Bipolar Disorder in Children and Adolescents Robert A

Bipolar Disorder in Children and Adolescents Robert A. Kowatch, MD, Ph. D Professor of Psychiatry The Ohio State University’s Wexner Medical Center Nationwide Children’s Hospital Center for Innovation in Pediatric Practice

DSM-IV Bipolar Disorders • Bipolar I Disorder • “Manic Depressive Illness” • Bipolar II Disorder • Cyclothymia • Bipolar Not Otherwise Specified • BP “NOS”

Lifetime Prevalence of Bipolar Disorder in the USA • Adults (NCS Replication Study, Merikangas et al. 2007) • Bipolar I Disorder: 1. 0% • Bipolar II Disorder: 1. 1% • Bipolar Subthreshold: 2. 4% • Adolescents • Bipolar Disorder: 1. 0 -1. 4% • Children • ? ? ?

Goodwin and Jamison, Manic Depressive Illness, March 22, 2007 | ISBN-10: 0195135792 | ISBN-13: 9780195135794 | Edition: 2

Topics • Differential diagnosis of mood swings in children and adolescents • Pharmacothera py of pediatric bipolar disorder Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Differential Diagnosis Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Other disorders that frequently cause mood swings • • ADHD ODD Anxiety Disorders Fetal Alcohol Spectrum Disorder • (ARND)
 Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html")
Attention-Deficit/Hyperactivity Disorder (ADHD) Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Attention Deficit Hyperactivity Disorder DSMIV Criteria • A persistent pattern of inattention and/or hyperactivityimpulsivity that is more frequent and severe than is typically observed in individuals at a comparable level of development • Some impairment from the symptoms must be present in at least 2 settings (e. g. , at home and at school) • There must be clear evidence of interference with developmentally appropriate social, academic, or occupational functioning • Present before age 7 years • 6 symptoms for at least 6 months

Prepubertal & Early Adolescent Bipolarity Differentiate From ADHD by Manic Symptoms § Subjects 60 Bipolar Subjects with ADHD § Mean age of 11 + 2. 7 yr. 60 ADHD Subjects with no mood disorder § Mean age of 9. 6 + 2 yr. § Method CGAS < 60 WASH-U-KSADS, 16 Mania Items § Mothers § Children & Adolescents Geller & Williams 1998
 Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html")
Oppositional Defiant Disorder (ODD) Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

DSMIV Criteria for Oppositional Defiant Disorder • A. A pattern of negativistic, hostile, and defiant behavior lasting at least 6 months, during which four (or more) of the following are present: • • • Often loses temper Often argues with adults Often actively defies or refuses to comply with adults' requests or rules • Often deliberately annoys people • Often blames others for his or her mistakes or misbehavior • Is often touchy or easily annoyed by others • Is often angry and resentful • Is often spiteful or vindictive B. The disturbance in behavior causes clinically significant impairment C. The behaviors do not occur exclusively during the course of a Psychotic or Mood Disorder D. Criteria are not met for Conduct Disorder

ODD vs. BPD Symptoms ODD BPD Often loses temper + + Often argues with adults + +/- Often actively defies or refuses to comply with adults' requests or rules + +/- Often deliberately annoys people + +

ODD vs. BPD Symptoms ODD BPD Often loses temper + + Often argues with adults + +/- Often actively defies or refuses to comply with adults' requests or rules + +/- Often deliberately annoys people + + Euphoria/Irritability - Inflated Self Esteem/grandiosity - Decreased Need for Sleep - More Talkative/Pressured Speech - + + Flight of Ideas/Racing Thoughts - Distractibility - Increased Goal Activity/Agitation - Excessive Involvement in Pleasurable Activities - + +

Anxiety Disorders Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Lifetime prevalence of mental disorders in U. S. adolescents 35 32 30 Lifetime Prevalence 25 With Severe Impairment 20 % 20 15 14 11 10 8 10 11 5 2. 7 0 Mood Anxiety Behavior Substance Use Eating Dis Merikangas et al. , J Am Acad Child Adolesc Psychiatry. 2010 Oct
 Worry a lot Headaches/Stomach Aches Anxiety often")
Anxiety Disorders § Generalized Anxiety Disorder (GAD) Worry a lot Headaches/Stomach Aches Anxiety often causes mood swings § OCD Symptoms > 1 Hour/Day Obsessions Compulsions § “Just Right” Phenomena § Frequent mood swings if things don’t go just right

Fetal Alcohol Disorders Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html
 § Maternal alcohol use during pregnancy § Growth deficiencies stunted")
Fetal Alcohol Syndrome (FAS) § Maternal alcohol use during pregnancy § Growth deficiencies stunted prenatal and/or postnatal growth § Permanent brain damage resulting in neurological abnormalities, delay in development, intellectual impairment and learning/behavior disabilities § Abnormal facial features including short eye opening, short nose, flat midface, thin upper lip and small chin

Fetal Alcohol Syndrome Facies Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html
 Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html")
Fetal Alcohol Syndrome (FAS) Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html
 • • • Full Dysmorphia Absent Poor impulse control Problems")
Alcohol-Related Neurodevelopmental Disorder (ARND) • • • Full Dysmorphia Absent Poor impulse control Problems in social perception Deficits in higher level receptive and expressive language Problems in memory, attention, or judgment learning Difficulties, deficits in school performance Poor capacity for abstraction or metacognition Specific deficits in mathematical skills Mood Dysregulation
 Slides Courtesy of David Axelson, M. D. Associate Professor")
Disruptive Mood Dysregulation Disorder (DMDD) Slides Courtesy of David Axelson, M. D. Associate Professor of Psychiatry Western Psychiatric Institute & Clinic - UPMC

