OSSEOINTEGRATION IN ENDOSSEOUS IMPLANTS CONTENTS 1 2 3







 ADAPTIVE OSSEOINTEGRATION § Osseous tissue approximating the surface of the")
 § Tissue integration around healed functioning endosteal dental implant")















 Close adaptation of the regularly")
 Fibroblasts and")







 Threaded or screw design implants § Demonstrated to function for decades")



 “The extent of bone implant interface is positively correlated")


















 /secondary implants (SI) § § § A variant of IFL After")












 Histomorphometric – To know the")

 § § § The individual unattached implant should")









- Slides: 84
OSSEOINTEGRATION IN ENDOSSEOUS IMPLANTS
CONTENTS 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. HISTORICAL BACKGROUND DEFINITIONS AND TERMINOLOGIES MECHANISM OF OSSEOINTEGRATION FIBROOSEUS VERSUS OSSEOINTEGRATION BIOINTEGRATION VERSUS OSSEOINTEGRATION IMPLANT TISSUE INTERFACE FACTORS EFFECTING OSSEOINTEGRATION IMMEDIATE LOADING METHODS TO CHECK OSEOINTEGRATION SUCCESS CRITERIA COMPLICATIONS IN OSSEOINTEGRATED IMPLANTS CONCLUSION BIBLIOGRAPHY
HISTORICAL BACKGROUND
§ 1931 - Mayan civilization - Honduras § 1950 - Chamber of titanium - study blood flow in vivo. § 1952 - Cambridge designed ‘rabbit ear chamber’ used in the rabbit femur. § Dr. Per. Ingvar. Branemark - ‘Osseointegration’. § 1965 - First titanium dental implant - Gösta Larrson.
DEFINITION AND TERMINOLOGIES
OSSEOINTEGRATION § 1969 - “As a direct contact between the bone and metallic implants without interposed soft tissues layers”. § 1977 – “Direct structural and functional connection between ordered, living bone and the surface of a load carrying implant. ”
According to GPT-8 “ the apparent direct attachment or connection of osseous tissue to an inert, alloplastic material without intervening connective tissue”
Meffert et al (1987) ADAPTIVE OSSEOINTEGRATION § Osseous tissue approximating the surface of the implant without apparent soft tissue interface at light microscopic level. BIOINTEGRATION § Is a direct biochemical bone surface attachment confirmed at electron microscopic level.
OSTEOPRESERVATION (STALLARD R. E ) § Tissue integration around healed functioning endosteal dental implant in which the prime load bearing tissue at the interface is a periimplant ligament composed of osteostimulatory collagen. PERIOSTEAL INTEGRATION § Tissue integration around a healed functioning subperiosteal implant in which the load bearing tissue is the sheath of dense collagenous tissue constituting the outer layer of periosteum.
MECHANISM OF OSSEOINTEGRATION
BONE HEALING § Inflammatory phase § Proliferative phase § Maturation phase MUCOPERIOSTEAL HEALING § Inflammatory phase § Proliferative phase § Maturation phase
PHASES OF GENERALIZED BONE HEALING After the surgical placement of implants into endosteal locations , at the traumatised bone around these implants begins the process of wound healing. Phase Timing Specific Occurrence Inflammatory phase Day 1 -10 Adsorption of plasma proteins Platelet aggregation and activation Clotting cascade activation Cytokine release Non-specific cellular inflammatory response Specific cellular inflammatory response Macrophage-mediated inflammation Proliferation phase Day 3 -42 Neovascularization Differentiation, proliferation and activation of cells Production of immature connective tissue matrix Maturation phase After day 28 Remodeling of the immature bone matrix with coupled resorption/ deposition of bone Bone remodeling in response to implant loading Physiologic bone recession
In Normal circumstances Healing of implants Associated with 0. 5 – 1. 5 mm of vertical bone loss (first year) attributed to generalized healing response resulting inevitably due to surgical trauma After this a steady state reached (normal physiologic bone resorption) 0. 1 mm /year
MUCOPERIOSTEAL HEALING Implants are placed into their endosteal position through incisions in the mucoperiosteum. One stage technique Transmucosal portions of the implant heal as a single unit Two staged technique Endosteal component is placed initially followed by the placement of the transmucosal portion after a period of healing.
