TITLE Complications of Diabetes in the Feet Vascular
 2)")
TITLE Complications of Diabetes in the Feet Vascular Tutorial (SET 1 and XXX) 2) INSERT 9 July DATE 2020

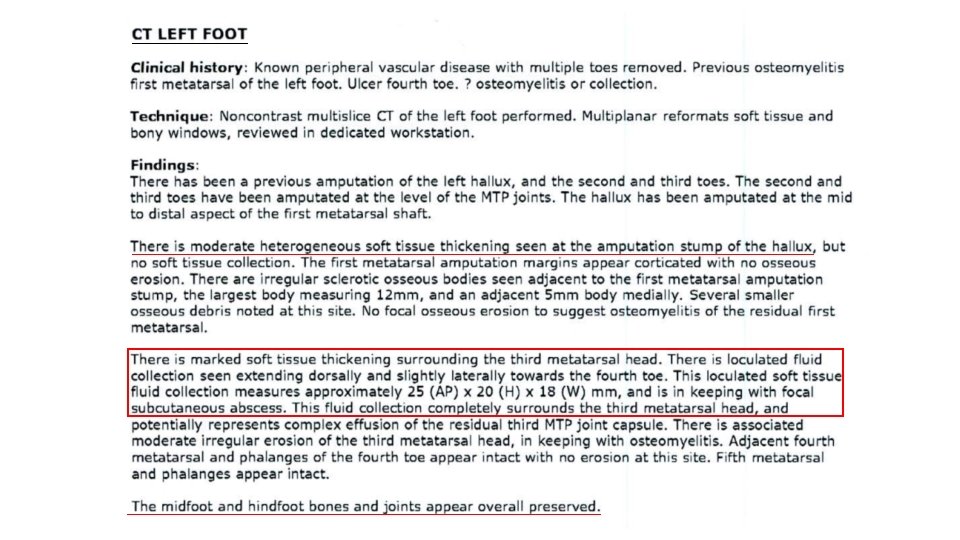
Clinical Scenario 1 • You review a 68 yo diabetic man in the outpatient clinic. He has a discharging sinus overlying his previously amputated third metatarsal head for the past two weeks. At that time (2 years prior), he has also had his 1 st and 2 nd toes amputated. • Your fellow registrar saw him in the emergency department over the weekend and prescribed oral cephalexin and arranged an external CT scan. You can’t access the CT images but the report and his plain X-ray are attached (OM of 3 rd MTP and collection). • He was reviewed in the vascular clinic 2 months ago and had a normal arterial duplex at that stage, with prior SFA stents patent.

imaging
 1. discuss the pathophysiology contributing to diabetes related foot disease and")
learning objective (s) 1. discuss the pathophysiology contributing to diabetes related foot disease and how this can differ from peripheral artery disease. 2. discuss the importance of foot architecture in diabetic foot disease and its relevance in this setting 3. consider reasons for the delayed presentation of his symptoms after his original surgery and potential preventative measures that may have helped

diabetes-related foot disease – globally • the leading cause of diabetes-related hospitalisations & amputations • mortality rates comparable to many cancers (annual mortality ~11% USA) • major amputation in 5 -8% of DFU patients within 1 -yr of ulceration • major amputation 5 -yr adjusted mortality ~45% (Rutherford) • a major burden on an individual’s quality of life with significant risks to their morbidity and mortality, and increases their healthcare costs
 • ulceration, ulceration infection, infection ischaemia or neuro-arthropathy of")
diabetes-related foot disease – definition(s) • ulceration, ulceration infection, infection ischaemia or neuro-arthropathy of the foot in neuro-arthropathy people with diabetes people at-risk of diabetes-related foot disease are – • those with diabetes who have developed peripheral neuropathy, peripheral arterial disease or have a history of previous foot disease

