Childhood Hip Deformity Judson W Karlen MD Phoenix













 Unable to bear weight or mobilize")














 Septic arthritis of the hip • (+) Fever (+) Irritable joint Elevated CRP")
 Synovitis • • Diagnosis of exclusion Much more common (1: 300")
 Synovitis • Treatment Anti-inflammatories Activity restriction Typically resolves over 7 -10 days")

 • Old term: CDH (congenital) • Spectrum of")












 • Too much flexion")



























- Slides: 76
Childhood Hip Deformity Judson W. Karlen, MD Phoenix Children’s Hospital Assistant Clinical Professor University of Arizona - Phoenix School of Medicine 1
Objectives • Review etiology of childhood hip deformity • “Common” Disorders – Slipped Capital Femoral Epiphysis – Legg-Calve-Perthes – Hip Dysplasia
Objectives • Review etiology of childhood hip deformity • Common Disorders – Slipped Capital Femoral Epiphysis – Legg-Calve-Perthes – Hip Dysplasia
Slipped Capital Femoral Epiphysis • • 13 yo M 3 month history of left knee pain Limp at the end of the day Plays sports, has not missed practices. No history of injury. No night pain, fevers. Exam – limp, able to run, jump, no tenderness about the knee
Six Weeks Later – Referred to Peds Ortho
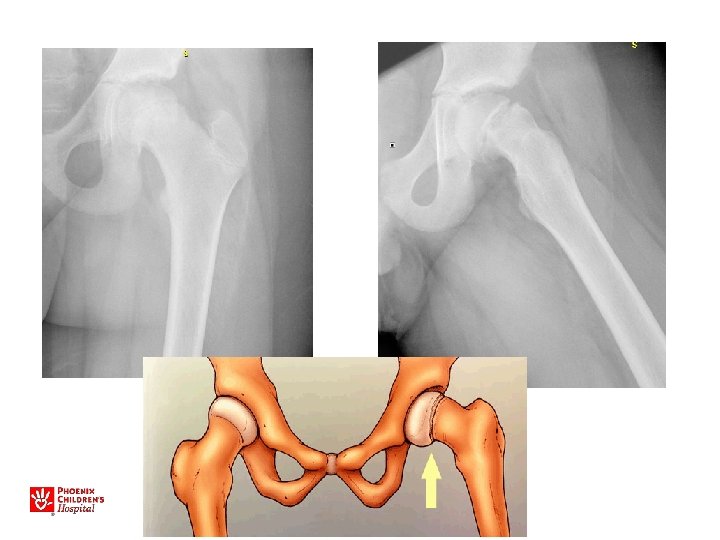
• • • Slipped Capital Femoral Epiphysis M>F Increased BMI Peak age around 11 -13 y. o. Walks with a limp Limited internal rotation, flexion • May walk with the foot pointed outward • Knee, Thigh, or Hip pain!
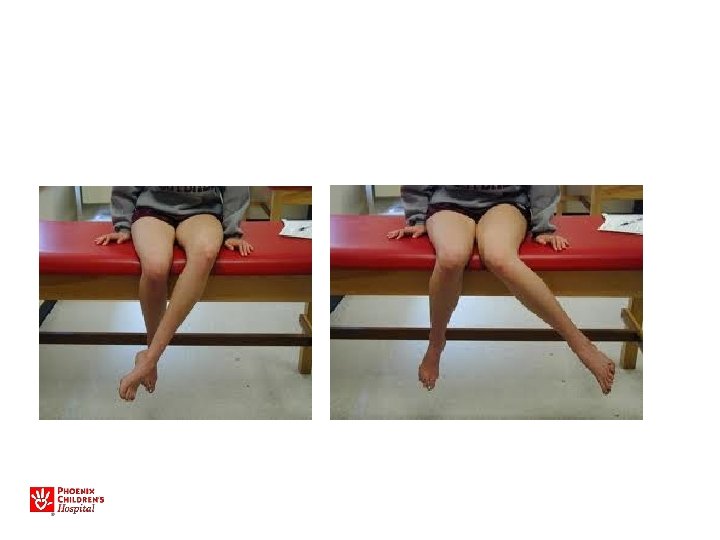
Examine the Hip!
Internal Rotation of Hip
External Rotation of Hip
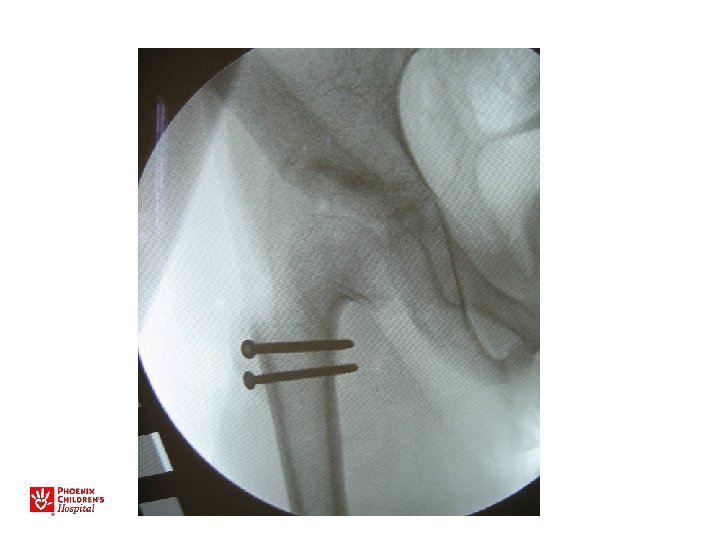
• Obtain AP and frog leg oblique x-rays • If a SCFE, make the child nonweightbearing • Send patient to ER immediately, admit to hospital for surgical fixation
12 yo F with right knee pain 3 week wait for a clinic appointment with an orthopaedist
Fell in gym class while kicking a ball Brought to ED by ambulance
Unstable SCFE • • • (5% of slips) Unable to bear weight or mobilize “Hip fracture” May have antecedent pain Minimal trauma High rate of osteonecrosis (20 -50%)
11 yo M, acute unstable SCFE
Avascular Necrosis of the Hip
Acute, Unstable SCFE • Capsulotomy to decompress – Either anterior open approach – Capsular decompression • Open reduction – Surgical hip dislocation
SCFE: Key Points Any child with knee pain • Examine hip range of motion – Prone and supine • Check AP and frog lateral hip films, particularly if limited hip motion • Any SCFE is an urgent referral – go to ER, see orthopaedist, admit to hospital for bedrest, surgical condition