PHASES OF MUCOPERIOSTEAL HEALING Phase Timing Specific Occurrence Inflammatory Day phase 1 -10 Platelet aggregation and activation Clotting cascade activation Cytokine release Non-specific cellular inflammatory response Macrophage-mediated inflammation Proliferative phase Day 2 - 42 Neovascularization Differentiation, proliferation, and activation of cells Deposition of immature collagen, elastin and ground substance Maturation phase After day Connective tissue remodeling 21
FIBROOSSEOUS RETENTION Vs. OSSEOINTEGRATION
Two basic means of retention of endosteal implants § § Osseointegration Fibroosseous retention Osseointegration development of ankylotic relationship between implant and bone Branemarks theory of osseointegration (1982) Advocates ……
Fibroosseous retention development of an intermediate ligamental system Weiss theory of fibroosseous integration A connective tissue structure is formed between the implant and the bone Jahn-First described it as a Hammock like suspensory ligament Weiss interprets it as a peri-implant membrane with an osteogenic effect
He believes collagen fibers originate from trabeculae of cancellous bone on one side, weave around the implant, reinserting into the implant on opposite side. When function is applied to implant, tension is applied to fibers, forces closest to implant cause compression of fibers close to implant and those away – corresponding tension. This difference results in Bioelectric Current Induces differentiation of CT into components required for maintenance of bone. Therefore the premise of fibers being osteogenic. Advocates…….
OSSEOINTEGRATION VS. BIOINTEGRATION
1985 – Putter etal observed 2 ways of implant anchorage § Mechanical § Bioactive
Bioactive Mechanical Achieved with bioactive materials such as hydroxyapatite Titanium / Ti alloys Retention based on undercut forms such as slots, vents, screws etc. Direct contact between the dioxide layer. E. g. the base metal and bone with no chemical bonding Retention depends on surface area. Surface area contact Bond directly to bone Bone matrix deposited on HA layer due to physiochemical interaction, between collagen of bone and HA crystals of implant Plasma spraying/ ion sputter Two techniques use to coat implant with HA
Implant Tissue Interface
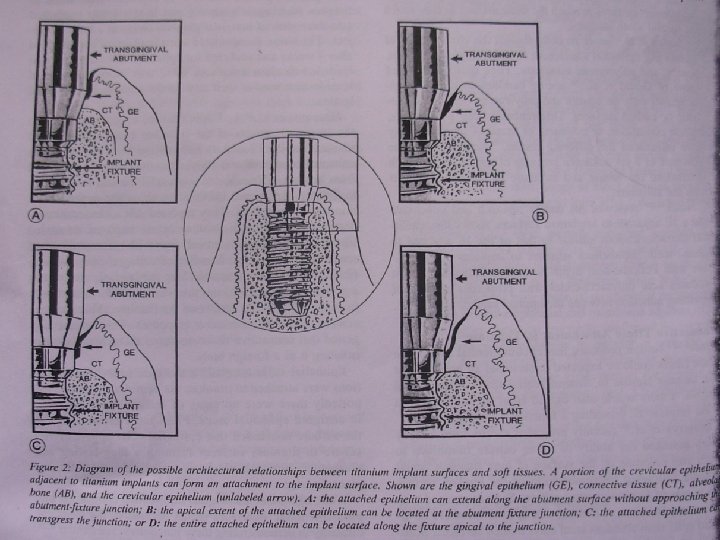
§ § § Implant – CT Interface Implant – Epithelium Interface Implant – Bone Interface
IMPLANT AND BONE INTERFACE Light microscopic level (100 X) Close adaptation of the regularly organized bone next to the Ti implants. Scanning electron microscopic level Parallel alignment of the lamellae of haversian system of the bone next to the Ti implants. No connective tissue or dead space at the interface. Ultramicroscopic(500 to 1000 X) level Amorphous coat of glycoproteins on the implants to which the collagen fibers are arranged at right angles and are partly embedded into the glycoprotein layer.
