FETAL ALCOHOL SPECTRUM DISORDER FASD UPDATE AND FUTURE
: UPDATE AND FUTURE DIRECTIONS ¡ Dina E. Hill, Ph.")

 populations.")
 FASDs are a group of conditions that can occur")





 – Surveillance for FASD in Midwestern")




 With or without documented prenatal alcohol exposure")


















































 ¡ Enhances child’s capacity to regulate")






















 ¡ Perseverance (determined, committed) ¡ Friendly/trusting, affectionate ¡")












 ¡ Functional Magnetic Resonance Imaging (f. MRI)")

")
 ¡ Spatial Working Memory ¡ Inhibitory Control ¡")



 66 -NOFAS;")


- Slides: 114
FETAL ALCOHOL SPECTRUM DISORDER (FASD): UPDATE AND FUTURE DIRECTIONS ¡ Dina E. Hill, Ph. D. (dhill@salud. unm. edu) ¡ Cynthia King, MD (cyking@salud. unm. edu) Department of Psychiatry, University of New Mexico, School of Medicine
DISCLOSURES ¡ ¡ Dr. Hill has a contract with IHS for neuropsychological assessment of children through her private practice. Dr. King has no financial relationships or conflicts of interest related to this presentation. She is not involved in any clinical drug trials.
GOALS/OBJECTIVES Define FASD, including its relevance to American Indian and Alaska Native (AI/AN) populations. ¡ Describe best practices in FASD for screening and diagnosis. ¡ Describe best practices in FASD for assessment and therapeutic interventions over the lifespan. ¡ Describe factors that contribute to resiliency. Describe what some AI/AN groups are doing to support and help develop resiliency in children, caregivers, community members, medical providers, educators, and others interacting with individuals with FASD. ¡
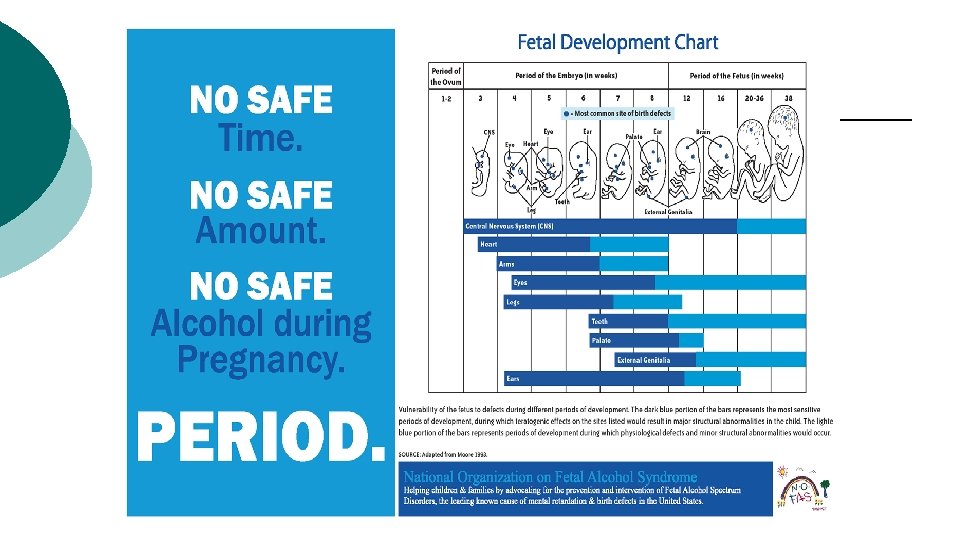
Fetal Alcohol Spectrum Disorders (FASD) FASDs are a group of conditions that can occur in a person whose mother drank alcohol during pregnancy. These conditions can affect each person in different ways, and can range from mild to severe. They can include physical problems and problems with behavior and learning. (CDC)
Fetal Alcohol Spectrum Disorders Institute of Medicine* – 4 categories l FAS – Fetal Alcohol Syndrome l PFAS –Partial Fetal Alcohol Syndrome l ARBD – Alcohol-Related Birth Defects l ARND – Alcohol-Related Neuro-developmental Disorder *Hoyme, et al. , (2016). Updated clinical guidelines for diagnosing fetal alcohol spectrum disorder. Pediatrics: 138, 1 -18.
