The female pelvis and fetal skull 2018 2019

















is at the")






this is largest")








- Slides: 38
The female pelvis and fetal skull 2018 -2019 4 th year ﺍﻟﻤﻌﻴﻨﻲ ﺍﺳﺮﺍﺀ . ﺩ. § ﺍ
The bony pelvis is made of four bones : The sacrum , coccyx , and two innominates(ilium, ischium and pubis). These bones are held together by symphsis pubis , sacroiliac joints and sacrococcygeal joint. The sacrum consists of 5 fused vertebrae, the anterior –superior edge of the first vertebra is called sacral promontory, which protrudes slightly into the cavity of the pelvis. the anterior surface of the sacrum is usually concave. it articulates with the illium at its upper segment , with coccyx at its lower segment , and with the sacrospinous and sacrotuberous ligaments laterally. The coccyx is composed of three to five rudimentary vertebrae. it articulate with the sacrum.
The pelvic brim and inlet The pelvic brim is the inlet of the pelvis and bounded in front by the symphysis pubis (the joint separating the two pubic bones) on each side by the upper margin of the pubic bone the ileopectineal line and the ala of the sacrum posteriorly by the promontory of the sacrum.
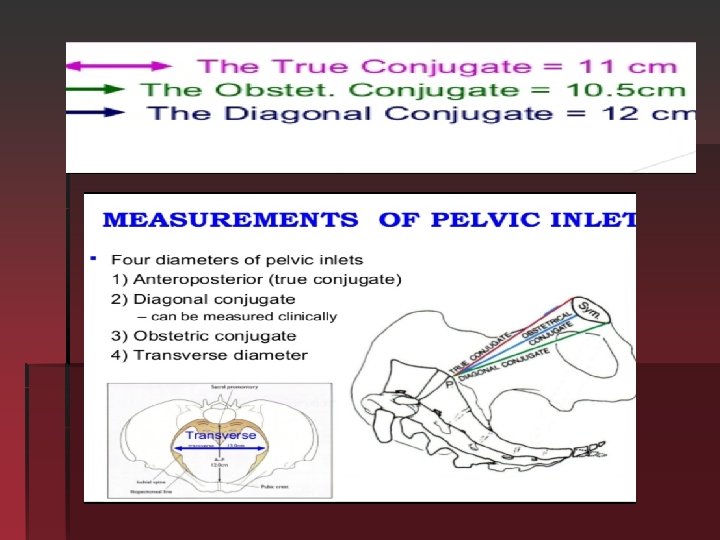
The pelvic brim and inlet: the normal transverse diameter in this plane is 13. 5 cm and is wider than the anterior-posterior diameter which is normally 11 cm , angle of the inlet is normally 60 degree to the horizontal in the erect position.
The cavity is almost rounded , as the transverse and anterior diameter are similar at 12 cm , the ischial spine are palpable vaginally and are used as land mark to asses the descent of the head during vaginal examination (station) they are also used as land marks for providing an anesthesia block to the pudendal nerve. Pudendal nerve passes behind and below the ischial spine on each
Station: of the presenting part in the pelvis canal is define as its level above or below the plane of the ischial spines. Ischial spine level =zero station eacn 1 cm above or below the level of ischial spine, given -1 and +1
The pelvic midcavity can be described as an area bounded in front by the middle of the symhysis pubis on each side by the pubic bone the obturator fascia and the inner aspect of the ischial bone and spine poteriorly by the junction of the 2 nd and 3 rd section of the sacrum.
The pelvic out let The pelvic outlet is bounded in front by the lower margin of the symphysis pubis on each side by the descending ramus of the pubic bone, the ischial tuberosity and the sacrotuberous ligment posteriorly by the last piece of sacrum
The pelvic out let The AP diameter of the pelvic out let is 13. 5 cm and the trasverse diameter is 11 cm.