DSM-5 Proposal: Disruptive Mood Dysregulation Disorder • • • A. The disorder is characterized by severe recurrent temper outbursts in response to common stressors. B. The temper outbursts are manifest verbally and/or behaviorally, such as in the form of verbal rages, or physical aggression towards people or property. C. The reaction is grossly out of proportion in intensity or duration to the situation or provocation. • The responses are inconsistent with developmental level. Frequency • The temper outbursts occur, on average, three or more times per week. Mood between temper outbursts: • Nearly every day, the mood between temper outbursts is persistently negative (irritable, angry, and/or sad). • The negative mood is observable by others (e. g. , parents, teachers, peers).
 • TDD is similar to SMD except the")
DMDD vs. Severe Mood Dysregulation (SMD) • TDD is similar to SMD except the symptoms of hyperarousal have been removed • SMD Hyperarousal Symptoms (need at least 3) • Insomnia • Agitation • Distractibility • Racing thoughts • Flight of ideas • Pressured speech • Intrusiveness

Temper Dysregulation Disorder with Dysphoria Criteria • Duration: Criteria A-C have been present for at least 12 months. Throughout that time, the person has never been without the symptoms of Criteria A-C for more than 3 months at a time. • The temper outbursts and/or negative mood are present in at least two settings (at home, at school, or with peers) and must be severe in at least in one setting. • Chronological age is at least 6 years (or equivalent developmental level). • The onset is before age 10 years.
 • In the past year, there has")
Temper Dysregulation Disorder with Dysphoria (cont. ) • In the past year, there has never been a distinct period lasting more than one day during which abnormally elevated or expansive mood was present most of the day for most days, and the abnormally elevated or expansive mood was accompanied by the onset, or worsening, of three of the “B” criteria of mania (i. e. , grandiosity or inflated self esteem, decreased need for sleep, pressured speech, flight of ideas, distractibility, increase in goal directed activity, or excessive involvement in activities with a high potential for painful consequences; see pp. XX). Abnormally elevated mood should be differentiated from developmentally appropriate mood elevation, such as occurs in the context of a highly positive event or its anticipation.

Disruptive Mood Dysregulation Disorder • The behaviors do not occur exclusively during the course of a Psychotic or Mood Disorder (e. g. , Major Depressive Disorder, Dysthymic Disorder, Bipolar Disorder) and are not better accounted for by another mental disorder (e. g. , Pervasive Developmental Disorder, post-traumatic stress disorder, separation anxiety disorder). (Note: This diagnosis can co-exist with Oppositional Defiant Disorder, ADHD, Conduct Disorder, and Substance Use Disorders. ) • The symptoms are not due to the direct physiological effects of a drug of abuse, or to a general medical or neurological condition.

DSM-V rationale for DMDD • Marked upsurge in the diagnosis of bipolar disorder in youth • Coincided with debate as to whether mania in children presented with severe, non-episodic irritability • Presented support from post-hoc analyses of longitudinal epidemiological studies that chronic irritability does not progress to bipolar disorder in young adulthood • Evidence from Severe Mood Dysregulation (SMD) studies in regard to differences between SMD vs. Narrow Phenotype BP youth in short-term course, family history and neural circuitry
 • Noted scientific support is limited but clinical need was strong")
DMDD Rationale (con’t) • Noted scientific support is limited but clinical need was strong for a separate diagnosis (instead of a course specifier for ODD) • “Based purely on scientific evidence, inclusion of a specifier might be most easily justified. However, when both clinical need and scientific evidence are considered together, a different conclusion emerges. ” Issues Pertinent to a Developmental Approach to Bipolar Disorder in DSM-5. accessed from www. dsm 5. org. American Psychiatric Association, 2010

Problems with TDD • “…it is clear that, from a pathophysiological perspective, TDD is unlikely to be categorically distinct from ODD, which is itself a heterogeneous category with disparate longitudinal outcomes. ” 1 • “It can certainly be argued that it is premature to suggest the addition of the TDD diagnosis to DSM-V, since the work has been done predominately by one research group in a select research setting” 2 1 Issues Pertinent to a Developmental Approach to Bipolar Disorder in DSM-5. accessed from www. dsm 5. org. American Psychiatric Association, 2010 2 DSM-5 Childhood and Adolescent Disorders Work Group. Justification for Temper Dysregulation Disorder with Dysphoria. accessed from www. dsm 5. org. American Psychiatric Association, 2010

Problems with DMDD • Abnormal mood, but no accompanying symptoms (temper outbursts are a behavioral manifestation of irritable mood) • Research support from studies of SMD, not TDD • Likely to be a very heterogeneous population • Almost all (85%) have ODD and ADHD • Difficult to determine “not exclusively during mood disorder” & “not better accounted for by ASD, PTSD…” in clinical settings • May be overly broadly applied • May stimulate drug companies to get FDA indication for TDD

Mood Swings Quick Guide

Higher Level of Suspicion § Family history of mood disorders § Episodes of aggressive behavior in the context of other manic symptoms § § § Early age of onset for depression Mood disorder with psychotic features Recurrent depressive episodes resistive to treatment Episodic presentation of ADHD Mood destabilization secondary to stimulant or antidepressant
… Fair Use Doctrine, http: //www. copyright. gov/fls/fl")
When you hear hoof beats (mood swings)… Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html
…")
When you hear hoof beats (mood swings)…