Mechanism of Attachment Cells binds to each other Glycoproteins Tri-peptides arginineglycinasperticacid (RGD) Fibroblasts and other connective tissue cells Binding elements Integrins recognizes the RGD’s and binds them
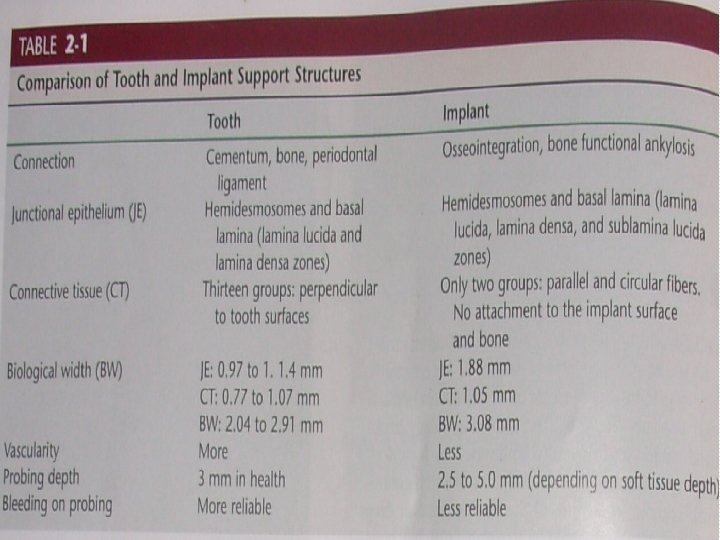
IMPLANT CONNECTIVE TISSUE INTERFACE Supracrestal connective tissue fibers will be arranged parallel to the surface of the implant § Not as strong as that of the connective tissue and tooth interface. § An implant has no connective tissue fibers in the connective tissue zone that insert into the implant.
Implant Epithelial Interface “Biologic seal” Hemidesmosomes attached to glycoprotein layer Connect the interface to the plasma membrane of the epithelial cells Similar to the junctional epithelium, Sulcus depth varies from 3 to 4 mm
FACTORS EFFECTING OSSEOINTEGRATION
Six different factors known to be important for the establishment of a reliable, long-term osseous anchorage of an implanted device § Implant biocompatibility § Design characteristics § Surface characteristics § State of the host bed § Surgical technique and § Loading conditions
Implant Biocompatibility Response of bone to different implant material is the principal factor on which an implant material is selected as suitable or unsuitable for osseointegration § Chemical interaction determined – properties of surface oxide Commercially pure (c. p. ) Titanium and Titanium alloy (Ti -6 AL 4 V) § Documented long term function § Covered with adherent, self- reparing oxide layer § Excellent resistance to corrosion – high dielectric constant § Load bearing capacity
§ The mechanical properties of Titanium alloy are superior to C. P-Titanium Other metals § Niobium, tantalum § Cobalt chrome molybdenum alloys § Stainless steels § Ceramics - calcium phosphate hydroxyapatite (HA) and various types of aluminium oxides Biocompatible - insufficient documentation and very less clinical trials - less commonly used.
Grouping of hard tissue replacement materials according to their compatibility to bony tissue Degree of Compatibility Characteristics of Reactions of Bony Tissue Materials Biotolerant Implants separated from adjacent bone by a soft tissue layer along most of the interface: distance osteogenesis Stainless steels: Co. Cr. Mo and Co. Cr. Mo. Ni alloys Bioinert Direct contact to bony Alumina ceramics, tissue contact zirconia ceramics, osteogenesis titanium, tantalum, niobium, carbon. Bioactive Bonding to bony tissue: bonding osteogenesis Calcium phosphatecontaining glasses, glass-ceramics, titanium (? )
Implant Design (Macrostructure) Threaded or screw design implants § Demonstrated to function for decades without clinical problems. § Provide more functional area for stress distribution than the cylindrical implants. § Minimal - <0. 2 mm/year bone loss Cylindrical implants § Press fit root form implants depend on coating or surface condition to provide microscopic retention and bonding to the bone § Bone saucerization ? Combination root forms § Macroscopic features of cylinder and screw root forms
The design of the threads The dental implant applications dictate the need for a thread shape optimized for long term function , load transmission under occlusal , intrusive and shear loading Functional surface area per unit length of implant may be modified by the thread geometry parameters • Thread shape • Thread pitch • Thread depth
• Square thread Optimized surface area for intrusive and compressive loads Shear force 10 times lesser than Vshape • Decreased thread pitch increases the functional surface area • The greater the thread depth the greater the surface area of the implant , if all factors are equal A wider diameter , more threads , deeper threads and surface structure that increase the initial bone contact percentage are of great benefit. Alterations in these are suggested according to Bone density.