History of FASD ¡ ¡ It has been known for centuries that alcohol causes problems for the fetus Late 1800 s mothers, who were inmates in the UK, were observed drinking and had poor pregnancy outcomes Lemoine (France -1968): described 127 babies born to drinking mothers Jones & Smith (1973): coined the term FAS
Epidemiology: Rates of Alcohol Use among Women of Childbearing Age CDC 2015 Morbidity and Mortality Report ¡ ¡ Non-pregnant women l Any Alcohol Use = 54% l Binge Drinking (4 or more) = 18% Pregnant women l Any Alcohol Use = 10% (1 in 10 consuming alcohol) l Binge drinking = 3% (1 in 33 binge drinking) Among Binge drinkers: Pregnant women have higher frequency of binge drinking than non-pregnant women Prevalence of alcohol use in pregnant women is higher for women with college degrees compared to less education
FASD Epidemiology ¡ It is not known what percentage of babies will be born with FASD if the mother drinks alcohol during pregnancy. ¡ FASD is likely underdiagnosed l l l ¡ ¡ Dysmorphic features can be less noticeable in newborns CNS deficits may not be recognized until preschool age Less consideration for prenatal alcohol use to be underlying factor in behavioral and learning disorders The CDC: up to 1. 5 infants per 1000 births with FAS The CDC: 0. 3 out of 1000 children from 7 to 9 years of age with FAS May et al. (2009): 10. 9 to 25. 2 cases of FAS/p. FAS per 1000. May et al. (2014): 24 to 48 of FASD per 1000.
FAS Surveillance in US ¡ 2009: CDC – Surveillance for FAS in 3 states (AZ, CO, NY) among 7 -9 year olds l l FAS rates ranged from 0. 3 to 0. 8 FAS cases per 1000 children ages 7 -9 years Highest among Native Americans: 2 FAS cases per 1000 children ages 7 -9 years Lowest among Hispanic: 0. 2 cases per 1000 children ages 7 -9 years No differences in prevalence by age or sex
FASD Surveillance in US May et al (2014) – Surveillance for FASD in Midwestern town among first graders l Active Case Ascertainment –Tier I, III l Interview Mothers, then examiners review all cases for final diagnosis l Estimated Prevalence ¡ FAS: 6 -9 per 1000 children ¡ PFAS: 11 -17 per 1000 children ¡ Total FASD: 24 -48 per 1000 children
FASD Can Happen to Any Child
Primary Care Setting: Screening for FASD ¡ Maternal Factors Report of maternal drinking during pregnancy ¡ Other risk factors ¡ ¡ Child Factors Sibling with FAS ¡ Unusual physical appearance/anomalies ¡ Behavioral/developmental problems ¡ ¡ Awareness of Populations with higher prevalence ¡ Child Welfare Services
Diagnostic Evaluation Process for FASD With a positive screening: refer for diagnostic evaluation l l Multidisciplinary approach (includes morphological, behavioral, and neuropsychological assessment) Diagnosis of Exclusion
Reminder: Fetal Alcohol Spectrum Disorders Institute of Medicine* – 4 categories ¡ l FAS – Fetal Alcohol Syndrome l PFAS –Partial Fetal Alcohol Syndrome l ARBD – Alcohol-Related Birth Defects l ARND – Alcohol-Related Neuro-developmental Disorder *Hoyme, et al. , (2016). Updated clinical guidelines for diagnosing fetal alcohol spectrum disorder. Pediatrics: 138, 1 -18.