diabetes-related foot disease – locally
 1. discuss the pathophysiology contributing to diabetes related foot disease and")
learning objective (s) 1. discuss the pathophysiology contributing to diabetes related foot disease and how this can differ from peripheral artery disease
 multi-factorial ulceration: ulceration • cumulative result of")
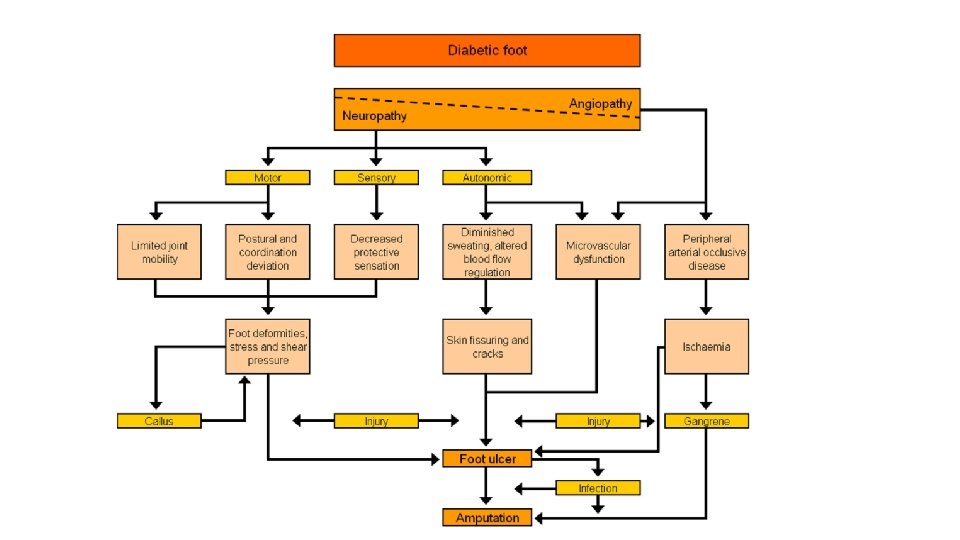
the natural history – complex & (usually) multi-factorial ulceration: ulceration • cumulative result of repetitive trauma causing ‘breach in continuity of skin, epithelium … caused by sloughing of inflamed, necrotic tissue’ (Robbins Pathology) TRIAD of – 1. neuropathy 2. foot deformity 3. trauma altered biomechanics causing shear / vertical stress through plantar aspect(s) of foot @ sites of 1) increased pressure, 2) foot deformity & 3) reduced joint mobility

neuropathy • ~50% DM patients • neurodegenerative process preferentially targeting: sensory → autonomic → motor axons • precise mechanism(s) remain debated

pathogenesis • ↑ glucose + • ↑ lipids + • ↑insulin signalling = DNA damage ER stress mitochondrial dysfunction neurodegeneration loss of neurotrophic signalling • macrophage activation & cell death • • •

neuropathy … • ‘length-dependant neuropathy’ / ‘stocking distribution’ • loss of distal epidermal axons → progressing proximally • polyneuropathy BUT is NOT a primary demyelinating neuropathy • retraction & ‘dying back’ of terminal (peripheral) axons (with preservation of cell body) • ALL regions of nerve involved

autonomic neuropathy • autonomic nerves regulate skin temp. & sweating • ↓ sweating & altered blood flow regulation • impaired autonomic (sudomotor) control = dry scaling skin & ↓oil gland function = ↑ skin cracking, fissure formation & ulceration • microvascular / veno-arterial reflex dysfunction & AV shunts (venous pooling) • ? pre-capillary sphincter dysfunction Sakai & Hosoyamada, JPhysio. Sci, 2013 1. local sympathetic axonal reflex 2. arteriolar-myogenic reflex 3. (minor) central sympathetic efferent response Hassan & Tooke Clin Sci (Lond) (1988) & Rathbun et al. , Vascular Medicine (2008)

microvascular dysfunction • many studies show NO change in blood flow associated with development of diabetic neuropathy • remains plausible pathological mechanism Kim et al. , Endocr. Metab. Immune Disord. Drug Targets 12 (2012). • poor neural microcirculation • thickened basement membranes • ↑ endo-neural capillary density (suggesting ischaemia) & • ↓ mediators of vasculargenesis (e. g. VEGF)

neuropathy … • sensory neuropathy • motor neuropathy

foot architecture & deformity

foot architecture – • structural deformity secondary to muscle degen. • longest motor nerves activate the intrinsic muscles of the foot (lumbricals)

foot architecture – ‘hammer toe’ prominent IPJ: prone to callus formation prominent plantar metatarsal heads: • ext of MTPJ = visible & palpable bony plantar prominences @ base of each toe. • First @ toes 1 & 5 then 2 -4 as neuropathy progresses → callus formation • normal = the lumbricals extend the IPJ & flex MTPJ • neuropathy = opposing muscles cause flex IPJ & extend MTPJ • sub-MT head fat pads migrate distally as a result of hyperextension of the MTPJ

