CONVEGNO REGIONALE SIE Il trapianto a condizionamento ridotto
















 by Dausset (photo)")







 (Upjohn – Horse; n=17) 26 Doney et")















 and graft versus host (GVHD)")



 46 *LD")



 (n=301) Days after HCT 50 Sandmaier et")

 (n=301) 5% Day-100 NRM 7% Day-100 NRM 26% Relapse")
 Double Autografts (n=46) 0 1 2 3")
 P=0. 03 Double Autografts (n=46) 0 1 2 3 4 5 6")
")
 URD (51%) Percent URD (51%) MRD (49%) Survival p=0. 57 PFS")


 Myeloablative (n=45) AML – CR 1 59 FHCRC, unpubl. Years")


 62 FHCRC, unpubl.")
 63 Pagel et al. , ASH 2005.")




 Reduce relapse Radiolabeled a. CD")

- Slides: 70
CONVEGNO REGIONALE SIE Il trapianto a condizionamento ridotto RIC compie 10 anni: è l’ ora dei bilanci STORIA DEL RIC Alberto Bosi Cattedra di Ematologia Università degli Studi di Firenze Senigallia 23 -24 Ottobre 2008
En parcourant la Voie Domitienne entre Nîmes et Beaucaire
THE BEGINNINGS In the 19 th century Brown-Sequard administred bone marrow by mouth in patients with acute leukemia with an understandable lack of success
THEN… • Intramuscolar injection by Scretzenmayer in 1937 • Intramedullary instillation by Rasjeck in 1939 • and FINALLY …. Intravenous infusion by Osgood in 1939
EARLY STUDIES ON ANIMALS I • During the World War II, Reckers infused bone marrow from normal dogs into dogs exposed to 350 R. • In 1954 Barnes and Loutit reported that letally irradiated mice protected with syngenic marrow survived beyond 100 days. • However, mice given allogeneic marrow survived at 30 days, but died of a “secondary disease”.
EARLY STUDIES ON ANIMALS II • In 1959, Billingham and Brent published a study on runt disease in newborn mice and described the biology of GVH reactions. • In the 1960 s studies on dogs performed by Cavins et al showed that hematopoietic stem cells for engraftment could be obtained also from peripheral blood.
STEM CELL MODEL The importance of hematopoietic stem cells in the protection of lethally irradiated animals became clear in the 1950 s. With the Till-Mc. Culloch spleen-colony assay it was realised that clonotypic precoursors could give rise to both erythroid and myeloid cells. Murine HSCT are isolated at a frequency of 0. 05%.
HUMAN HEMATOPOIETIC STEM CELL CD 34+ Thy-1 +
EARLY CLINICAL STUDIES • In 1959 Mathè reported the infusion of marrow into patients exposed to potentially lethal irradiation in a reactor accident. • At the same time successfull transplants using an identical twin donor were reported.
FRED HUTCHINSON CANCER RESEARCH CENTER SEATTLE
Seattle Team in 1965 12 Rainer Storb Don Thomas Bob Epstein Dean Buckner
ALLOGENEIC TRANSPLANTATION Allogeneic transplantation was employed in clinics only in patients with advanced and refractory hematological malignancies who were in poor general condition. In 1957 Thomas et al. Reported intravenous infusion of bone marrow in patients receiving radiation and chemotherapy 1990 In E. Donnall Thomas shared the with Dr. Joseph Murray Nobel Prize in Physiology and Medicine
Reported Human Marrow Allografts 1958 -68 14 Bortin, Transplantation 9: 571, 1970
70 60 50 # Reported Cases Human Bone Marrow Transplants from 1958 to 1968 (n=203) (Bortin, 1970) 40 30 20 ? 10 0 15 1958 1960 1962 1964 1966 1968 Bortin, Transplantation 9: 571, 1970