Diagnostic Criteria for Fetal Alcohol Syndrome (FAS) With or without documented prenatal alcohol exposure The diagnosis of FAS requires A – D: A. B. C. D. Characteristic pattern of minor facial anomalies Prenatal and/or postnatal growth deficiency Evidence of CNS involvement Neurobehavioral Impairment **For children > 3: cognitive and/or behavioral impairment **For children < 3 years of age: Evidence of developmental delay
Confirmation of Maternal Alcohol Consumption ¡ One or more of the following conditions: l l l > 6 drinks/week for > 2 occasions during pregnancy > 3 drinks per occasion on > 2 occasions during pregnancy Documentation of alcohol-related social or legal problems in proximity to the pregnancy Documentation of intoxication during pregnancy by blood, breath, or urine content testing Positive testing with established alcohol-exposure biomarker(s) during pregnancy or at birth Increased prenatal risk associated with drinking during pregnancy as assessed by validated screening tool
Characteristic Pattern of Minor Facial Anomalies Including > 2 of the following: ¡ ¡ ¡ Short palpebral fissures (less than or equal to the 10 th percentile) Thin vermilion border of the upper lip (score 4 or 5 on the lip/philtrum guide) Smooth philtrum (score 4 or 5 on the lip/philtrum guide)
Palpebral Fissure Measurement
Normative Data for Palpebral Fissure Measurements
Lip-Philtrum Guide
Microcephaly
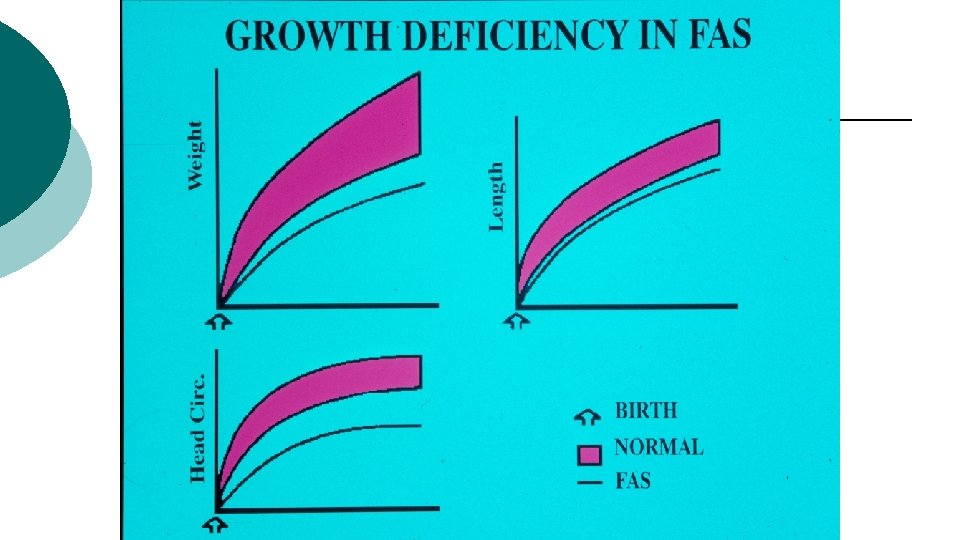
Prenatal and/or Postnatal Growth Deficiency Restricted prenatal and/or postnatal growth including: l l Height – less than 10 th percentile on normal growth curves* Weight – less than 10 th percentile on normal growth curves *Plot on racially or ethnically appropriate growth curve if available
Evidence of CNS Involvement Including > 1 of following: ¡ Decreased head circumference at birth (< 10 th percentile) ¡ Structural brain abnormalities ¡ Recurrent, non-febrile seizures
Evidence of Neurobehavioral Impairment > 3 years of age ¡ With Cognitive Impairment: Evidence of global impairment (> 1. 5 SD below mean) OR cognitive deficit (> 1. 5 SD) in at least one domain ¡ With Behavioral Impairment: Evidence of behavioral deficit in at least 1 domain > 1. 5 SD below mean in selfregulation < 3 years of age ¡ Evidence of developmental delay > 1. 5 SD below the mean
FAS – Only the Tip of the Iceberg ¡ ¡ ¡ PFAS –Partial Fetal Alcohol Syndrome (PFAS) Alcohol-Related Birth Defects (ARBD) Alcohol-Related Neurodevelopmental Disorders (ARND)
Diagnostic Criteria for PFAS: With Confirmed Maternal Alcohol Consumption A. Characteristic pattern of > 2 minor facial anomalies B. Neurobehavioral impairment (either cognitive or behavioral): l l > 3 years of age: global impairment or cognitive deficit in 1 domain or behavioral deficit in at least 1 domain < 3 years of age: developmental delay
