MISURE DI PREVENZIONE E CONTROLLO DELLA DIFFUSIONE DI

 delle strutture ospedaliere censite ha inviato")

 • isolamento da contatto in stanza")




















 baths (4% liquid formulation) • Decrease in central")




, AND ENVIRONMENTAL (BED RAIL, BEDSIDE TABLE, CALL")



 in patients")



- Slides: 46
MISURE DI PREVENZIONE E CONTROLLO DELLA DIFFUSIONE DI C. DIFFICILE NELLE STRUTTURE ASSISTENZIALI ADRIANA CATALDO DIPARTIMENTO CLINICO E DI RICERCA INMI
• Nella regione Lazio il 74% (91/123) delle strutture ospedaliere censite ha inviato i questionari compilati. • Misure di isolamento dei pazienti con CDI sospetta o accertata
IGIENE DELLE MANI • Il 24% delle strutture possiede stanze dedicate alla degenza dei pazienti dotate di “antistanza” ove effettuare l’igiene delle mani e indossare i dispositivi di protezione individuali • Nelle strutture non dotate di antistanza, l’igiene delle mani viene effettuata – presso la medicheria 40% – nel bagno della stanza di degenza 15% – dispenser per l’igiene delle mani senz’acqua posizionati in prossimità dell’ingresso delle stanze o su appositi carrelli 13%
PROVVEDIMENTI INTRAPRESI NEL PAZIENTE CON DIARREA (CDI SOSPETTA) • isolamento da contatto in stanza singola con servizio igienico: 35%; • nessuno, si attende il risultato del test per C. difficile: 26%; • isolamento da contatto in stanza condivisa con altri pazienti (non necessariamente con diarrea), con servizi igienici in comune 21%; • isolamento da contatto in stanza condivisa con altri pazienti (non necessariamente con diarrea), con servizi igienici in comune e servizi igienici dedicati al paziente con diarrea: 15%; • isolamento da contatto in stanza singola senza servizio igienico: 2%.
PROVVEDIMENTI INTRAPRESI NEL PAZIENTE CON CDI • Isolamento da contatto in stanza singola con servizio igienico: 77%; • Isolamento da contatto in stanza condivisa con altri pazienti (non necessariamente con diarrea da C. difficile), con servizi igienici in comune: 9%; • Isolamento da contatto in stanza condivisa con altri pazienti (non necessariamente con diarrea da C. difficile), con servizi igienici dedicati al paziente con diarrea: 8%; • Isolamento da contatto in stanza singola senza servizio igienico: 4%; • Isolamento da contatto in stanza dedicata con altri pazienti con infezione da C. difficile (coorte): 2%. • • Solo nel 56% delle strutture l’isolamento è segnalato sulla porta di ingresso della stanza di degenza.
PROVVEDIMENTI INTRAPRESI NEL PAZIENTE CON CDI • “Nell’impossibilità di ricovero in stanza singola, quali provvedimenti vengono intrapresi per il paziente con accertata infezione da C. difficile? ” • 49% il paziente viene ricoverato in camera con altri degenti senza CDI, ma in isolamento da contatto di tipo “funzionale” • 33% in coorte con malati con CDI • solo il 6% delle strutture ha dichiarato che la necessità di ricoverare un paziente con CDI accertata in stanza condivisa con altri pazienti non sussiste mai.