16 D. W. van Bekkum & M. J. de Vries, Radiation Chimeras, Logos Press, London, 1967
Histocompatibility Typing Mid-Late 1960 s Humans Dogs Dausset: MAC; v. Rood: 4 a + b o Sera from parous women + transfusion recipients Bach: MLC Seattle: groups a–h and MLC o Sera from cross-immunized littermates Tests: Leukoagglutination or lymphocytotoxicity (trypan blue exclusion) 17
HISTOCOMPABILITY 1958 Elucidation of the genetics of human leukocyte antigen (HLA) by Dausset (photo) and van Rood Application of histocompatibility testing for organ transplantation led the way to frequent application for marrow grafting for hematological disease
1960 Medawar and Burnett received the Nobel Prize for the discovery of “acquired immunological tolerance”.
Unrelated DLA-Nonidentical Marrow Grafts *Only single drug occasionally resulting in graft-host tolerance in this setting 20 Transplantation 9: 240, 1970 Transplantation 10: 165, 1970 Blood 42: 601, 1973 Transplantation 56: 800, 1993 Bone Marrow Transplantation 15: S 98, 1995 Yu et al. , Blood 91: 2581, 1998.
CYCLOSPORINE In 1972 the immunosuppresive effect of CSA was discovered by Sandoz. CSA used was approved in 1983.
22 J Clinical Invest. 50: 1272, 1971.
1968 Canine Long-Term Survivors 23
Sites of ATG Production 24
Patient with 1° Refractory AML 25 Blood 44: 57, 1974
Survival after Therapy for Acute GVHD (n=20) (Upjohn – Horse; n=17) 26 Doney et al. Am. J. Hematol 11: 1, 1981.
CY / TBI and MTX 27 Thomas, et al. NEJM 301: 597, 1979
UNRELATED DONORS In 1973 at The Memorial Sloan-Kattering Cancer Center of New York City the first unrelated bone marrow transplant was performed on a five-year-old boy with severe combined immunodeficiency syndrome. The donor was found in Denmark through the Blood Bank. Since then….
The program started on 1974 to find a donor for Anthony Nolan, born in 1971 affected by Wiskott Aldrich syndrome. Anthony died in 1979 without a transplant "It's good to be alive. “ A bone marrow transplant recipient. Antony and Shirley Nolan
BONE MARROW REGISTRIES • In the early 1980 s individual registries of HLA-typed people were established in Milwaukee, Saint Paul, Seattle and Iawo City. • In July 1986 The American National Bone Marrow Donor Registry began to operate. • Since then stem cell donor registries have been created worlwide. • From 1999 all the registries offered all the three stem sources of stem cell used in transplants: BM, PB and CB.
PERIPHERAL BLOOD 1978 John Goldman reported the first use of blood cells for autologous transplantation after high dose cytotoxic therapy in patients with CML
CORD BLOOD TRANSPLANTATION 1989 Eliane Gluckman reported the first successful transplat using cord blood
NON MYELOABLATIVE TRANSPLANTATION Rainer Storb was one of the first investigators to show that non myeloablative HSCT can be done safely and effectively in elderly and in poor performance status patients
Rational for non-myeloablative transplants High dose chemo-radiation cannot completely sterilize many malignancies even with pre-transplant intensification Burchenal JH et al, Cancer Res 1960 Thomas ED et al, NEJM 1975
Rational for non-myeloablative transplants Many cures can be attributed to immunological anti-tumor reactions brought about by lymphocytes contained in the allograft Barnes DWH, Loutit FJ. Br J Haematol 1957 Mathè G et al, Cancer Res 1965 Weiden et al, NEJM 1979; NEJM 1981