Grooves on implants. Groovy on the collar too! Grooves on the threads of all implants and on the collars, whereever appropriate. § Increase surface area § Increase area for bone-to-implant contact
Implant Surface (Microstructure, Surface Topography) “The extent of bone implant interface is positively correlated with an increasing roughness of the implant surface” Roughened surface § Greater bone to implant contact at histological level § Micro irregularities - cellular adhesion. § High surface energy - improved cellular attachment.
Methods § Electroploishing § Sand blasting and acid attack § Titanium plasma spraying THE TITANIUM WITH HIGHEST BONE TO IMPLANT CONTACT WAS CREATED WITH LARGE GRIT BALATING AND ACID ATTACK. THIS SURFACE GAVE SIMILAR BONE TO IMPLANT CONTACT AS DID IMPLANTS COATED WITH HYDROXY APATITE.
SURFACE COATINGS Two materials plasma sprayed onto implant body § Titanium § Hydroxyapatite Advantages of TPS § Increased surface area § Increased roughness for initial stability § Stronger bone to implant interface Advantages of Hydroxyapatite on TPS § Faster healing bone interface § Stronger interface than TPS § Less corrosion of metal
State of the Host Bed Ideal host bed Healthy and with an adequate bone stock § BONE HEIGHT § BONE WIDTH § BONE LENGTH § BONE DENSITY Undesirable host bed states for implantation § PREVIOUS IRRADIATION § RIDGE HEIGHT RESORPTION § OSTEOPOROSIS
§ 10 -15% poorer clinical results must be anticipated after a therapeutic dose of irradiation - vascular damage, at least in part. § Such clinical states may constitute an indication for ridge augmentation with bone grafts. § As stated by Branemark et al and Misch, the bones with D 1 and D 2 bone densities shows good initial stability and better osseointegration. SELECT SUITABLE IMPLANTS DEPENDING ON THE QUALITY AND QUANTITY OF AVAILABLE BONE
Surgical Considerations The main aim of the careful surgical preparation of the implant bed is to promote regenerative type of the bone healing rather than reparative type of the bone healing. § The critical time/ temperature - bone tissue necrosis 47° for one minute.
Recommendations by Erickson R. A. § Slow speed § Graded series § Adequate cooling § Overheating avoided § Bone cutting speed of less than 2000 rpm § Tapping at a speed of 15 rpm with irrigation § Using sharp drills
The surgical preparation sequences as well as the instruments depend upon the quality of the bone. Number of drills used to prepare implant osteotomy corresponds to bone density § D 1 uses six drills and D 3 uses four Drills § D 4 uses osteotomes trabecular bone. § Bone taps are used for D 1 and D 2 bone. § Countersink drill is optional in D 3 bone to compact fine
Power used at implant insertion § § Too strong a hand will use in bone tension and a resorption response will be stimulated. Holding power of the implant will fall to dangerous levels after a strong insertion torque. § A moderate power at the screwing home of an implant is therefore recommended. § The optimal torque threshold – 35 N/cm. § Implant should gently engage the bone in order to avoid too much pressure at the bone interface which could jeopardize healing
Surgical fit of the fixture § The accurate fit consists of more surface contact, less dead space and thus better healing.