Diagnostic Criteria for PFAS: Without Confirmed Maternal Alcohol Consumption A. Characteristic pattern of > 2 minor facial anomalies B. Growth deficiency or deficient brain growth, abnormal morphogenesis, or abnormal neurophysiology C. Neurobehavioral Impairment: l l > 3 years of age: global impairment or cognitive deficit in 1 domain or behavioral deficit in at least 1 domain < 3 years of age: developmental delay
Diagnostic Criteria for ARBD A. Documented prenatal alcohol exposure B. One or more specific major malformations demonstrated in animal models and human studies to be the results of prenatal alcohol exposure
Associated congenital anomalies, malformations, & dysplasias: Cardiac ASD Aberrant great vessels VSD Conotruncal heart defects Hypoplastic nails Clinodactyly of 5 th fingers Short 5 th digits Pectus carinatum/excavatum Radioulnar synostosis Vertebral segmentation defects Lg joint contractures Scoliosis Camptodactyly “Hockey stick” palmar creases Renal Aplastic/hypoplastic/ Dysplastic kidneys “Horseshoe” kidneys/ Ureteral duplications Eyes Strabismus Refractive errors Retinal vascular anomalies Optic nerve hypoplasia “Railroad track” ears Conductive/ neurosensory hearing loss Skeletal Ears
Hockey Stick Palmar Crease
Railroad Track Ears
Diagnostic Criteria for ARND Diagnosis cannot be made in children <3 years old A. Confirmed maternal alcohol consumption B. Neurobehavioral impairment: • • With cognitive impairment: evidence of global impairment, cognitive deficits in at least 2 domains With behavioral impairment: behavioral deficits in at least 2 domains
BREAK TIME
Evidence of Neurobehavioral Impairment > 3 years of age ¡ With Cognitive Impairment: Evidence of global impairment (> 1. 5 SD below mean) OR cognitive deficit (> 1. 5 SD) in at least one domain ¡ With Behavioral Impairment: Evidence of behavioral deficit in at least 1 domain > 1. 5 SD below mean in selfregulation < 3 years of age ¡ Evidence of developmental delay > 1. 5 SD below the mean
Neuropsychological Assessment ¡ ¡ ¡ Clinical Interview - Parent or caregiver v Background History v Cognitive & Behavioral Concerns v Adaptive Behavior Concerns Record Review – Medical & Academic Standardized Testing l Cognitive l Behavioral l Adaptive Skills
Neurobehavioral Impairments in FASD ¡ ¡ ¡ ¡ Language Deficits Learning and Memory Attention Executive Functions Self-Regulation Adaptive Functioning Sensory Processing
Neuropsychological Assessment ¡ Standardized Testing l l l l Intellectual Ability Attention/Information Processing Executive Functions Language Visual Perception/Visual Construction Learning and Memory Motor Function Academic Functioning
Intellectual Ability ¡ ¡ Diminished intellectual functioning, with group means falling in the borderline to extremely low range (IQs 65 -75) Low intellectual functioning remains relatively unchanged over lifespan
Attention & Information Processing Speed ¡ ¡ Attention deficits common including: vigilance, focused attention, sustained attention (visual>auditory), and shifting attention Impaired processing speed including: slower processing speed on effortful tasks
Executive Functions ¡ ¡ Impairment in executive control including: planning, shifting, fluency, and concept formation Difficulties with processes underlying executive functioning: working memory, response inhibition