Pharmacotherapy of Children and Adolescents with Bipolar Disorder Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html
, placebocontrolled, double-blinded trials are there for mania in children and")
How many, large (n>100), placebocontrolled, double-blinded trials are there for mania in children and adolescents? 1. 2 2. 4 3. 9 4. 12
 116 PBC: Lithium vs")
Large Controlled Trials in Pediatric Mania Trial n Oxcarbazepine (Trileptal) 116 PBC: Lithium vs DVP 153 Sodium Divalproex (Depakote ER) 150 Risperidone (Risperdal) 169 Olanzapine (Zyprexa) 161 Quetiapine (Seroquel) 284 Aripiprazole (Abilify) 296 Ziprasidone (Geodon) 238 TEAM (Risp, Lith, DVP) 279 Total 1846

Status of Pediatric Bipolar Studies and Indications Double-Blind, Placebo-Controlled Studies Divalproex Lithium Oxcarbazepine Topiramate Carbamazepine ER Risperidone Olanzapine Aripiprazole Quetiapine Ziprasidone Open-Label Studies Lithium Carbamazepine Divalproex Topiramate Risperidone Olanzapine Aripiprazole Quetiapine Ziprasidone Comparator Studies Quetiapine vs. divalproex Lithium vs. Valproate vs PBO Green=Indicated White=Not Indicated
 Carbamazepine § New/Novel Gabapentin Lamotrigine Topiramate")
Mood Stabilizers § Traditional Lithium Valproate (Sodium Divalproex) Carbamazepine § New/Novel Gabapentin Lamotrigine Topiramate Tiagabine Oxcarbazepine Levetiracetam Zonisamide

Pediatric Lithium Trials • 4 Older, Crossover Trials • • Average n = 18 Response Rates 33 -80% • 1 Double-Blind Placebo Trial • Geller et al. , 1997 • 1 Discontinuation Trial • Lithium Salts Kafantaris 2004
 § NIMH Funded, Multi-Site § § CCHMC, Case Western,")
Pediatric Bipolar Collaborative Trial (PBC) § NIMH Funded, Multi-Site § § CCHMC, Case Western, Milwaukee Children’s Double blinded, doubledummy, placebo controlled Randomized Monotherapy § Lithobid, Depakote, Placebo § 2: 2: 1 § 6 Months of Treatment 8 Week Acute 16 Week Continuation § Stimulants for ADHD could be added § 153 Subjects Randomized Ages 7 -17 yr.
 § NIMH Funded, Multi-Site § § CCHMC, Case Western,")
Pediatric Bipolar Collaborative Trial (PBC) § NIMH Funded, Multi-Site § § CCHMC, Case Western, Milwaukee Children’s Double blinded, doubledummy, placebo controlled Randomized Monotherapy § Lithobid, Depakote, Placebo § 2: 2: 1 § 6 Months of Treatment 8 Week Acute 16 Week Continuation § Stimulants for ADHD could be added § 153 Subjects Randomized Ages 7 -17 yr. 0. 6 Cohen's D 0. 4 0. 2 0 0. 41 Lith vs PBO 0. 54 DVP vs PBO

Lithium • FDA Indication • Indicated in the treatment of manic episodes of manicdepressive illness > age 12 years Side effects Common Weight gain, Exacerbation of Acne, Enuresis, Hypothyroidism Uncommon Polyuria/Polydipsia, Hair loss, NMS (Haloperidol) Interactions NSAID Increase lithium levels Antibiotics (ampicillin, doxycyline, tertacycline…) decrease renal clearance of lithium and increase level of lithium

Lithium Use § Target dose of 30 mg/kg/day Start outpatients 25 mg/kg/day Serum level of 0. 9 -1. 1 m. Eq/L § Onset of action: 7 -14 days Full efficacy in 6 -8 Weeks § Baseline labs: CBC/diif, pregnancy, EKG, renal & thyroid function, calcium § Q 6 Months Lithium Level, TSH, BUN, serum creatinine

Management of Common Lithium Side Effects

Divalproex Sodium Use in Children § Target dose of 20 mg/kg/day Start outpatients at 15 mg/kg/day Serum level of 80 -120 mg/m. L § Onset of action: 7 -14 days Full efficacy in 4 -6 weeks § Side effects Nausea Sedation Weight gain § Labs: pregnancy, CBC, platelets, LFTs § Monitor for Polycystic Ovary Syndrome (PCOS)

Divalproex/Valproate Side Effects Nausea, vomiting, diarrhea Tremor/Myoclonus Sedation, mental dulling Weight gain Hair loss, decreased platelets Liver toxicity, pancreatitis, hyperinsulinism, polycystic ovary syndrome (PCOS) Black Box Warning Hepatotoxicity: Hepatic failure resulting in fatalities has occurred in patients receiving valproic acid and its derivatives. Experience has indicated that children under the age of two years are at a considerably increased risk of developing fatal hepatotoxicity, especially those on multiple anticonvulsants… Pancreatitis: Cases of life-threatening pancreatitis have been reported in both children and adults receiving valproate.
 Acute manic and mixed episodes • Target serum level")
Carbamazepine • Clinical Indications (Adults) Acute manic and mixed episodes • Target serum level • • 9 -11 g/ml Many Cytochrome P 450 Interactions Strong association between the risk of developing SJS/TEN with carbamazepine treatment and the presence of an inherited variant of the HLA-B gene, HLA-B*1502 Testing for HLA-B*1502 should be performed in patients with ancestry in patients of Chinese ancestry Side effects Dizziness, somnolence, nausea, vomiting, ataxia Black Box Warning “Aplastic anemia and agranulocytosis have been reported in association with the use of carbamazepine. ”