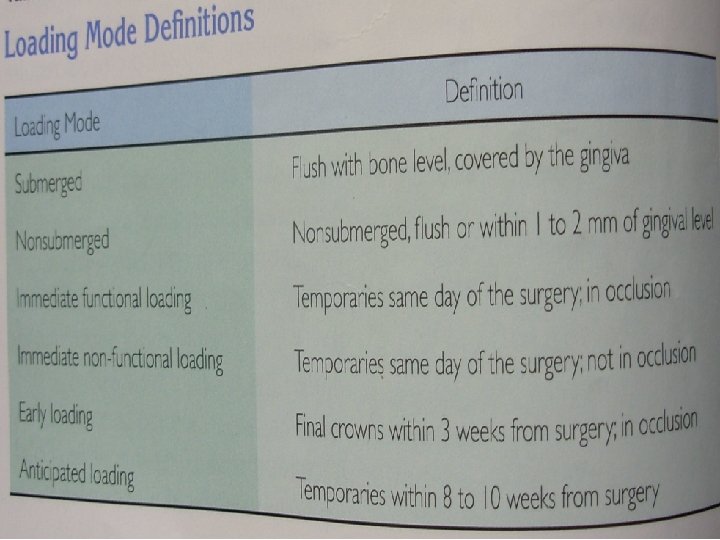
Loading Conditions § § Progressive or two stage loading Immediate or one stage or nonsubmerged loading
Progressive or two stage loading Branemark etal to accomplish osseointegration considered the following prerequisites § Countersinking the implant below the crestal bone § Obtaining and maintaining a soft tissue covering over the implant for 3 to 6 months § Maintaining a nonloaded implant environment for 3 to 6 months
Elements of progressive loading § § § Time interval Diet Occlusal material Occlusal contacts Prosthesis design
TIME The healing time between the initial and second stage surgeries for § § § D 1 and D 2 is similar – 3 to 6 months D 3 and D 4 – 5 to 6 months 3 month loading delay in the mandible and a 4 -6 month delay in the healthy maxillary bone - more cancellous in character.
DIET The dentist controls diet of the patient to prevent overloading. § Initial healing phase- avoid chewing in the area. § Initial transitional prosthesis to final prosthesis – soft diet § After evaluation of final prosthesis function, occlusion and cementation - normal diet.
OCCLUSION § § Initial healing – no occlusal contacts First transitional prosthesis left out of occlusion in partially edentulous patients No occlusal contacts on cantilevers Final restoration - implant protective occlusion concepts.
The salient features of Branemark and his team’s work § § § About more than 50 designs of Ti screws (implants) were tested and used. The surgical protocol followed was: two stage surgery, which was proved beneficial. Minimal trauma during the surgery results in bone regeneration rather than bone repair at the implant site. Non-contaminated implants (sterile and clean implants) prove good integration. Prosthesis and abutments were screw attached for more technical flexibility. There were more mechanical failures at the interface rather than biological failures.
IMMEDIATE LOADING Non submerged one stage healing § Loads the implant with a provisional restoration at the same appointment or shortly thereafter. Rationale § Reduces the risk of fibrous tissue formation § Minimizes woven bone formation § Promotes lamellar bone maturation to sustain occlusal load § Enhances bone remodeling § Increased bone density §
3557 Immediate Functional and Non Functional loading of dental implants: a clinical study of 646 titanium implants M. DEGIDI, M. PIATTELLI, G. PETRONE, and A. PIATTELLI, University of Chieti, Italy, J PERODONTOLOGY 2003 The aim of this study was the evaluation, from a clinical point of view, of implants subjected to immediate functional loading (IFL) and to immediate non-functional loading (INFL) in various anatomical configurations. § Whenever esthetic , psychological or functional conditions allow it , second stage surgery is no longer necessary. § In totally edentulous patient- IFL - reliable. § Partially edentulous – adequate bone quality and quantity available- INFL brings together the advantages of IFL while reducing the biomechanical risks to a minimum. § Careful patient selection remains , in any case important.