TRASMISSIONE • Clostridium difficile è presente – nell’ambiente – nella microflora dell’intestino (adulti 3%, neonati 70%) che ne controlla la crescita • In condizioni ambientali sfavorevoli (ph fortemente acido, temperature elevate, carenza di nutrienti) la forma vegetativa si trasforma in spora § La forma vegetativa sopravvive fino a 24 h in presenza di O 2 § Le spore sopravvivono fino a 2 anni in presenza di O 2 e sono molto resistenti a calore, radiazioni, essiccamento, composti chimici vari
TRASMISSIONE • CD entra in contatto con il nostro organismo attraverso l’ingestione di spore presenti nell’ambiente esterno (via oro-fecale) • Toccando con le mani le superfici contaminate le spore vengono ingerite, raggiungono l’apparato gastro-intestinale e per all’ambiente fortemente acido (acidi biliari) germinano nella forma vegetativa
Weber. DJ et al. Am J Infect Control 2010; 38: S 25 -33
TRASMISSIONE • Reservoirs di C. difficile in ambiente nosocomiale sono i pazienti con CD (sintomatici e asintomtici) e gli oggetti • Pazienti con CDI sintomatica sono il reservoir principale • I pazienti colonizzati sono una potenziale fonte di contaminazione • Le mani degli operatori sanitari, ambiente contaminato e strumenti medicali sono un’importante veicolo di trasmissione
ENVIRONMENTAL CONTAMINATION Sample patient room identifying high touch surfaces • The level of environmental contamination with C. difficile spores increases with increasing severity of disease
• Aerosolization of C. difficile occurs commonly but sporadically in patients with symptomatic. CDI. • We detected airborne C. difficile most commonly during periods of activity, particularly around the busy lunchtime period. • Activities known to liberate particles into the air, such as bed making and curtain drawing, as well as contact with these items may contribute to the spread and C. difficile. Line indicating the total number of Clostridium difficile colonies recovered at various times throughout the day (total of 10 patients tested aerosolization of for 2 days). The number of patients the colonies were isolated from is indicated in parentheses. Best LM et al. Clinical Infectious Diseases 2010; 50(11): 1450– 1457
LINEE GUIDA
SORVEGLIANZA
ISOLAMENTO DA CONTATTO • Hospital room design and handwashing accessibility are essential elements in the prevention and control of CDI. • Private rooms may facilitate better infection control practices • Significant reduction in CDI rates by 43%, was reported after an ICU was renovated to only private rooms with accessible handwashing facilities • Cohort study of healthcare-associated CDI acquisition: – higher rates of CDI among patients housed in double rooms than in single rooms (17% vs 7%; P =. 08) – significantly higher risk of acquisition after exposure to a roommate with a positive culture result
HOSPITALS WITH A LIMITED NUMBER OF SINGLE ROOMS • CDI patients with stool incontinence should be prioritized for placement in single rooms. • Cohort patients with CDI in a multibed room — do not cohort patients with CDI who are discordant for other multidrug-resistant organisms Risk of recurrence examined among CDI patients admitted to a cohort (adjusting for potential risk factors) : Admission to a C. difficile cohort ward was shown to be an independent predictor for recurrence If cohorting is required, dedicated commodes should be provided to the patients to reduce further cross-transmission.
PRECAUZIONI DA CONTATTO
USO DEI GUANTI • Wearing gloves should decrease the concentration of C. difficile organisms on the hands of healthcare personnel. • trial of vinyl glove use for handling body substances: decrease in CDI rates, from 7. 7 to 1. 5 cases per 1000 discharges (before and after institution of glove use) – No decrease on control wards that did not institute the glove intervention • Care should also be taken to prevent contamination of hands when removing gloves.
CAMICI MONOUSO • Clostridium difficile has been detected on nursing uniforms • Use of gowns recommended because of potential soiling and contamination of the uniforms of healthcare personnel with C. difficile • High quality of evidence for reducing transmission of other enteric multidrug-resistant organisms • The fact that gloves reduce transmission provides further indirect evidence for gowns.
HAND HYGIENE • C. difficile spores are highly resistant to killing by alcohol • Addition of ethanol to stool samples in the laboratory facilitates the culture of C. difficile from these specimens • Healthcare personnel whose hands become contaminated may be merely redistributing spores over the hand surface when using alcohol-based products • Numerous studies have not shown an association between the use of alcohol-based hand hygiene products and an increased incidence of CDI
HAND HYGIENE • Handwashing with soap and water, or with an antimicrobial soap and water: more effective at removing C. difficile spores than alcohol-based hand hygiene products • Chlorhexidine-containing antiseptic more effective than plain soap for eliminating C. difficile from hands • C. difficile was recovered from the hands of 88% of personnel (14 of 16) who had washed with plain soap. • Washing with 4% chlorhexidine gluconate reduced the rate to 14% (1 of 7 personnel) • Another study showed no difference between plain soap and chlorhexidine gluconate in removing C. difficile from hands
• Hands of patients can also become contaminated with C. difficile at a rate of 32% • These patients can transmit C. difficile to surfaces • This could be a factor in CDI recurrence when the spores are ingested from their contaminated hands • Patient bathing can also decrease skin contamination of C. difficile • Among 37 patients with CDI, showering was more effective than bed bathing in decreasing the rate of positive skin cultures • Encouraging patients to wash hands and shower could be a useful strategy to reduce the burden of spores on the skin.