Mood Stabilizer Toolbox Mood Stabilizer Start at Target Serum Level Lithium 25 -30 mg/kg/day 0. 8 -1. 2 Meq/L Renal/Thyroid Function Valproate 15 -20 mg/kg/day 85 -110 μg/m. L Liver/Pancreas/ PCOS Plats. Hyperammonemia 7 -10 μg/m. L WBC/Plats. Carbamazepine 15 -20 mg/kg/day Monitor Watch Out For Dehydration toxicity CYP 450 Interactions
 § Gabapentin § Topiramate § Oxcarbazepine § Lamotrigine § Levetiracetam")
Newer Antiepileptic Drug (AEDs) § Gabapentin § Topiramate § Oxcarbazepine § Lamotrigine § Levetiracetam § Tiagabine § Zonisamide Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

A Pilot, Controlled Trial of Topiramate for Mania in Children and Adolescents With Bipolar Disorder § DB, Placebo-controlled § 56 subjects Mean age 13. 8 ± 2. 6 yrs 48% female 62% mixed episode 59% comorbid ADHD § Dose Mean 278 +121 mg/day Del. Bello MP, et al. J Am Acad Child Adolesc Psychiatry. 2005; 44 Mean Change From Baseline F 1, 48 = 2. 12, P=0. 152

A Double-Blind, Randomized, Placebo-Controlled Trial of Oxcarbazepine in the Treatment of Bipolar Disorder in Children and Adolescents 116 Outpatients Ages 7 -17 yr. Bipolar I, Mixed or Manic Double-Blinded, Placebo Controlled Flexibly Dosed 900 -2400 mg/day Mean dose 1515 mg/day Primary Efficacy Measure YMRS Wagner et al. , Amer J Psychiatry July 2006

Lamotrigine § Blocks voltage-sensitive sodium channels § Adults 2 controlled studies demonstrated efficacy for bipolar depression § Indicated for maintenance treatment of BP I in adults § Concern: serious rashes/serum sickness FDA black box warning § Not FDA-indicated < Age 16 yrs

Lamotrigine - Rashes & Dosing § Higher past incidence of rash due to Higher initial dosing and faster titration 1 Concomitant VPA administration 1, 2 Definition of serious rash including any rash leading to discontinuation from trial 2 § Regular tabs available in 25 mg, 100 mg, 150 mg, 200 mg § Chewable tabs in 2 mg, 5 mg, 25 mg § Stanford Antigen Precautions by T. Ketter 1 Dooley, J, et al (1996) Neurology 46: 240 -242 2 Messenheimer, J (2002) J Child Neurology 17: 2 S 34 -42

Revised Lamotrigine Dosing Initiating lamotrigine in adult bipolar patients: Not taking drugs known to increase the clearance of lamotrigine* or valproate Weeks 1 & 2 25 mg/day Weeks 3 & 4 50 mg/day Week 5 Week 6 100 mg/day Target dose 200 mg/day Taking valproate Weeks 1 & 2 25 mg/every other day Weeks 3 & 4 25 mg/day Week 5 Week 6 50 mg/day Target dose 100 mg/day Taking drugs known to increase the clearance of lamotrigine* and not taking valproate Weeks 1 & 2 50 mg/day Weeks 3 & 4 100 mg/day in divided doses Week 5 200 mg/day in divided doses Week 6 300 mg/day in divided doses Week 7 Target dose up to 400 mg/day in divided doses

An Open-Label Study of Lamotrigine Adjunct or Monotherapy for the Treatment of Adolescents with Bipolar Depression § 20 subjects enrolled BPI, II, NOS Mean Age 15 yr. § 8 -week open study § Weekly assessments: CDRSR, YMRS, CGI-S, OAS-M, CGIC § Mean final dose = 132 ± 31 mg/day § Response CGI-C: 16/19 (84%) CDRS-R: 12/19 (63%) Chang et al. JAACAP March 2006 CDRS-R YMRS
 2. Asenapine Maleate (Saphris) 3. Clozapine (Clozaril) 4. Iloperidone")
Atypical Antipsychotics 1. Aripiprazole (Abilify) 2. Asenapine Maleate (Saphris) 3. Clozapine (Clozaril) 4. Iloperidone (Fanapt) 5. Lurasidone (Latuda) 6. Olanzapine (Zyprexa) 7. Olanzapine/Fluoxetine (Symbyax) 8. Paliperidone (Invega) 9. Quetiapine (Seroquel) 10. Risperidone (Risperdal) 11. Ziprasidone (Geodon) Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

A Double-Blind Randomized Pilot Study Comparing Quetiapine and Divalproex for Adolescent Mania § 50 Adolescent inpatients Bipolar disorder, type I, mixed or manic § Mean Age 15+1 yr. § Treatment duration 28 days § Randomized/Double. Dummy/DB Quetiapine 400 -600 mg/day § 100 -200 -300 -400 Valproate 80 -120 mg/dl (20 mg/kg) § 96% achieved level > 80 mg/dl by day 7 Del. Bello et al. JAACAP March 2006 YMRS Remission Rates DVP QUE