Language l Expressive Language: includes verbal and nonverbal skills and how an individual uses language l Receptive Language: comprehension of language l Pragmatic Language: social language skills
Visual Perception & Visual Construction ¡ Less known about these skills ¡ Generally intact facial recognition ¡ Impaired skills include: visual-motor integration, spatial learning/working memory, spatial recall, visual-perceptual matching
Learning and Memory ¡ ¡ ¡ Children with FASD are known to have difficulty with learning new information “What is learned one day is gone the next day” Animals exposed to alcohol show damage to the hippocampus- an area in the brain that is critical for learning new information
Motor Function § § Fine Motor Deficits include: delayed development, weak grasp, and poor eye-hand coordination Gross Motor Deficits include: balance, coordination, and ball skills
Academic Functioning ¡ ¡ ¡ Reading: weaker reading comprehension than decoding skills Mathematics: Primary learning difficulty Written Expression: writing mechanics, organization, production
Cognitive Functioning in FASD: Summary
Behavioral Assessment ¡ Standardized Sensory Processing/Integration l Behavior: Behavioral Phenotype l Adaptive Functioning Examiner Observation/Provided History Goal: differential diagnosis, identify comorbid diagnoses l ¡ ¡ Questionnaires
Sensory Integration/Processing ¡ Sensory Processing Differences include l l l ¡ Auditory Visual Tactile Pain Perception Vestibular Need for Occupational Therapy
Behavioral Phenotype ¡ ¡ ¡ Externalizing Behaviors: hyperactivity, conduct problems Internalizing Symptoms: inattention, mood disorders Need for psychotherapy/behavioral support; possible medication management
Adaptive Functioning includes assessment of ¡ Social Skills ¡ Adaptive Communication Skills ¡ Personal Living Skills ¡ Community Living Skills ¡ Adaptive Motor Skills
Neuropsychological Assessment Putting It All Together l Comprehensive Report l Feedback sessions with parents/caregivers
Diagnostic Coding ¡ Other Specified Neurodevelopmental Disorder due to prenatal alcohol exposure l l ¡ Fetal Alcohol Syndrome (dysmorphic) l ¡ DSM-5: 315. 8 ICD-10: F 88 ICD-10: Q 86. 0 Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (DSM 5)
Common Comorbid Diagnoses ~40% ADHD ¡ ~15 -20% Intellectual Disability ¡ ~25% Learning Disability ¡ ~30% Sensory Impairment ¡ ~4% Cerebral Palsy ¡ ~30% Speech & Language Disorders ¡
FASD: Differential Diagnosis ¡ Facial Features l l l ¡ ¡ Smooth Philtrum: Opitz syndrome, Cornelia de Lange syndrome, Toluene embryopathy, Floating-Harbor syndrome Thin Vermillion Border: Miller-Dieker syndrome, Cornelia de Lange syndrome, fetal valproic syndrome Short Palpebral Fissures: Williams syndrome, Trisomy 18 syndrome, PKU fetal effects, Opitz syndrome Growth Retardation CNS involvement
FASD: Differential Diagnosis
. BREAK TIME
FASD Interventions What helps maximize an individual’s potential?