Much of the Success of Allogeneic Hematopoietic Cell Transplantation in Cancer Due to Graft vs. Tumor Effects 36 Weiden et al. , NEJM 304: 1529, 1981 NEJM 300: 1068, 1979.
Rational for non-myeloablative transplants The curative potential of the GVT effect has been directly confirmed with DLI that could produce complete remission in patients relapsed after HSCT Kolb HJ et al, Blood 1990 Kolb HJ et al, Blood 1995
Rational for non-myeloablative transplants 1. 2. High dose chemo-radiation cannot completely sterilize many malignancies even with pre-transplant intensification The transplant effect may often be attribute to immunological anti-tumor reaction of lymphocytes contained in the allograft Conceptual emphasis has shifted away from trying to eradicate malignant cells through toxic therapy towards using allogeneic effectors cells to eliminate the malignancy
Reduced toxicity Extend the eligibility for transplantation to patients older and with comorbidities
Ages at Diagnoses vs. Ages at Myeloablative HCT 40 Molina et al. , Current Opinion Org Transpl 5: 366, 2000.
Rational for non-myeloablative transplants Improvement of post-transplant immunossuppression regimen in a preclinical canine model for decreasing the risk of GVHD and reducing HVG reactions Storb R et al, Blood 1997
T lymphocytes are effectors cells that mediate hostversus-graft (HVG) and graft versus host (GVHD) Pretransplant immunosuppression to reduce HVG Post-transplant immunosuppression to suppress residual HVG and to control GVHD → create a stable tolerance with the co-existence of donor and host cells (mixed chimerism)
PRECLINICAL CANINE MODEL 200 c. Gy TBI MMF for 4 weeks Storb R Blood 1997 CSA for 5 weeks after HSCT 450 c. Gy nodal irradiation MMF for 4 weeks CSA for 5 weeks after HSCT STABLE MIXED CHIMERISM Storb R Blood 1999
Novel Allogeneic HCT Approach 44 Substitute nonmyeloablative conditioning for toxic high-dose chemoradiotherapy Use novel postgrafting immunosuppression to both prevent graft rejection and control GVHD Grafted immune cells eliminate cancer
• Creation of marrow space by cytotoxic agents is not required for stable engraftment • Pretransplant irradiation may be replaced by non-toxic and more specific T-cell immunosuppression • The post-grafting immunosuppression facilites the development of a stable state of tolerance with mixed chimerism
Marrow Grafts From DLA-Identical Canine Littermates After Single-Dose TBI (7 c. Gy/min) 46 *LD 99 = 8 Gy Blood 86: 4376, 1995 Blood 89: 3048, 1997 BBMT 9: 489, 2003.
Clinical Treatment Protocol FLU 2 Gy TBI HCT Chimerism Analyses 30 mg/m 2/d 35 40 Related 28 CSP 6. 25 mg/kg po BID MMF 15 mg/kg po BID Unrelated -4 -3 -2 -1 0 CSP 6. 25 mg/kg po BID MMF 15 mg/kg po BID / TID 47 56 84 100 180
Reduced intensity conditioning SCT OBJECTIVES: -> Reduce the early toxicity of allogeneic SCT -> Keep the Graft-versus-leukemia effect n Mainly proposed to: - older patients (> 55 y) - patients with comorbidity n Reduces the duration of neutropenia n Reduces mucosal and liver toxicity n Does not solve the problem of GVHD