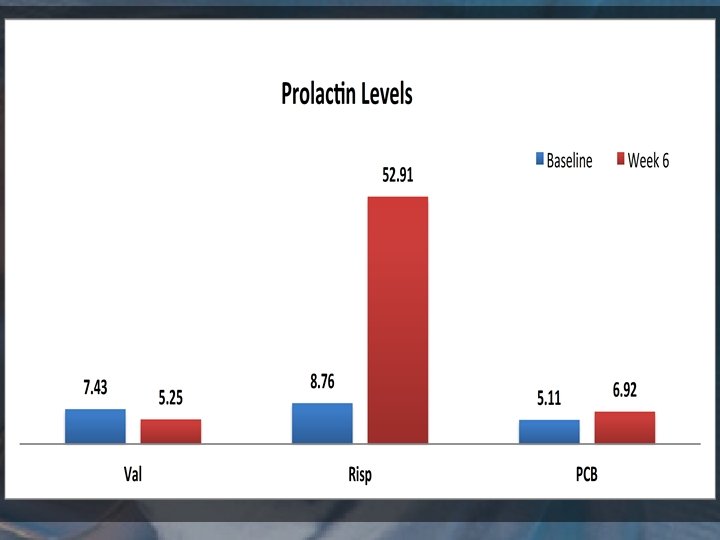
Risperidone for the Treatment of acute mania in bipolar youth • J & J Sponsored Multisite • BD I, mixed or manic • N=166 • 10 -17 years old • Inpatients or Outpatients • 3 -week DBRCT • 2 doses of RIS • 0. 5 -2. 5 mg/day • 3. 0 -6. 0 mg/day

Adverse Events: Risperidone in Pediatric Mania Placebo 0. 5 -2. 5 mg/day 3. 0 -6. 0 mg/day Response rate 26% 59% 63% YMRS change, mean (SD) 9 (11) 19 (10) 17 (10) 8% 5% 25% Boys 0. 6 (7) Girls 2 (7) Boys 32 (23) Girls 50 (46) Boys 50 (23) Girls 68 (49) 0% 11% 25% 0. 7 (1. 9) 1. 9 (1. 7) 1. 4 (2. 4) EPS Prolactin change, mean (SD) Abnormal prolactin Weight change, mean kg (SD)

Olanzapine in the Treatment of Acute Manic or Mixed Episodes in Adolescents Efficacy § 3 Week, Double-blind, placebo 2: 1 Randomization § 161 Subjects BP I, Mixed or Manic Mean Age 15+1. 1 yr. § Age Range 13 -17 Psychotic 18% Baseline YMRS 32 § Modal Dose 9. 7+4. 5 mg/day Tohen et al. AJP 2007 Olanz Placebo

Olanzapine in the Treatment of Acute Manic or Mixed Episodes in Adolescents Efficacy § 3 Week, Double-blind, placebo 2: 1 Randomization § 161 Subjects BP I, Mixed or Manic Mean Age 15+1. 1 yr. § Age Range 13 -17 Psychotic 18% Baseline YMRS 32 § Modal Dose 9. 7+4. 5 mg/day Tohen et al. AJP 2007 Weight ≥ 7% of baseline*** Olanz Placebo Weight Gain Olanz. N/N (%) Placebo n/N (%) **p Value 44/105 (41. 9) 1/54 (1. 9) <. 001

Olanzapine 26 Week Open. Label Extension Treatment • 146 adolescents with bipolar I, manic or mixed who completed a 3 week double-blind placebo controlled study • Open label olanzapine (2. 5 mg– 20 mg/day) for up to 26 weeks • Results: • Response rate 62. 9% • ≥ 50% decrease YMRS and CGI-BP severity ≤ 3 Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Summary of Atypical Controlled Trials in Pediatric Bipolar Disorder Study/ Sponsor Ref N Olanz. / Lilly Tohen Am J Psych. 161 Risper. / Janssan AACAP 2007 Aripip/ BMS Duration (Days) Dose (mg/day) Response Rate (YMRS) Mean Weight Gain (kg) DBPCRT 2: 1 21 10. 4 +4. 5 49% 3. 66 +2. 18 BPD I Manic, Mixed DBPCRT 1: 1: 1 21 0. 5 -2. 5 3 -6 59% 63% 1. 9 1. 4 10 -17 BPD I Manic, Mixed DBPCRT 1: 1: 1 28 10 30 45% 64% 0. 9 0. 54 M 10 -17 BPD I Manic DBPCRT 1: 1: 1 21 400 64% 58% 1. 7 M 10 -17 BPD I Manic, Mixed DBPCRT 2: 1 28 80 -160 -13. 83 (Zipras) -8. 61 (PBO) - Sites Age Range Yr. DX 26 10 -17 BPD I Manic, Mixed 169 M 10 -17 ACNP 2007 296 M Que/ Astra. Zeneca ACNP 2007 284 Zipras/ Pfizer APA 2008 238 Design

YMRS Change Scores Atypical Antipsychotics vs. Mood Stabilizers 20 18 16 YMRS Score 14 16. 5 8 15. 6 14. 25 14. 2 12 10 18. 5 17. 65 9. 99 8. 2 16. 5 13. 83 11 9. 04 9. 1 8. 61 9 High 6 6 Low PBO 6 4 2 0 Arip Olanz Quet Risp Zipras Lith Val
 Target Dose (mg/day) Monitor Aripiprazole 2. 5")
Atypical Toolbox Atypical Antipsychotic Start at (mg/day) Target Dose (mg/day) Monitor Aripiprazole 2. 5 -5 5 -20 Weight/Height/BMI EPS Olanzapine 5 5 -20 Weight/Height/BMI Weight (Choles/FAs) Quetiapine 50 -100 300 -600 Weight/Height/BMI Weight Risperidone 0. 35 -0. 50 1 -3 Weight/Height/BMI EPS/TD/Weight Ziprasidone 20 -40 80 -160 Weight/Height/BMI ECG Take with food Assess cardiac risk factors Watch Out For