Video: Mother of Adoptive Child with FASD https: //www. youtube. com/watch? v=m 7 Vf. Rg 8 u-5 w
General Guidelines: Strengthening Families, a project of the Center for the Study of Social Policy: www. strengtheningfamilies. net Protective Factors Framework: 1. Parent Resilience 2. Knowledge of Parenting and Child Development 3. Social and Emotional Competence of Children 4. Social Connections 5. Concrete Support in Times of Need
General Caregiver Guidelines Provide a safe, stable, and structured home l Avoid too much sensory stimulation l Use calming approaches/techniques l Use simple, specific directions (1 step) l Keep rules simple and consistent l Have immediate consequences/feedback on behavior l
General Guidelines for Interventions with FASD Children Minimize change ¡ Offer services over a longer period of time ¡ Expect slower progress ¡ Use examples, modalities and treatment goals that are appropriate for children with FASD ¡ Consider child’s cognitive abilities, behavior regulation problems; other comorbid conditions ¡
General Guidelines: Behavioral Problems Recognizing your child's strengths and limitations ¡ Implementing daily routines ¡ Creating and enforcing simple rules and limits ¡ Keeping things simple by using concrete, specific language ¡ Using repetition to reinforce learning ¡ Pointing out and using rewards to reinforce acceptable behavior ¡ Teaching skills for daily living and social interactions ¡
FASD Presenting Concerns Infant & Toddlers ¡ Sleep disturbances ¡ Feeding difficulties ¡ Reduced attention ¡ Decreased visual focus ¡ Hyper-arousal ¡ Problems with coordination and balance ¡ Frequently irritable
Interventions to Support Infant & Toddlers ¡ Early identification and referral for EI ¡ Support for caregivers is essential Early intervention and a stable, nurturing home are important factors in protecting children with fetal alcohol syndrome from some of the secondary disabilities they're at risk of later in life
FASD Presenting Concerns 4 – 5 Year Olds ¡ Delayed speech development ¡ Altered motor skills ¡ Attention deficits ¡ Learning deficits ¡ Behavioral concerns
Example: Strategies for Enhancing Early Developmental Success (SEEDS) ¡ Enhances child’s capacity to regulate emotions and behaviors and impacts multiple levels of the family system Parent education and advocacy module l Attachment-based parenting skills group l Music-based parent-child play group l
Example: Manitoba Canada Community-Based Home-Visiting Program with Preschool Children Prenatally Exposed to Alcohol ¡ ¡ Community home-based attachment intervention, Circle of Security® (COS), with preschool children affected by PAE/FASD
Video: 9 year-old boy with FASD https: //www. youtube. com/watch? v=bd 3 ts. HOz. Tr 0
FASD Presenting Concerns for School-Aged Children ¡ Neurocognitive ¡ Self-Regulation ¡ Adaptive/Social
Interventions to Support School-Age Children ¡ ¡ Home-Based: treatment for mother; individual therapy; parent/caregiver support; medication; adaptive skills training Education-Based: special education; speech/language, occupational, & physical therapies; FASD-specific strategies; social skills intervention; assistive technology
The Families Moving Forward Program takes a positive parenting approach that uses weekly therapeutic intervention to help you care for a child with known or suspected FASD.
Example: Alert Program ¡ Self-Regulation Program ¡ Program Aims l l l Teach children concept of self-regulation Teach sensory self-awareness Teach child to select behaviors that match the environment
Example: Visual Cues to Support Behavior Regulation
Example: Project Bruin Buddies ¡ Parent-Assisted Training ¡ Project l l l Child Friendship Aims Develop understanding of social cues Develop social problem solving Develop conflict avoidance/negotiation