Primary implants (PI) /secondary implants (SI) § § § A variant of IFL After the placement of all the necessary implants , some 3 or 4 implants are used to support the fixed prosthesis during the healing period- secondary implants They are meant to support the temporary prosthesis until the other primary implants have completely osseointegrated If impaired osseointegration – eliminated / reassessment to include in the final prosthesis. Commonly used in totally edentulous jaw
Questions related to immediate loading Optimal time interval between surgery and prosthetic delivery? § Prosthesis given the same day of surgery, delaying by few days exposes the patient to unpleasant experience of post operative swelling. Which technique for partial /total edentulism? § IFL - totally edentulous; INFL – partial and single tooth replacements
Optimal or minimum ratio between the number of prosthetic units and the number of implants? § PU/I – 1; should not exceed 1. 4 in maxilla and 1. 5 in mandible , independently of IFL and INFL implants. § High PU/I bending and flexure of the interim prosthesis at the implant interface and fibrous encapsulation. § Avoid long span bridges, rigid metallic abutments; use metallic reinforcement to the provisional prosthesis; decrease when possible the clinical crown height; avoid occlusal contacts in parafunctions; avoid cantilevers micromovement
Should the immediately loaded provisional prosthesis only acrylic or should it have metallic reinforcement? screw retained or cemented? § Screw retained preferred – rigidity; easier § Low PU/I – reduces the flexibility of the temporaries § High PU/I - metal reinforcement to decrease the bending of the temporary structure could be of some help.
Is there an ideal abutment? § § Does not exist. Should present the rigidity of an titanium abutment, but should be able to be prepared like an acrylic abutment. Cost effective Have an internal screw of sufficient length or design to prevent screw loosening during the healing period.
Long term outlook for implant bone interface? § Clinical and radiographic results show that immediately loaded implants remain osseointegrated for long periods(5 years)
Immediate loading versus immediate provisionilazation of maxillary single tooth repalcements –A prospective randomized trial with Biocomp implants J oral maxilofacial surg 2006 § No significant differences in radiographic bone loss and gingival esthetics were found between Immediate non loaded provisionilazation and immediate loaded Biocomp implants in the maxilla.
Immediate loading of root form implants : two case reports 3 years after loading Int J Periodont rest dent 1998 § For a distinct population , immediate loading of multiple splinted implants may prove to be a valuable adjunct to therapy. § The threshold of micromovement is not exceeded with immediately loaded and splinted implants. § A fixed temporary restoration improves chewing, esthetics comfort and self esteem during healing phase.
Endopore dental implant The Endopore dental implant incorporates a unique, truncated cone-shaped design that uses a multilayered porous surface geometry over most of its length to achieve integration by threedimensional bone ingrowth.
Endopore's surgical Advantages § § § § A secure, three-dimensional interlocking interface with bone Predictable and minimal crestal bone remodeling Greater surgical options with shorter implant lengths Uncomplicated surgical sequence Minimal instrumentation and inventory Self seating , tapered, pressfit, prosthetically friendly design Good resistance to torsional forces Shorter initial healing time.
Methods of Evaluation of Osseointegration
Implant stability § § § Stability is a requisite characteristic of osseointegration. When an implant is placed surgically, initial stability is a function of the bone quality, implant deign and surgical technique. Implant placed in the dense cortical bone should have higher initial stability than in a weak cancellous bone During the osseointegration healing and maturation process , the initial stability changes with increases in bone- to –implant contact and osseous remodeling. It is unknown however what precisely constitutes “adequate stability” to warrant proceeding with restoration
Rigid fixation § § § Absence of observed clinical mobility. Two terms osseointegration and rigid fixation are interchangeably used. First clinical criterion to be evaluated. A healthy implant moves less than 73 microns – appears as zero clinical mobility. The goal for root form implants should be rigid fixation and IM status 0
Invasive Methods § § Histological sections (10 microns sections) Histomorphometric – To know the percentage of bone contact Transmission electron microscopy By using Torque gauges