A Randomized Controlled Trial of Risperidone, Lithium, or Divalproex Sodium for Initial Treatment of Bipolar I Disorder, Manic or Mixed Phase, in Children and Adolescents • • 279 antimanic medication– naive subjects age, 10. 1 years; 50. 2% female) 100% elated mood and/or grandiosity, 77. 1% psychosis, 97. 5% mixed mania, 99. 3% daily rapid cycling, mean (SD) mania duration of 4. 9 (2. 5) years. Dosing • Mean (SD) titrated lithium level was 1. 09 (0. 34) m. Eq/L, • Mean (SD) divalproex sodium level was 113. 6 (23. 0) μg/m. L. • Mean (SD) titrated risperidone dose was 2. 57 (1. 21) mg. Comparisons of end-point Clinical Global Impressions for Bipolar Illness Improvement. Mania (CGI-BP-IM) response rates by medication Geller, B. et al. Arch Gen Psychiatry 2012; 0: Archgenpsychiatry. 2011. 1508 v 1 -14

Treatment Algorithm for Mania/ Hypomania in Children and Adolescents 1 A: Mixed/Manic Quetiapine/ Aripiprazole/Risperidone Stage 1 Monotherapy 1 B: Lithium/Valproate/ Olanzapine/Ziprasidone Negative response Evaluate Positive response Continue Partial response Stage 2 Augmentation 2: Add mood stabilizer to atypical or vice versa Evaluate Stage 3 2 drug combinations Partial response or nonresponse 3: 2 mood stabilizers + 1 atypical or 2 atypicals + mood stabilizer Kowatch RA et al. Clinical Manual for the Management of Bipolar Disorder in Children and Adolescents. Arlington, VA: American Psychiatric Publishing, Inc; 2008.

Pediatric BPD Comorbid Disorders Disorder Prepubertal Adolescent 70 -90% 30 -60% 20 -30% 30 -40% 30 -60% Oppositional Defiant Disorder 60 -90% 20 -30% Substance Abuse 10% 40 -50% 30 -40% ADHD Anxiety Disorders Conduct Disorders Learning Disabilities

Young Children Mania Trial • Sponsored by the Stanley Research Foundation • 6 week, double-blinded, placebo, controlled • Randomized to: • Liquid valproate, risperidone or placebo • 46 Subjects • Ages 3 -7 yr. ; mean age 5. 5 yr • ~70% Caucasian • ~60% Male • DSM-IV Criteria for Bipolar Disorder I, Mixed or Manic Episode, Current

Family History in Mother or Father 70 60 60 50 40 % 28 30 23 20 9 10 0 BPD MDD ADHD Schizophren

Young Mania Rating Scale p=0. 008 B 6 1 2 3 Week 4 5

Guidelines: How Long to Treat? • The Consensus of Opinion Was That Medication Tapering or Discontinuation Be Considered If the Patient Has Achieved Remission for a Minimum of 12 -24 Consecutive Months • For Less Severely Ill Patients, or in Patients for Whom a Diagnosis Is Less Clear, a Briefer Treatment Period May Be Indicated CABF Guidelines 2006

• 115 Children • Enrolled 1995 -1998 • First Episode Bipolar I • Ages 7 -16 yr. • Elation and/or Grandiosity • Retention Rate 94% • Assessed • 6, 12, 18 months • 2, 3, 4, 5, 6, 8 yr. • Treated in community

• After Reaching Age 18 yr. • 115 Children • Enrolled 1995 -1998 • 54 Subjects • First Episode Bipolar I • Mean Age 20. 6+1. 8 yr • Ages 7 -16 yr. • Outcome • Elation and/or Grandiosity • 44% BPD I • Retention Rate 94% • 30% Depressive • Assessed Disorder • 6, 12, 18 months • 35% SUD • 2, 3, 4, 5, 6, 8 yr. • Treated in community

Pediatric Bipolar Summary Difficult to recognize and manage More Research Is Needed Single Agents Combination Pharmacotherapy + DBT Recurrent Disorder That Requires Psychosocial Therapy & Pharmacotherapy We are making progress Fair Use Doctrine, http: //www. copyright. gov/fls/fl 102. html

Course of Illness & Psychosocial Treatment of Bipolar Disorder in Children Mary A. Fristad, Ph. D, ABPP Professor, Psychiatry, Psychology & Nutrition Director, Research & Psychological Services Division of Child & Adolescent Psychiatry The Ohio State University’s Wexner Medical Center

Just Because I’m Bipolar th 14 Year Old 8 Grader Former MF-PEP Study Participant Just because I’m bipolar I’m not a freak I’m not weird I just want to be noticed Just because I’m bipolar I still have feelings I still have emotions I just have trouble expressing them Just because I’m bipolar I can still be trusted I can still be reliable Just because I’m bipolar—I’m still a normal kid

Conflict of Interest/Funding § Dr. Fristad receives royalties from § CFPSI: MF-PEP and IF-PEP Workbooks § Guilford Press: § Raising a Moody Child: How to Cope with Depression and Bipolar Disorder § Psychotherapy for Children with Bipolar and Depressive Disorders § APPI: § Clinical Manual for Management of Bipolar Disorder in Children and Adolescents § Children’s Interview for Psychiatric Syndromes (Ch. IPS)

When Will My Child Get Better. . . ? The MDD Picture Birmaher et al, 96 § Single episode length: 7 -9 months § 90% get well by 1. 5 -2 years § 6 -10% stay impaired § Recurrence § 40%, 2 yrs § 70% 5 yrs

When Will My Child Get Better? The DD Picture Kovacs et al, 94 § Single untreated episode: 4 years § MDD episode usually comes 2 -3 years after DD onset § Can lead to: § Bipolar disorder: 13% § Substance abuse: 15%
")
Early Age of Onset Linked to Longest Delay to Treatment Leverich et al (2007) J Ped 150: 485 -490 480 outpts w/ BPD retrospectively rated for onset and prospectively followed for one year