Video: Adult with FASD https: //www. youtube. com/watch? v=Laf. Um. ARk. Ppg
FASD Presenting Concerns for Adolescents Behavioral Problems ¡ Problems with planning, organization, & timemanagement ¡ Problems with focusing ¡ Problems with temper, mood, & impulsive behaviors ¡ Poor judgment ¡ Acts like younger child
FASD Presenting Concerns for Adolescents Learning Problems l Reading comprehension l Math achievement l Language problems l Faulty logic l Problems with abstract thinking
General Guidelines for Working with Adolescents & Young Adults Safety & Health Considerations l Higher accidents and injuries l More experiences of abuse and mistreatment by adults and peers l Problems following medication routines l Problems making decisions about legal and illegal substances l Difficulties driving safely l Risk for suicide
General Guidelines for Working with Adolescents & Young Adults 14 -60 % have Legal Problems l Poor impulse & temper control l Problems understanding future consequences l Trouble understanding what is illegal l Difficulty connecting cause and effect l Difficulty taking responsibility l Vulnerability to peer pressure & high suggestibility/ victimization l Weaknesses in learning from experience
General Guidelines for Working with Adolescents & Young Adults The 4 S’s + C ¡ Structure ¡ Supervision ¡ Simplicity ¡ Steps ¡ Context
Interventions for Adolescents & Young Adults ¡ ¡ ¡ Recognize potential for co-occurring disorders, secondary disabilities, risk for health, safety, and legal problems Holistic approach - consider all aspects of life Safe, structured environments – home/community Include family and caregivers Include client in building a treatment plan Consider needs for transition to adulthood: Family planning, vocational training, guardianship to support financial & medical decisions
Interventions for Adolescents & Young Adults ¡ ¡ ¡ Individual treatment may be more effective than group treatment Establish routines & written guidelines: Need to teach social rules, boundaries Awareness of sensory issues interfering with success – too bright, too loud Use multiple methods for processing and learning new skills • Watching videos, role-play specific scenarios • Expressing self in creative ways, music & art Use active listening and build success
Presenting Concerns for Adults Behavior & Learning Problems Perseverates, Rigid Thinking/Behavior l Difficulty holding a job/living independently l Poor social skills/lack of reciprocal relationships l Drug/alcohol abuse l
FASD Secondary Disabilities Disrupted school experience/school failure ¡ Mental health problems ¡ Inappropriate sexual behavior ¡ Trouble with the law/incarceration ¡ Alcohol & drug problems ¡ Unemployment ¡ Dependent living ¡
General Guidelines: Low Intellectual Ability ¡ ¡ ¡ Speak slowly and use simple and clear language at all times. Stop between ideas and allow for processing. Use concrete terms like “walk slowly” rather than “straighten up” Avoid using the negative terms like “stop running” instead say “thank you for walking slowly” Use visual cues to help with the explanations
General Guidelines Continued: Low Intellectual Ability ¡ Break each task into small steps and teach through repetition ¡ Reinforce behaviors you want and use the same language each time ¡ Understand the child will have difficulty benefitting from feedback ¡ “Think younger”: Understanding (especially social/emotional) will be below chronological age
Examples: FASD-Specific Strategies ¡ ¡ ¡ Multi-modal presentation Experiential teaching methods Routines/Schedules Memory aids Repeat, repeat