Objectives • Review etiology of childhood hip deformity • Common Disorders – Slipped Capital Femoral Epiphysis – Legg-Calve-Perthes – Hip Dysplasia
Legg-Calve-Perthes • AVN in childhood, usually 4 -8 yo • Broad spectrum of deformities and outcomes • Incidence 11/100, 000
• Most younger children do well • >8 at onset more likely to have problems, need surgery
• Some children have minimal effects • More severe cases of Perthes can lead to severe, intractable hip deformity
DDX- Septic arthritis of the hip
Septic Arthritis • +/- Osteomyelitis
Septic arthritis – Delayed Diagnosis
Septic arthritis of the hip • Ultrasonography
(+) Septic arthritis of the hip • (+) Fever (+) Irritable joint Elevated CRP and ESR Effusion on U/S • ASPIRATE ! – (nucleated cell count typically > 50, 000/mm 3) – I and D
DD: Transient (Toxic) Synovitis • • Diagnosis of exclusion Much more common (1: 300 children) Clinical presentation like septic joint BUT…. Less fever Near normal labs Joint aspirate unremarkable Usually walking Child appears healthy
Transient (Toxic) Synovitis • Treatment Anti-inflammatories Activity restriction Typically resolves over 7 -10 days If doesn’t resolve in 2 - 3 weeks, consider more imaging/work-up
Objectives • Review etiology of childhood hip deformity • Common Disorders – Slipped Capital Femoral Epiphysis – Legg-Calve-Perthes – Hip Dysplasia
Developmental Dysplasia of the Hip (DDH) • Old term: CDH (congenital) • Spectrum of abnormalities from shallow hip to dislocation • Poor formation of hip joint • May lead to clinical or subclinical instability
Risk Factors • 10/1000 live births – 1/1000 dislocated at birth • Female (7: 1) • Breech position – Female, breech, firstborn – Nearly 10% risk! • Ethnic (Native American) • Family history • Oligohydramnios – Torticollis, metatarsus adductus
Effects • Hip with DDH may become normal, have residual instability, subluxate, or dislocate • Instability/subluxation leads to abnormal wear • Untreated, will lead to adult hip DJD in 25 -50%, accounts for about 20% of hip replacements
• Significant cause of early arthritis 39
Spectrum of condition Normal Acetabular Dysplasia Subluxated/ Unstable Dislocated
Diagnosis • Primarily physical exam • Ultrasound • X-ray – After 4 months • MRI/CT (usually only pre or post op)
Physical Exam • Barlow – “dislocatable hip” – Femur gently adducted and flexed, posterior force applied – Feel for palpable give or clunk as head leaves socket
• Ortolani – “click of entry” – Femur gently abducted, trochanter elevated – Feel for palpable clunk as head falls into socket
Other signs • Galeazzi sign – Femur appears short with hip flexed • Asymmetric abduction/motion of hip • Remember, irreducible hip is Barlow/Ortolani negative