Non-Invasive Methods Percussion test § Tapping with a metallic instruments The fixture produces ringing sound- osseointegrated. Dull sound - fibrous integration. § Radiographs § Perio-test Checks mobility and damping system. Normal values - 5 to +5 PTV § Dynamic modal testing § Resonance frequency analysis § Impulse testing § Implatest §
The Success Criteria (Alberktsson et al) § § § The individual unattached implant should be immobile when tested clinically. The radiographic evaluation should not show any evidence of radiolucency. The vertical bone loss around the fixtures should be less than 0. 2 mm per year after first year of implant loading. The implant should not show any signs of pain, infection, neuropathies, parasthesia, violation of mandible canals and sinus drainage. The success rate of 85% at the end of 5 year and 80% at the end of 10 years
According to Misch
COMPLICATIONS IN OSSEOINTEGRATED IMPLANTS
POTENTIAL PROSTHODONTIC COMPLICATIONS Improper implant placement § Abutment screw fracture § Framework fracture § Esthetics § Speech § Gingival complications § Peri implantitis Successful reconstruction , however means more than successful integration. Predetermination of the framework design, the components to be used, and esthetic and speech requirements will ensure a more predictable prosthodontic reconstruction. §
CONCLUSION
§ Long term successful prosthodontic rehabilitation requires prosthodontists to be analytical , critical and follow a sequential line of rehabilitation therapy. § As the concept of osseointegration has developed and spread globally , it has had a dramatic impact on the practices of dentistry. § In implant dentistry , an undisturbed healing period is always required to ensure osseointegration. § A modified protocol with early or immediate loading has been tested to satisfy the demand of more rapid treatment and to reduce discomfort of wearing removable appliances during the healing period. § Provided that the implant has primary stability , studies have shown that the survival of loaded implants can be analogous to the unloaded protocol. Therefore we need to empower ourselves and keep pace with the progress that is happening at rocketing speed in dental implants !!
BIBLIOGRAPHY 1. 2. 3. 4. 5. 6. 7. Branemark Per Ingvar 1983 “Osseointegration and its experimental background. ” Journal of Prosthetic Dentistry; 50(3): 399 -407. Degidi and Piatelli 2003 “Immediate Functional and Non Functional loading of dental implants. ” Journal of Periodontology; 74: 225 -241. Donley G. Timothy and Gillette B. William 1991 “Titanium Endosseous Implant – Soft tissue interface. A literature review. ” Journal of Periodontol; 62: 153 -160. Jensen Ole 1989 “Site classification for the osseointegrated implants. ” Journal of Prosthetic Dentistry; 61(1): 229 -234. Kasemo B. 1983 “Biocompatibility of Titanium implants surface science aspect. ” Journal of Prosthetic Dentistry; 49(6): 833 -836. David. L. Cochran. Comparison of endosseous implants surfaces. Journal of Periodontol; 1999; 1523 -29 Doglass. A. Depoerter. simplifying treatment of edentulism. JADA ; 127 ; 1996
8. 9. 10. 11. 12. 13. 14. 15. Krogh H. J. Paul and Collins A. Thomas 1994 “Complications of osseointegrated implants. Oral and Maxillofacial Surgery Clinics of North America; 6(4): 837 -858. Misch Carl E. Contemporary Implant Dentistry, 2 nd Edition, Mosby Publication. Philips Science of Dental Materials, 11 th Edition, Anusavice Saunders. Sahin Samie and Akagawa Yasumasa 1996 “The three dimensional bone interface of an osseointegrated implant II – a morphometric evaluation after 3 months loading. ” Journal of Prosthetic Dentistry; 76: 176 -180. Sones D. Amerian 1989 “Complications with osseointegrated implants. ” Journal of Prosthetic Dentistry; 62(5): 581 -585. Tomas Allbrektsson 1983 “Direct bone anchorage of dental implants. ” Journal of Prosthetic Dentistry; 50(2) : 225 -260 Shalak Richard 1983 “Biomechanical considerations in osseointegrated prosthesis. ” Journal of Prosthetic Dentistry; 49(6): 843 -848. Electronicaly monitoring dental implant osseointegration. JADA vol 133 , April 2002
16. 17. 18. 19. Zarb A. George and Smith E. Dale 1989 “Criteria for success of osseointegrated endosseous implants. ” Journal of Prosthetic Dentistry; 62(5): 567 -572. Immediate loading versus immediate provisionilazation of maxillary single tooth repalcements –A prospective randomized trial with Biocomp implants. j oral maxilofacial surg 2006 3557 Immediate Functional and Non Functional loading of dental implants: a clinical study of 646 titanium implants. J Perodontology 2003 Immediate loading of root form implants : two case reports 3 years after loading. Int J Periodont Rest Dent 1998
THANK YOU