General Guidelines: Comorbid Behavioral & Psychiatric Disorders Psychiatry referral for medication Stimulants ¡ Antidepressants/Anti-Anxiety ¡ Neuroleptics ¡
FASD Positive Characteristics/Strengths Creativity (artistic, musical) ¡ Perseverance (determined, committed) ¡ Friendly/trusting, affectionate ¡ Spontaneous, lots of energy ¡ Great sense of humor ¡
FASD Long-Term Support ¡ Section 1115 of the Social Security Act ¡ State-specific waiver plans: www. medicaid. gov ¡ Vocational Rehabilitation Programs ¡ College/University Programs
Neuroimaging Methods: Structural & Functional ¡ ¡ Neuroimaging methods allow visualizing brain structures in detail (MRI, DTI) Some other imaging methods allow looking at what is happening in the brain (function) while someone doing a task (f. MRI, EEG, MEG)
Structural MRI: Cortical Overall Brain Size Cerebral Cortex Frontal Lobes Parietal Lobes Temporal Lobes
Brain Differences: FASD versus Control
Structural MRI: Subcortical ¡ Basal Ganglia l Caudate Nucleus ¡ Corpus Callosum ¡ Hippocampus ¡ Cerebellum
Basal Ganglia: Caudate Nucleus ¡ ¡ ¡ Basal Ganglia: motor control and learning Caudate Nucleus: associated with learning, mental flexibility, and behavioral inhibition Basal ganglia structures are significantly smaller even when controlling for overall brain size
Caudate Nucleus in Two 18 -Year Olds Normal FAS
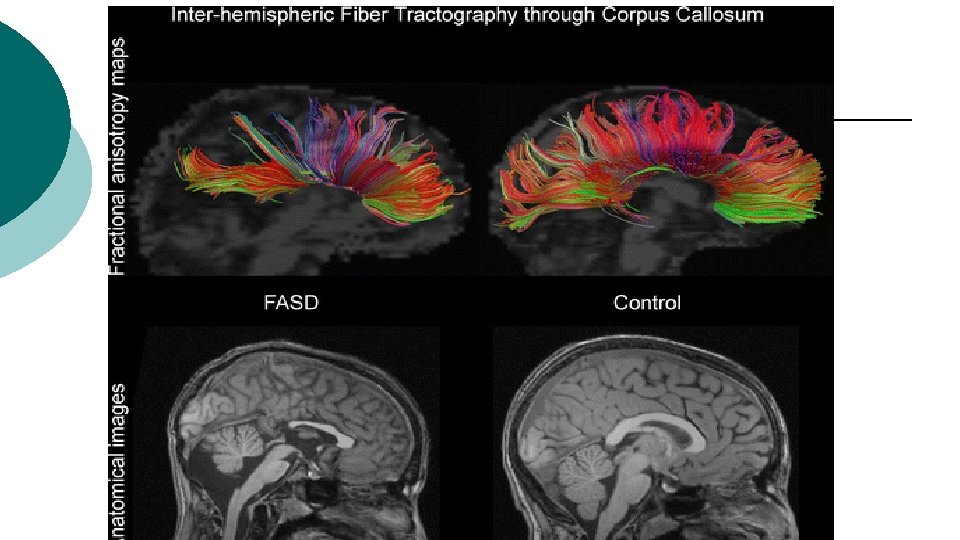
Corpus Callosum ¡ ¡ ¡ The corpus callosum is the fiber tract that connects the two hemispheres Anomalies in the corpus callosum can range from thinning in some regions to the total absence called agenesis The integrity of corpus callosum is critical to the integration of information from two hemispheres
Hippocampus ¡ ¡ The hippocampus is a structure located inside the medial temporal lobe The hippocampus plays a critical role in learning and memory
Hippocampus: FASD versus Control
Cerebellum ¡ ¡ Important for attention, executive functions, and movement Differences seen in cerebellar structures for individuals with FASD
Cerebellum: Control versus FASD
Functional Brain Imaging ¡ Magnetoencephalography (MEG) ¡ Functional Magnetic Resonance Imaging (f. MRI)
Magnetoencephalography
Delayed neural responses to stimuli as revealed by magnetoencephalography; Stephen et al. (in press)
Functional Magnetic Resonance Imaging (f. MRI) ¡ Spatial Working Memory ¡ Inhibitory Control ¡ Verbal Learning & Working Memory ¡ Visual Working Memory ¡ Summary f. MRI Findings
Summary At a behavioral level children with FASD show slow information processing and increased inattentiveness. ¡ At a neurocognitive level children with FASD display impaired performance on tasks that involve the integration and manipulation of information. ¡ At a neuronal level children with FASD show both structural and functional differences. ¡
Research Challenges & Opportunities Mechanisms of Alcohol’s Prenatal Effects ¡ Preventing Potentially Harmful Alcohol Consumption ¡ Combination Drug Use and FASD ¡ Biomarkers of FASD ¡ Animal Models ¡
FASD Resources ¡ ¡ ¡ State-specific waiver plans l www. medicaid. gov Substance Abuse and Mental Health Services Administration (SAMHSA) l https: //store. samhsa. gov/shin/content/SMA 134803/SMA 13 -4803. pdf National Institute on Alcohol Abuse and Alcoholism ¡ http: //pubs. niaaa. nih. gov/publications/arh 341/toc 34_1. htm
FASD Resources No. FAS: National Organization on Fetal Alcohol Syndrome - (800) 66 -NOFAS; www. nofas. org ¡ American Academy of Pediatrics – FASD Toolkit: www. aap. org/en-us/advocacy-and-policy/aap-healthinitiatives/fetal-alcohol-spectrum-disorderstoolkit/Pages/default. aspx ¡ CDC: www. cdc. gov/ncbddd/fasd/index. html ¡ IHS: www. ihs. gov/telebehavioral/icpfaqs/ ¡ The Arc: www. thearc. org/what-we-do/resources/factsheets/fetal-alcohol-spectrum-disorder ¡
QUESTIONS