Adults—BPD Rea et al, JCCP, 2003 § UCLA study, N=53: delays rehospitalization

Does Expressed Emotion Predict Mood Symptom Scores Over 2 Years Among Adolescent Bipolar Patients (N=20)? (Miklowitz et al. , 2006; Dev and Psychopathology) High-EE Low-EE Time (Months) F(1, 17) = 6. 33, p =. 02; Cohen’s d = 0. 98

Psychosocial Impact on Course of Illness Geller et al, 2000; 2002; 2004 § At baseline, families of youth with BPD, compared to healthy and ADHD control groups: § Less warmth § Greater tension and hostility § At 2 and 4 year follow-up, § Lower maternal warmth predicted faster relapse after recovery from mania § Intact families associated with faster rate of recovery § Medication status was not predictive of illness course

Empirically Supported Psychosocial Adjunctive Treatments for Childhood Bipolar Disorder § Fristad, Goldberg-Arnold & Gavazzi, 1999 Bipolar Disorders -None

Current Psychotherapies for Youth with Bipolar Disorder § CBT/Family Systems Based § Pavuluri/West—RAINBOW program § Miklowitz-FFT-A § PEP (MF-PEP, IF-PEP) § DBT—T. Goldstein § IP-SRT--Hlastala

How to Conceptualize Family-Based Intervention § Historically, families § Have been blamed § Have not gotten useful information/support/skill building § This can result in families being “skittish” or “defensive” about family-based intervention

Goals of Psychoeducation § Teach parents and children about § The child’s illness & its treatment § Provide support § Peers (“I’m not the only one”) § Professionals - understand the disorder § Build skills § problem-solving § communication § symptom management

Our Motto § It’s not your fault, but it’s your challenge!

ODMH Study Fristad, Goldberg-Arnold & Gavazzi, JMFT, 2003 § 35 children and their parents § 54% depressive; 46% bipolar disorders § M=3. 6 comorbid diagnoses/child (range, 1 -7) § C-GAS=51 at baseline § 29/35 (83%) on meds § 8 -11 years old (average, 10. 1 yrs) § 77% boys § 6 month wait-list design § 6 sessions, 75 minutes/session, manualdriven treatment

ODMH Findings Fristad, Goldberg-Arnold & Gavazzi, JMFT, 2003 § Parents § § § Increased knowledge of mood disorders Increased positive family interactions Increased efficacy in seeking treatment Improved coping skills Increased social support Improved attitude toward child/treatment § Children § Increased social support from parents § Increased social support from peers (trend)
 Fristad, Verducci, Walters & Young (2009) Arch Gen Psych, 66(9):")
Multi-Family Psychoeducational Psychotherapy (MF-PEP) Fristad, Verducci, Walters & Young (2009) Arch Gen Psych, 66(9): 1013 -1021 § Children aged 8 -11 (any mood disorder) § 8 sessions, 90 minutes each § Begin/end with parents/children together § Middle (largest) portion-separate groups §Children receive in vivo social skills training (in gym) after formal “lesson” is completed § Therapists: 1 -parents; 2 -children § Families receive projects to do between sessions

8 Session Outline - Parents 1. 2. 3. 4. 5. 6. 7. 8. Welcome, symptoms & disorders Medications “Systems”: school/treatment team Negative family cycle, WRAP-UP 1 st ½ Problem solving Communication Symptom management WRAP-UP 2 nd ½ of program & graduate

8 Session Outline - Children 1. 2. 3. 4. 5. 6. 7. 8. Welcome, symptoms & disorders Medications “Tool kit” to manage emotions Connection between thoughts, feelings and actions (responsibility/choices) Problem solving Nonverbal communication Verbal communication Review & GRADUATE!

Demographics—Various Samples Variable Treated BPD n=89 Age BPD-ITT n=115 9. 8 % Male 72 69 % White 91 94 % Fam Hx-Mania 53 55 % Fam Hx. Depression % Fam Hx-Either 73 72 84 83 9. 7

NIMH Study Design, N=165 Groupa Time 1 Month 0 Time 2 Month 6 Time 3 Month 12 Time 4 Month 18 MF-PEP Baseline: Follow-up + TAUb Pretreatment WLC + Baseline Follow-up Pre. Follow-up treatment TAUc a. Families were enrolled in 11 sets of 15 (7 -MFPG/8 -WLC) = 165 families b. Multi-Family Psychoeducational Psychotherapy + Treatment As Usual c. Wait-List Control + Treatment As Usual
 § <10:")
Outcome Measure § MSI=Mood Severity Index § CDRS-R + MRS (equal contributions) § <10: minimal symptoms § 11 -20: mild symptoms § 21 -35: moderate symptoms § >35: severe symptoms
 MF-PEP BPD Sample § N=115, all BPD § n=55")
Mood Severity Index (Parent, Current) MF-PEP BPD Sample § N=115, all BPD § n=55 Immediate § n=60 Wait List § Linear Mixed Effects Modeling § Χ 2=6. 19, p<. 02 § Slope difference= -7. 76/12 mos § Pre-post Imm=WLC Dr. Fristad--R 01 MH 61512
 MF-PEP Treated BPD Sample § N=89 § n=54 Immediate")
Mood Severity Index (Parent, Current) MF-PEP Treated BPD Sample § N=89 § n=54 Immediate § n=35 Wait List § Linear Mixed Effects Modeling § Χ 2=5. 91, p<. 02 § Slope difference= -7. 96/12 mos § Pre-Post Imm=WLC Dr. Fristad--R 01 MH 61512

Impact of MFPG on Service Utilization & Mood Severity Mendenhall, Fristad & Early, 2009, J Cons Clin Psychol § Parental attitudes toward treatment changes with MF-PEP; impacts quality of services sought § Improved quality of services leads to better mental health outcomes § MF-PEP appears to improve quality of services utilized & child’s mood severity over time as designed to do. It helps parents become better consumers.