Information provided to patients should include: • Explanation of the infection • Discuss how the organism is spread, including skin contamination, colonization, shedding, and environmental contamination and how to prevent transmission of C. difficile • Describe what the patient can do to help reduce the spread of the disease, including performance of patient hand hygiene • Discuss the importance of both hand hygiene and showering to reduce the bioburden of C. difficile on their skin. • Nursing staff should assist the patient if the patient is unable to perform hand hygiene. This is especially important before eating • Educate the patient and their family about visitors who may be at high risk for acquiring C. difficile and help them make a decision about their visitation.
• The family should understand that items that have been in the patient’s room should not be taken to common waiting room areas because they may be contaminated with spores. • Identify steps that patients and family can do to clean their environment at home including not sharing towels or hygiene products, cleaning, and laundry practices.
PATIENT BATHING • Chlorhexidine gluconate (CHG) baths (4% liquid formulation) • Decrease in central line–associated blood stream infections (CLABSIs) and a decrease in MDROs including C. difficile. • The antimicrobial CHG soap kills the vegetative cells, and the soap and water removes the spores Rupp ME, et al. Infections. Infect Control Hosp Epidemiol 2012
• Environmental contamination has been associated with the spread of C. difficile via contaminated commodes, blood pressure cuffs, and oral and rectal electronic thermometers • Replacement of electronic thermometers with single-use disposable thermometers has been associated with significant decreases in CDI incidence • Stethoscopes were found to acquire and transfer C. difficile spores as often as gloved hands • It is important to ensure that the responsibility and methods for cleaning and disinfection are clearly defined in standard operating procedures.
• Acquisition of Clostridium difficile on gloved hands after contact with skin of patients with C. difficile infection and environmental surfaces in their rooms at the time of the order for testing versus • Acquisition after availability of stool testing results. The skin sites contacted included the patient’s chest and abdomen and their arm and hand. The environmental sites contacted included the call button and telephone and the bed rail and bedside table. Venkata C. K. Sunkesula et al. Infect Control Hosp Epidemiol 2013; 34(3): 306 -308
QUANDO INTERROMPERE L’ISOLAMENTO DA CONTATTO • CDC recommends that contact precautions be continued for the duration of the illness • UK guidelines recommend continuing contact precautions for at least 48 hours after diarrhea resolves • There are no studies that demonstrate further extending contact precautions results in reductions in CDI incidence
• Fifty-two patients with CDI • C. difficile was suppressed to undetectable levels in stool samples from most patients during treatment • 1– 4 weeks after treatment, 56% of patients who had samples tested were asymptomatic carriers of C. difficile. Sethi AK et al. Infect Control Hosp Epidemiol 2010; 31: 21 -27
PERCENTAGE OF STOOL, SKIN (CHEST AND ABDOMEN), AND ENVIRONMENTAL (BED RAIL, BEDSIDE TABLE, CALL BUTTON, TOILET SEAT) CULTURES POSITIVE FOR C. DIFFICILE Sethi AK et al. Infect Control Hosp Epidemiol 2010; 31: 21 -27
PATIENT RISK FACTORS FOR INITIAL AND RECURRENT CLOSTRIDIUM DIFFICILE INFECTION. De. Pestel DDet al. Journal of Pharmacy Practice 2013 26: 464
RISK FACTORS: PPI • Use of acid suppression therapy, in particular PPIs as a risk factor is still controversial. • 2 meta-analyses suggest increased risk of CDI with PPI use • Janarthanan et al (Am J Gastroenterol. 2012): PPI use associated with a 65% increased risk of CDI • Deshpande et al (Clin gastroent and epatology 2012): PPI therapy increased the risk for CDI (odds ratio, 2. 15, 95% confidence interval, 1. 81– 2. 55) • Significant heterogeneity in results among studies • H 2 antagonists also found to be associated with CDI but as not as high a risk as PPIs
• Literature from their inception to December 2016 without restriction of language. • All controlled observational studies examining the association between acid suppressive therapy and CDI • RESULTS: • Pooled analysis: significant association between PPI use and risk of developing CDI, OR 1. 26, (1. 12 -1. 39) as compared with non-users. • RR of hospital-acquired CDI and community-associated CDI were 1. 29(1. 14 -1. 44) and 1. 17(0. 74 -1. 59). • The relative risks of hospital-acquired CDI in ICUs and general wards were 1. 43(0. 742. 11) and 1. 29(1. 13 -1. 45).