• distal migration • normal • obliteration

foot architecture – ‘hammer toe’ + intrinsic minus • hammer toe + • upward rotation of the forefoot • hyper ext. of MTPJ. • weak extension of the hallux longus (great toe): hallux limitus • normally toe extension & flexion are balanced • lumbircal weakness = extension from the rest position is weak as the toe is already fully extended • cock-up deformity of the hallux longus with prominent extensor tendon: • impaired flexion at rest can cause the distal end of this toe to be visibly higher than the other toes. • high arch: relates to tightening of the plantar fascia causing a bowstring flexion the bones of the longitudinal arch

foot architecture – ‘charcot’ • pathogenesis – incompletely understood • neuropathy / abnormal protective motor reflexes & development of abnormal loading forces within the foot (+/- osteopenia) damage bone, joints & ligaments • subluxation +/- dislocation of MT / tarso-metatarsal / tarsal joints & odema from leaked synovial fluid & inflammation • bone perfusion increased ? due to abnormal sympathetic control (which may contribute to the osteopenia) • osteo-sclerotic change & fracture = tarsal collapse & outward bowing of the arch (‘rocker-bottom foot’ deformity), further adding to the abnormal loading and ulcer risk

foot architecture – ‘charcot’ • often precipitated by minor trauma, & may progress rapidly over weeks or a months • Stage 0 = unstable, warm, red and swollen foot • the point at which treatment should be initiated for maximum benefit • Stage 1 = ‘fragmentation’ with periarticular fractures, joint dislocation(s), instability & deformity • Stage 2 = ‘coalescence’ = reabsorption of bone debris • Stage 3 = stability = deformed foot

angiopathy • peripheral arterial disease 20 -60% of pts with diabetes • poor BSL management accelerates PAD; • ~1% ↑ HBA 1 c = 25 -28% relative risk of PAD • diabetes ↑ prevalence of symptomatic PAD (3. 5 x men & 8. 6 x women) • >50% DFU is neuro-ischaemic & ~90% in DFU requiring neuro-ischaemic major amputation • impaired O 2 delivery to meet metabolic demand • diabetes PAD commonly multi-segmental, typically infrapopliteal & poorly co-lateralised

 1. discuss the pathophysiology contributing to diabetes related foot disease and")
learning objective (s) 1. discuss the pathophysiology contributing to diabetes related foot disease and how this can differ from peripheral artery disease
 2. discuss the importance of foot architecture in diabetic foot disease")
learning objective (s) 2. discuss the importance of foot architecture in diabetic foot disease and its relevance in this setting

 3. consider reasons for the delayed presentation of his symptoms after")
learning objective (s) 3. consider reasons for the delayed presentation of his symptoms after his original surgery and potential preventative measures that may have helped

multifactorial & multi-disciplinary treatment of diabetic foot disease • perfusion: SFA stent & PAD surveillance / vascular follow up • infection: loss of protective sensation & DM management • pain: loss of protective sensation • metabolic control: worsening BSL / HBA 1 c / endocrinology • offloading: altered architecture after initial amputation (podiatry) • wound management: podiatry / pressure care / self-examination • correction foot deformity: prosthetics & orthotics / podiatry • medical optimisation: co-morbidity management • health education & behaviour:
 1. discuss the pathophysiology contributing to diabetes related foot disease and")
learning objective (s) 1. discuss the pathophysiology contributing to diabetes related foot disease and how this can differ from peripheral artery disease. 2. discuss the importance of foot architecture in diabetic foot disease and its relevance in this setting 3. consider reasons for the delayed presentation of his symptoms after his original surgery and potential preventative measures that may have helped
- Slides: 33