Asymmetric skin folds • Skin folds in groin or buttock, not thigh Concerning Normal
Ultrasound • Used for evaluation/treatment exam -positive hips • May also be used for very high-risk patients (breech, family hx) • Not for general screening in US – Leads to overdiagnosis/treatment • Dynamic study most useful • Do after 2 -3 weeks of age
US • • • Sens 88. 5% Specificity 96. 7% PPV 61% NPV 99. 4% Operator Dependant! » BMJ 2005 47
Referral Newborn hip exam Normal Click / High suspicion Markedly Abnormal Static/Dynamic US after 2 -3 weeks of age Refer to Ortho
Treatment • Pavlik Harness – Complications with incorrect positioning (rare) • Too much flexion - femoral nerve palsy • Too much abduction - poss AVN 49
Treatment • Pediatrics 12/09 – Some cases of mild dysplasia resolve – May be no detriment in observing for 6 wks – Does NOT apply to unstable hips 50 50
Non-Operative • Childrens Abduction Brace – Stiffer, more restrictive – Used in older children or as fallback to Pavlik 51 51
Operative Treatments • • • 52 Closed Reduction Open Reduction Spica Casting Pelvic Osteotomy Femoral Osteotomy
Advanced surgical procedures • Bernese Periacetabular Osteotomy – Ability to rotate and correct hip socket
• Early diagnosis and appropriate treatment can minimize operative treatments 54 54
DDH CASES 55
8 day old female infant • • 56 Mother’s first child Breech, C-section Otherwise healthy R hip dislocated, can be reduced with Ortolani
57
• Pavlik Harness treatment for 8 weeks 58
59
9 day old female infant • Mother’s first child • Breech • R hip dislocated, can be reduced with Ortolani • Decreased abduction, positive Galeazzi 60
61
• Pavlik Harness 62
63
• Abduction brace 64
65
66
• Arthrogram • Closed reduction • Cast 67
68
69
70
13 yo with hip pain, limp • Family has noted increased pain with activity, not able to walk long distances • No infantile treatment or history • Patient has features of Charcot-Marie. Tooth (associated with hip dysplasia)
• Bilateral periacetabular osteotomies • Bilateral femoral osteotomies
Recommended Reading • Guille JT, Pizzutillo PD, Mac. Ewen GD. Development dysplasia of the hip from birth to six months. J Am Acad Orthop Surg. 2000 Jul-Aug; 8(4): 232 -42. – Comprehensive orthopaedic review • Shipman S, Helfand M, Nygren P, Bougatsos Screening for Developmental Dysplasia of the Hip US Prev Services Task Force 2006 – Reviews available literature, but conclusions are “incomplete” • Mahan S, Katz J, Kim Y. To screen or not to screen? A decision analysis of the utility of screening for DDH. JBJS 2009 91: 1705 -19 75
Thank you!