuria, occasional microhematuria, hypercoagulopathy (renal vein thrombosis) Spontaneous remission in 25%
Other renal failure • Membranoproliferative glomerulonephritis (MPGN) • Can present with nephrotic or nephritic features • Assoc w/ infection, autoimmune disease, HCV, cryoglobulins, low C 3 • 50% mortality or progression to ESRD w/in 5 yrs of diagnosis • Diabetic nephropathy • Leading cause of ESRD in US • Onset 5 -10 yrs after onset of type I DM • Tx- TGCP, ACEI • Others • Malignancy (lymphoma, myeloma) • Infection (HIV, HBV, HCV, syphilis, leprosy, malaria) • SLE, amyloidosis, sickle cell, preeclampsia
Dialysis related problems • Vascular access hemorrhage • Minor bleeding from puncture– nonocclusive pressure, reassess for thrill • Significant bleeding from aneurysm or pseudoaneurysm– direct pressure, vascular consult • Vascular access thrombosis • Most common problem • Loss of thrill; unable to access during session • Vascular surgery consult; don’t irrigate b/c can cause clot embolization
Dialysis related problems • Vascular access infection • Often staph; more common in artificial than native grafts • Signs of infection (redness, warmth, induration) may be absent; may only have fever • Treatment– blood cultures, antibiotics (Vanco); may not require device removal • Peritoneal dialysis • Peritonitis– cloudy dialysate effluent • Abdominal pain, fever • Fluid WBC >100 with >50% PMNs or positive Gram stain
Dialysis related problems • Disequilibrium syndrome • • Rapid solute shifts during hemodialysis Most often during first session Headache, nausea, malaise, disorientation, confusion, seizure, coma, death Treatment is supportive; r/o other causes of AMS • Cardiac arrest • Beware of hyperkalemia and acute pericardial tamponade
Urinary Tract Problems
Urinary tract infections • Cystitis • Dysuria, urgency, frequency, hematuria, suprapubic discomfort, significant bacteriuria • Causes– SEEK PP • Staph saprophyticus (2 nd), E coli (1 st), Enterobacter, Klebsiella, Proteus, Pseudomonas • Uncomplicated UTI • Most UTIs; nonpregnant, healthy women with no neurologic or structural dysfunction • Treatment– 3 -6 days (Bactrim, quinolone, nitrofurantoin)
Urinary tract infections • Complicated UTI • Associated with any neurologic, structural, or comorbid condition that increases risk for acquiring infection and reduced efficacy of standard tx regimens • Predispose • Structural (calculi, catheters, stents, prostatic infection, urinary diversion procedures) • Metabolic or hormonal (diabetes, pregnancy) • Vesicoureteral reflux, immunocompromised, recent urinary tract instrumentation, male gender, extremes of age, unusual pathogens, recent antibiotic use of failed treatment for UTI, symptoms longer than 7 days • Treatment– 7 -10 days
Urinary tract infections • Pyelonephritis • Fever, flank pain, vomiting, malaise, CVA tenderness, significant bacteriuria • Consider hospitalization • • • Severe illness/sepsis Extremes of age Uncertain diagnosis h/o stones, obstruction, instrumentation Underlying anatomic urinary tract abnormality Comorbidities Failed outpatient Persistent vomiting Immunocompromised Poor access to followup • Culture all except uncomplicated cystitis
Nephrolithiasis • Composition • 80% contain calcium (2/3 calcium oxalate, 1/3 calcium phosphate) • Dehydration, hyperoxaluria, hypercalciuria (hyperthyroidism, hyperparathyroidism, neoplasm, sarcoidosis, multiple myeloma, distal RTA), PUD (ingest large amts of calcium) • 15% struvite (magnesium-ammonium-phosphate) • Caused by chronic UTI from urea-splitting organisms (Proteus) • 6 -10% uric acid • Gout, myeloproliferative disease, leukemia, high protein diet • 1 -3% cysteine • familial
Nephrolithiasis • Presentation • • • Unilateral colicky pain in flank, back, lower quadrant Radiation to groin, labia, testicles Dysuria, frequency, hematuria Nausea, vomiting Severe discomfort, diaphoresis, restlessness • Beware of AAA, iliac aneurysms, renal vein thrombosis • Diagnosis • • • Only 80% have hematuria 90% seen on KUB; can be used to follow progression/passage CT is test of choice IVP can show delayed nephrogram, hydronephrosis, hydroureter, extravasation US in pregnant and kids Image– first episode, unclear diagnosis, coexistent UTI, elderly
Nephrolithiasis • Most common sites of stone impaction • ureteropelvic junction, pelvic brim (where ureter crosses iliac vessels), ureterovesical junction (most narrow point in ureter) • Likelihood of spontaneous passage • <5 mm pass 90%; 5 -8 mm pass 15%; >8 mm pass 5% • Coexistent UTI is an emergency!! • NSAIDs and narcotics act synergistically • Admit • High-grade obstruction, intractable pain/vomiting, associated UTI, solitary or transplanted kidney, unclear diagnosis, extravasation of dye, renal failure, stone >5 mm (relative)
Bladder calculi • Elderly men • Complication of other urologic disease • Urinary stasis • Infection of residual bladder urine with urea-splitting organisms • Pain on voiding, hematuria, sudden interruption of urinary stream
Hematuria • • • Trauma: bladder injury, ureter injury, retroperitoneal injury Anemia, thrombocytopenia, renal insufficiency: HUS Flank pain: nephrolithiasis Urine + for heme and – for RBCs: rhabdomyolysis Dysuria, frequency: UTI Hearing loss: Alport syndrome Hemoptysis: Goodpasture syndrome Immigrant: Schistosomiasis Nephrotic syndrome, flank pain: renal vein thrombosis Proteinuria, RBC casts: glomerulonephritis Recent URI: glomerulonephritis, Ig. A nephropathy Gross hematuria: imaging is recommended for age >40