Anecdotal Evaluations-Parents § No matter how bad the situation is…there is hope and treatment. Don’t give up. This program was an eye opener for me. I also was encouraged and relieved to find out that I was not alone. § Listen to what they are saying. They can really help you. Learn what is going on with your child. Stay focused on what is going with your child and do not give up on your child.

Anecdotal Evaluations. Children § You get to meet new people you never knew before. They help you with your symptoms. § They’re nice and they’re helpful. And you guys support us and give us snacks. You’ve been nice to us and treated us with respect. § It really helps out if you let it.

Efficacy-to-Effectiveness Trial Mac. Pherson, Fristad, et al, ABCT, ‘ 08, ’ 09, ‘ 10, KS Conference ‘ 10 § Parent Findings: § ↑ knowledge of mood disorders § ↑ satisfaction with treatment § Child Findings: § ↑ satisfaction with treatment § Referring Therapist Findings: § ↑ satisfaction with MF-PEP § ↑ agreement with MF-PEP goals/concepts § ↑ parental knowledge and coping § smooth transition to usual care § discussion of MF-PEP content by family in therapy sessions § intention to refer future families to MF-PEP

Efficacy-to-Effectiveness Trial Mac. Pherson, Fristad, et al, ABCT, ‘ 08, ’ 09, ‘ 10, KS Conference ‘ 10 § Treating Therapist Findings: § positive experience and general satisfaction with training in and implementation of MFPEP § interested in running future MF-PEP § Preliminary results support the transportability and acceptability of the intervention
 OH Dept Mental Health, 2002 -2004 § N=20 § 16 sessions")
Individual-Family Psychoeducation (IF-PEP) OH Dept Mental Health, 2002 -2004 § N=20 § 16 sessions § Alternate child and parent with parent § Same content + Healthy Habits § diet, exercise, sleep § Comparable design to MFPG

IF-PEP Primary Outcome: MSI-Parent-Cur—Power Analyses Variable MSI-Parent-CUR T 1 -T 2 MSI-Parent-CUR T 1 -T 3 N per Condition 64 Effect Size. 45 36 . 60

IF-PEP: Parent Evaluations § Anonymous evaluations completed after treatment § Parents report (1 -5 rating, overall 1. 6) § ↑ knowledge re: symptoms, medication, accessing treatment § ↑ skills re: working with schools and treatment team, managing symptoms at home § Feeling supported/not blamed

IF-PEP: Children’s Evaluations § 1 -5 Rating Scale § Overall rating, 1. 7 § Item Range: 1. 3 (therapist) to 2. 2 (learned about medications) § ↑ knowledge re: mood symptoms, medication § ↑ ability to get along with family, friends and at school § ↑ skill re: symptom management § ↑ support/ ↓ isolated, “not the only one” § parents’ behavior toward them better

IF-PEP 24: Two Case Studies Leffler, Fristad & Klaus, 2010, J Fam Psychotherapy § Expanded from 16 to 24 sessions § 1 sibling session § 1 additional systems-of-care (school, mental health) session § 1 school professionals session (face-toface or conference call attendance) § 2 Healthy Habits sessions § 3 additional “in-the-bank” sessions

IF-PEP 24: Case Studies Leffler, Fristad & Klaus, 2010, J Fam Psychotherapy § 11 yr old girl “Jane” § Long treatment history § sertraline, 3 mos: akathesia, elevated mood, dangerous behaviors § divalproex sodium, clonidine, quetiapine, ages 9 -11: no significant improvement § fluvoxamine and clonazapam: for compulsive behavior and agitation § School and private therapeutic support

IF-PEP 24: Case Studies Leffler, Fristad & Klaus, 2010 § 10 yr old boy “John” § Extensive treatment history § 2 yrs, divalproex sodium (trial of methylphenidate) § 4 yrs, risperidone § 6 yrs, atomoxetine § 8 yrs, trials of methylphenidate, amphetamine/dextroamphetamine, clonidine, lithium, and aripiprazole § 9 yrs, trials of quetiapine and escitalopram § 10 yrs, oxcarbazepine § very significant weight gain § Extensive psychotherapy history

Jane’s Diagnoses Leffler, Fristad & Klaus, 2010 § BP-1: Most Recent Episode Mixed: current moderate to severe symptoms: dysphoric mood, irritability, psychomotor agitation, increased appetite, strong craving for sweets, weight gain, rejection sensitivity, irritability, motor hyperactivity, derailment, mood lability § ADHD-Combined § ODD § GAD § OCD

John’s Diagnoses Leffler, Fristad & Klaus, 2010 § BP-1 Most Recent Episode Hypomanic: § current mild symptoms: irritability, negative self-image, elevated mood, uninhibited people seeking, hypersexuality § ADHD-combined § ODD § Specific Phobia-dark & heights § SAD

Jane’s Treatment Response Measure Pre C-GAS: Current 36 Post 48 Change Improved C-GAS: Worst 31 41 Improved KMRS 45 28 Improved KDRS 67 55 Improved TBQ-P 3. 9 4. 2 Improved

John’s Treatment Response Measure Pre C-GAS: Current 35 Post 40 Change Improved C-GAS: Worst 15 38 Improved KMRS 48 28 Improved KDRS 43 55 Worsened TBQ-P 3. 3 4. 2 Improved
- Slides: 120