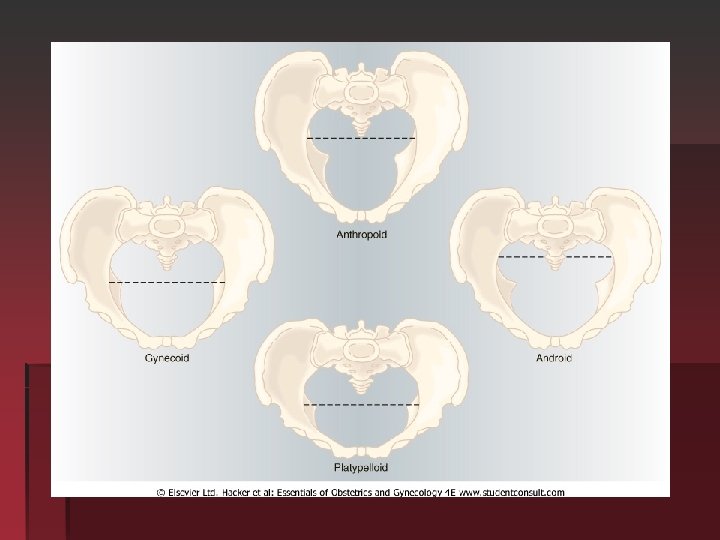
Avariety of pelvic shapes has been described and these may contributed to difficulties in labor
Gynaecoid pelvis Present in 40%of women pelvic inlet is rounded with transverse diameter larger than anteroposterior diameter side wall is straight , well rounded sacroscaitic notch, well curved sacrum , spacious sub pubic angle =90 degree, average prominence of spine , head forced to occipital anterior position
Anthropoid pelvis 20% of female , long narrow oval inlet , long antero-posterior diameter large posterior inclination of sacrum , spine not prominent but close , narrow subpubic angle , precipitate occipitalposterior position and delivery in such
Android pelvis In 30% of women tringular inlet with flat post segment widest diameter closed to sacrum , side is convergent , long and narrow sacrosciatic notch, shallow sacral curve , narrow subpubic arch , prominent spine , forced to be occipittrasverse position (funnel shape) deep trasverse arrest
Platypelloid pelvis Flattened gynaecoid pelvis 3%of female pelvis oval shape inlet , straight or divergent side wall, round sacrosciatic notch , posterior inclination of sacrum , wide bispinous diameter , wide subpubic angle , fetal head engage in transverse diameter increased risk of obstructed labour.
The pelvic floor This is formed by the two levator ani muscles which with their fascia form a musculofascial gutter during the 2 nd stage of labour. The perineal body is a codensation of fibrous and muscular tissue lying between the vagina and the anus. It receives attachments of the posterior ends of the bulbocavernous muscles , the medial ends of the superficial and deep transverse perineal muscles and the anterior fibers of the external anal sphincter , it is always involved in a 2 nd degree perineal tear and an episiotomy.
episiotomy type 1. median or midline 2. mediolateral 17
The FETAL skull The fetal skull is made up of the vault , face , base. The vault of the skull is formed by the parietal bones and parts of the occipital , frontal and temporal bones. Between these bones there are four membaranous sutures, the sagital , frontal coronal and lumbdoidal sutures
§ The anterior fontanelle or bregma closed at 18 months (diamond shape)is at the junction of the sagittal , frontal and coronal sutures § The posterior fontanelle triangular in shape lies at the junction of the sagittal and lambdoidal sutures between the two parietal bones and the occipital bone closed at 6 -8 weeks of life. § It allow these bone to move together and even to overlap the parietal bones usually tend to slide over the frontal and occipital bones. § The bones themselves are compressible together these characteristics of the fetal skull allow a process called moulding to occur , which effectively reduces the diameter of the fetal skull and encourages progress through the bony pelvis with out harming the under lying brain.
Vertex the area of the fetal skull bounded by the two parietal eminences and the anterior and posterior fontanelle. Attitude of the fetal head refers to the degree of flexion and extension at the upper cervical spine. Different longitudinal diameters are presented to the pelvis in labor depending on the attitude of the fetal head.
The diameter of fetal skull
The diameter of fetal skull: § Vertex presentation § Well flexed head the longitudinal diameter , is the suboccipito – bregmatic diameter 9. 5 cm and measured from the sub occipital to the anterior fontanelle . § § longitudinal diameter that present in a less well flexed head such as is found in the occipito- posterior position is the Suboccipito-frontal diameter and is measured from the suboccipital region to the prominence of the forehead 10 cm.
§ Further extension of the head Occipito-frontal daimeter present this is measured from the root of the nose to the posterior fontanelle and is 11. 5 cm.
The largest longitudinal § daimeter that may present is the Mentvertical which is taken from the chin to the furthest point of the vertex and measure 13 cm known as Brow presentation and it is usually too large to pass through the normal pelvis.
§ Extension of the fetal head beyond this point result in a smaller daimeter, submentobreg matic daimeter is measured below the chin to the anterior fontanelle and is 9. 5 cm this is clinically a face presentation.
§ Transverse diameters of fetal skull are: § Biparietal (9. 5 cm)this is largest transverse, diameter (between two parietal bones). § Bitemporal 8 cm shortest transverse diameter , between two temporal bones.