Candidates for HLA-Matched Related and Unrelated Nonmyeloablative HCT Ineligible for conventional HCT because of: Age Medical contraindications – Previous high-dose HCT – Comorbidities 49
Acute GVHD – Grades Related Unrelated (n=426) (n=301) Days after HCT 50 Sandmaier et al. , ASH 2005.
Nonmyeloablative HCT for Hematologic Malignancies Chronic GVHD No No Yes Months from Onset / Landmark 51 Baron et al. , JCO 23: 2001, 2005.
Probability Mortality Related Unrelated (n=426) (n=301) 5% Day-100 NRM 7% Day-100 NRM 26% Relapse 30% Relapse 20% Non-relapse 27% Non-relapse Years after HCT 52 Sandmaier et al. , ASH 2005
% Non-Relapse Mortality Multiple Myeloma Autograft-Allograft (n=58) Double Autografts (n=46) 0 1 2 3 4 5 6 P<0. 001 % Relapse Mortality P=0. 09 7 Double Autografts (n=46) Autograft-Allograft (n=58) 0 1 2 3 4 5 6 7 Years Prospective Randomized Study 53 Bruno et al. , NEJM 356: 1110, 2007.
Autograft-Allograft (n=58) P=0. 03 Double Autografts (n=46) 0 1 2 3 4 5 6 7 8 % Event-Free Survival % Overall Survival Multiple Myeloma P=0. 07 Autograft-Allograft (n=58) Double Autografts (n=46) 0 1 2 3 4 5 6 7 8 Years Prospective Randomized Study 54 Bruno et al. , NEJM 356: 1110, 2007.
NHL – Aggressive n=40 Mantle Cell Lymphoma n=33 Unrelated=66% Related=56% Unrelated (n=13 Related (n=27) Relapse/Progression. Free Survival 0 1 2 Years after HCT 55 Norasetthada, et al. Blood 104 (Part 1): 634 a, #2307, 2004. Maris, et al. Blood 104: 3535, 2004. 3
Fludarabine-Refractory CLL (n=82) URD (51%) Percent URD (51%) MRD (49%) Survival p=0. 57 PFS MRD (35%) p=0. 28 Years after HCT 56 Sorror, et al. JCO 23: 3819, 2005 J Clin Oncol, in press.
57 Burroughs et al. , ASH 2007.
AML 122 total Years after HCT 58 Hegenbart et al. JCO 24: 444, 2006.
% Survival Nonmyeloablative (n=22) Myeloablative (n=45) AML – CR 1 59 FHCRC, unpubl. Years after Unrelated HCT
100 % Survival 80 Nonmyeloablati ve Related=18 Unrelated=21 60 40 Myeloablative Related=29 Unrelated=27 20 AML – CR 2 0 0 60 FHCRC, unpubl. 1 2 3 4 Years after HCT 5 6
MDS – RAEB / t. AML with Chemo RX Non-ablative Ablative 61 Years after HCT Scott et al. , Leukemia 20: 128, 2006
Ph+ ALL With Imatinib (n=12) 62 FHCRC, unpubl.
Advanced AML + MDS (n=33) 63 Pagel et al. , ASH 2005.
Condizionamento nel trapianto Allogenico
Allo - trapianti linfoma Condizionamento mieloablativo N° % yes no 2000 60 40 2001 42 58 2002 32, 5 67, 5 2003 27 73 2004 29 71 2005 35 65 2006 45 55 2007 38 62
Trapianti allogenici suddivisi per patologia confronto 2002 -2007 per regime di condizionamento Convenzionale Diagnosi 2002 N° Tx 2003 N° Tx 2004 N° Tx 2005 N° Tx 2006 N° Tx 2007 N° Tx LMA 150 171 238 219 241 224 LYMPHOMA 39 35 46 59 79 70 MM/PCD 39 33 26 20 26 31 Ridotto Diagnosi 2002 N° Tx 2003 N° Tx 2004 N° Tx 2005 N° Tx 2006 N° Tx 2007 N° Tx LMA 46 49 54 77 84 70 LYMPHOMA 81 92 115 110 95 114 MM/PCD 67 94 106 77 70 58 *dati non definitivi per anno 2007
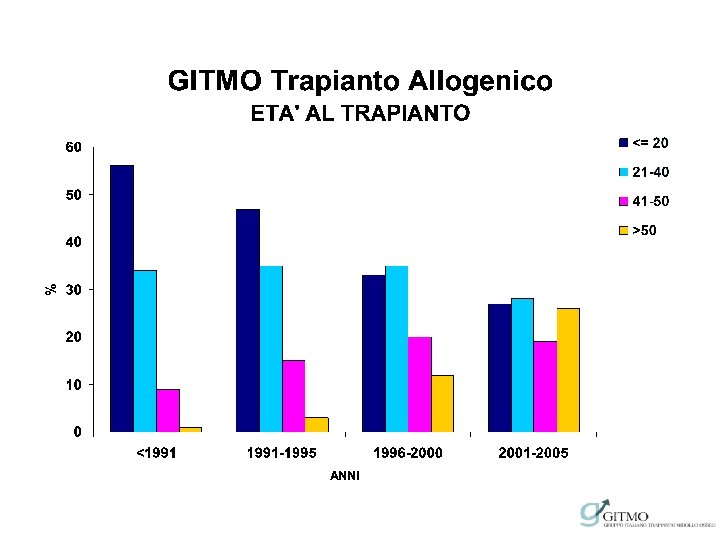
GITMO Trapianto Allogenico 2000 -2005 TRAPIANTI PER TIPO DI PATOLOGIA e CONDIZIONAMENTO
Current Directions Reduce GVHD 3 -arm randomized study (unrelated) Reduce relapse Radiolabeled a. CD 20 or a. CD 45 MAb Ablative vs. nonablative Patients with AML and MDS ≤ 65 years Increase donor pool HLA-mismatched HCT GVT effects Understanding target antigens 69
IL TEAM CLINICO 70