Acute urinary retention • Causes • BPH (most common)– hesitancy, diminished stream quality, dribbling, nocturia, sensation of incomplete bladder emptying • Obstructive– prostate carcinoma, prostatitis, urethral stricture, posterior urethral valves, phimosis, pharaphimosis, balanitis, meatal stenosis, calculi, blood clots, circumcision, urethral foreign body, constricting penile ring, clogged Foley • Neurogenic– spinal cord injury, herniated lumbosacral disc (cauda equina), CNS tumors, stroke, diabetes, MS, encephalitis, tabes dorsalis, syringomyelia, herpes simplex, herpes zoster, alcohol withdrawal, postop • Pharmacologic– anticholinergics, antihistamines, antidepressants, antispasmodics, narcotics, sympathomimetics, antipsychotics, antiparkinsonian • Pass a foley, coude, suprapubic catheter • Beware of postobstructive diuresis, especially if chronic urinary retention
Male GU Disorders
Orchitis • Usually direct extension of epididymitis • Viral orchitis caused by mumps • Symptoms evolve several days after onset of parotitis • Testicular pain and swelling
Acute bacterial prostatitis • Frequency, urgency, dysuria, obstructive voiding sx, perineal discomfort, fever, myalgias, malaise, low back or rectal pain • Usually Gram negatives (80% E coli) • Tender, swollen prostate is warm and firm • Do not massage the prostate b/c can precipitate bacteremia • Treatment with quinolone or Bactrim for 30 days • If urinary drainage needed, suprapubic catheter (not foley)
Penile ulcers • HSV, syphilis, chancroid, granuloma inguinale, lymphogranuloma venereum • Behcet’s syndrome • Vasculitis with chronic oral ulcerations, relapsing iridocyclitis, genital ulcers • May also have polyarthritis and erythema nodosum • Treatment is steroids
Fournier’s gangrene • Necrotizing infection of subq tissue of perineum • Bacteroides fragilis, E coli • Acute onset, toxic • Painful, erythematous, edematous scrotum, +/crepitus/gangrene • Risk– diabetes, chronic steroids, alcoholic, local trauma • Treatment– Abx, urology consult, debridement, hyperbaric oxygen
Balanoposthitis • Inflammation of glans penis (balanitis) and forskin (posthitis) • If recurrent, think diabetes • Retraction of foreskin reveals foul, purulent material • Glans is red, swollen, tender to palpation • Topical antifungal, circumcision, good hygiene, consider anti-strep abx, r/o diabetes
Phimosis • Inability to retract foreskin behind glans • Usually secondary to chronic infection of foreskin • Usually uncircumcised men • Treatment– dorsal slit if difficulty voiding; circumcision
Paraphimosis • Inability to pull retracted foreskin back over glans • Infection, trauma, hair tourniquet, sexual activity • Distal venous congestion can lead to arterial compromise, necrosis, gangrene • Treatment– manual reduction, ice, dorsal slit, circumcision
Penile fracture • Tear of tunica albuginea (usually during erection) • Retrograde urethrogram to r/o urethral injury
Priapism • Low-flow • Decreased venous outflow venous stasis, ischemia of corpus cavernosae but spares glans and corpus spongiosum rigid, painful penile shaft and soft glans • Causes– sickles cell, leukemia, intracavernosal injections of ED, trazodone, marijuana, idiopathic • High-flow • Rare; not a true emergency • Increased arterial blood flow to corpus cavernosae increased venous blood flow partially rigid, painless penile shaft and hard glans • Causes– groin/straddle injury (arterial-cavernosal shunt), high spinal cord injury/lesion • Terbutaline subq, analgesia, pseudoephedrine injection, corporeal aspiration, shunt surgery
Testicular torsion • Bimodal peaks– first few days of life and ages 12 -18 • Predisposition– bell-clapper deformity • Acute onset severe unilateral testicular pain or lower abdominal pain +/- recent history of strenuous physical activity or h/o testicular pain with resolution • Exam done with patient standing– swollen, firm, high-riding testicle with transverse lie; contralateral testicle may also be transverse b/c bell-clapper deformity • No urinary sx • Immediate urology consult • Attempt manual detorsion (opening a book) • Doppler ultrasound • Salvage rate 100% at 6 hrs but approaches 0% at 24 hours
Torsion of appendices epididymis and testis • Unilateral pain, more gradual in onset, not as severe, localized to involved appendix early; late, generalized scrotal swelling and tenderness • Blue dot sign– visualization of necrotic appendix testis through scrotal wall on superior aspect of testicle on transillumination • Self-resolving, benign process • Rest, scrotal elevation, analgesia
Epididymitis • Gradual onset unilateral pain and swelling • Associated fever and dysuria • Tenderness and swelling of epididymis (located posteriorly) • Elevation of testicle relieves pain (Prehn’s sign) • Age <35 • Chlamydia, gonorrhea; ceftriaxone IM and doxy x 10 days • Age >35 • Gram negatives (E coli, Pseudomonas); quinolone 10 -14 days • 3 -11% patients on amiodarone develop epididymitis
Other testicular conditions • Hydrocele • Fluid collection in tunical vaginalis • Transilluminates • Not firm or hard • Varicocele • “bag of worms” • 85 -95% on left • Tumors • Painless, unilateral scrotal mass palpated directly from the testis • Firm and hard