Engagment occurs when the widest diameter of the fetal presenting part has passed through the . pelvic inlet. In vertex –biparietal , breech-intertrochanteric
Synclitic: when the biparietal diameter is parallel to the pelvic plane and the sagital suture is mid way between the anterior and posterior planes of the pelvis when this relationship not present the head is considered to be asynclitic
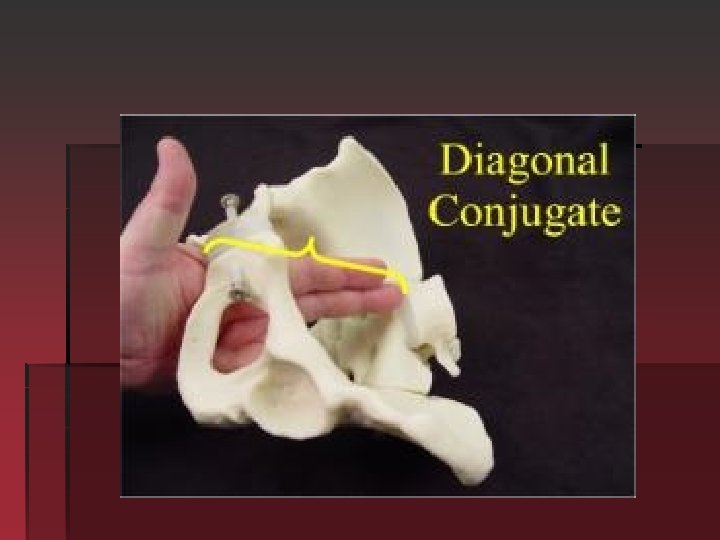
Clinical pelvimetry: The clinical evaluation of the pelvis Pelvic inlet: 1 -Anteroposterior diameter assesment by measure the diagonal. conjugate , which is obtained on clinical examination 11. 5 considered is considered adequate. The obstetric conjugate is then estimated by subtracting 1. 5 to 2 cm Often the middle figure of the examining hand cannot reach the sacral promontory, thus the obstetric conjugate is adequate. 2 -The anterior surface of the sacrum is then palpated to assess its curvature. The usual shape is concave. Aflat or convex shape may indicate anteroposterior constriction throughout the pelvis. §
Diagonal conjugate
The midpelvis 1 -the pelvis side walls can be assessed to determine whether they § are convergent rather than having the normal , almost parallel, configuration. 2 -The ischial spines are palpated carefully to assess their prominance and several passes are made between the spines to approximate the bispinous diameter more than 10. 5 cm.
3 -The lenghth of the sacrospinous ligment is assessed by placing one fingure on the ischial spine and on the sacrum in the midline. The average length is 3 fingure breadths. 4 -If the sacrospinous notch that is located lateral to the ligament can accommodate two-and half fingure tips, the posterior mid pelvis is most likely of adequate dimensions. short ligament suggests a forward inclination of the sacrum and a narrwed sacrospinous notch.
pelvic outlet is assessed. 1 - This is done by first placing a fist between the ischial tuberosities. An 8. 5 cm distance is considered an adequate transverse diameter. The posterior sagittal measurement should also be greater than 8 cm. 2 - The infrapubic angle is assessed by placing thumb next to each inferior pubic ramus and then estimating the angle at which they meet. An angle of less than 90 degree is associated with a contracted transverse diameter in the midplane and out let.
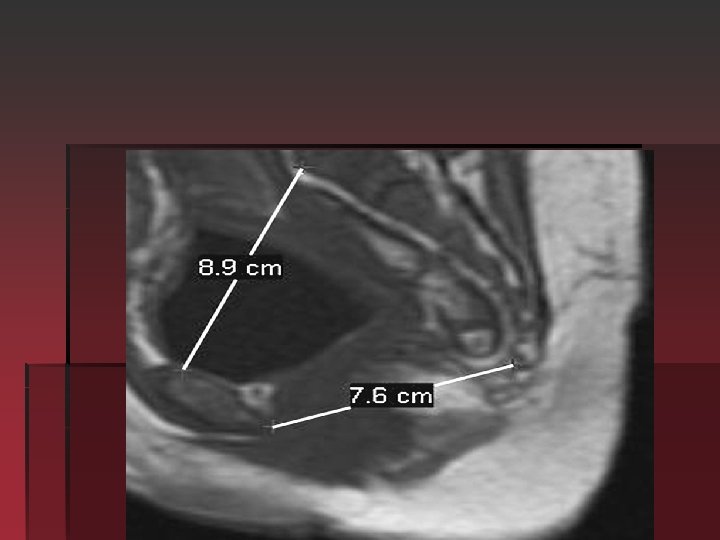
Radiological assessment of the pelvis: § When an accurate measurement of the pelvis is indicated nuclear magnetic resonance may be used. The advantage of MRI over the X-Ray or CT for the pelvic assessment is the lack of ionizing radiation exposure. Indications: 1 -Clinical evidence or obstetric history suggestive of pelvic abnormalities. 2 -Ahistory of pelvic trauma.