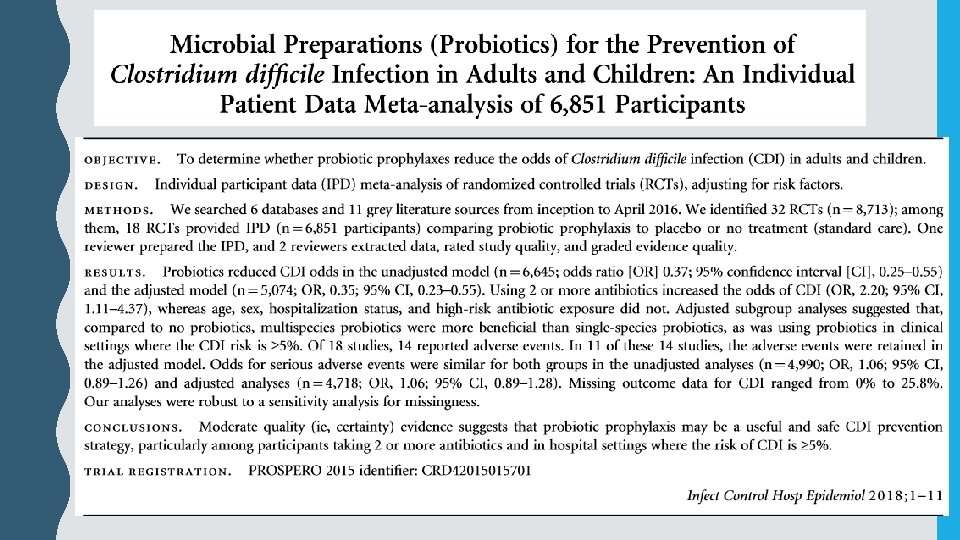
PROBIOTICI • Cochrane review assessed the incidence of CD associated diarrhea (CDAD) in patients • taking antibiotics • CDAD heterogeneous condition based on the definitions reported by authors in the included studies • overall pooled results showed that the incidence of CDAD was significantly lower in the group of patients taking probiotics during antibiotic treatment (2. 0%) as compared to patients taking placebo or no treatment (5. 5%; RR 0. 36; 95% CI 0. 26 to • 0. 51) • Analysis of studies that reported CDI incidence, the overall pooled results did not show a statistically significant reduction (incidence 12. 6% versus 12. 7% in the probiotics and control group, respectively; RR 0. 89; 95% CI 0. 64 to 1. 24) • authors concluded that the short-term use of probiotics appears to be safe and effective when used along with antibiotics in patients who are not immunocompromised or severely debilitated; the quality of evidence. Goldenberg was moderate. JZ, et al. Cochrane Database Syst Rev.
PROBIOTICI • Meta-analysis including randomized studies assessing primary prevention of CDI with probiotics according to the formulation of probiotic used. • 3 studies assessing the use of formulation of L. acidophilus and L. casei: overall protective effect against CDI; • 4 studies assessing the use of formulation of S. boulardii showed no significant difference in CDI rates Johnson S, Int J Infect Dis. 2012