Case scenario3 Palmoplantar psoriasis with nail involvement History



































 – Eight features –")






- Slides: 44
Case scenario-3 Palmoplantar psoriasis with nail involvement
History of presenting illness § 35 year old male § Clerk by profession § Scaly lesions on palms and soles – 5 years § Exacerbation of lesions with fissuring and pain – Difficulty in walking and working in office – 15 days
Examination § Well defined scaly plaques – Both palms and soles § Nails – Pitting of all nails – Oil spot 3
Scaly plaques on palms 4
Scaly plaques on soles 5
Nail changes 6
Investigations Skin biopsy: Features of psoriasis LFT: Normal Blood counts: Normal 7 RFT: Normal
How different is palmoplantar psoriasis as a variant of psoriasis? § Affects approx 5% of all psoriasis patients § Second most common form of psoriasis § Disabling and difficult-to-treat variant § Epidemiology is poorly defined § Age of onset is later § More common in: – manual laborers, drivers, farmers, housewives
What is its effect on Quality of life? § Even with less BSA involvement – more likely to suffer from significant impact on Qo. L – significantly more likely to report problems • with mobility, self-care, and usual daily activities – level of functional impairment more § So considered independent criterion of severity – discordance b/w BSA involvement & QOL impact – even justifying the use of biologic therapies
What are the common manifestations? § With or without psoriasis elsewhere on body § Clinical forms: – well-demarcated, erythematous, scaly plaques – thick, scaly, hyperkeratotic plaques – painful fissures – pustules – nail involvement
Extensive fissuring
Fissures on soles
Nails
Pustular lesions
What are the triggers? § Trauma § Smoking § Irritants § Genetics: same as psoriasis vulgaris Smoking Genetics: same as psoriasis vulgaris Irritants
Differential diagnosis § Chronic eczema § Tinea manum/pedis § Pityriasis rubra pilaris § Cutaneous T cell lymphoma § Acquired keratoderma – Greater risk of misdiagnosis when nails affected
Hand eczema 17
Tinea pedis 18
PRP
Skin biopsy in palmoplantar psoriasis § ONLY When clinically difficult to differentiate from hyperkeratotic hand eczema – Except for vertically oriented multiple foci of parakeratosis, alternating with orthokeratosis, • no other histological feature considered significant enough § Some soft pointers – multiple foci of parakeratosis – focal loss of granular layer – presence of neutrophils at the summits of parakeratosis – thinning of supra-papillary plate – presence of tortuous and dilated capillaries in the papillary dermis
What are the treatment options? § First line: Topicals § Severe functional impairment, failure of topicals: – Phototherapy – Systemic therapy – Biologics
How to decide on which therapy? § Physical and emotional effects § Benefits and side effects of each therapy § Disease type § Topical treatment: results often disappointing – poor penetration through thick stratum corneum
What are the topical therapies available? § Topical corticosteroids – potent to super-potent, for up to 6 -8 weeks § Keratolytics: Salicylic acid, Urea § Calcipotriol § Tazarotene § Coal tar § Anthralin § Emollients
Factors which increase efficacy of topicals? § Occlusion § Combination of topical corticosteroids with: – Salicylic acid – Calcipotriol – Tazarotene – Phototherapy, Systemics and Biologics § Salicylic acid should not be combined with – Calcipotriene or UVB
Role of phototherapy? § PUVA: Topical and oral are very effective – Results comparable with systemic treatments – Fewer side effects § Nb. B-VB not as effective § Can be combined with topical steroids, systemic retinoids or methotrexate § 308 -nm excimer laser – healthy surrounding tissue is spared – more effective than NB-UVB
Which systemics can be used? § Acitretin & Methotrexate – Drugs of first choice § Acitretin – Under-utilized drug in this scenario. Well worth trying. – Give 8 -12 weeks before assessing success. Escalate to 35 mg/day after 8 weeks, if response inadequate – Combine with phototherapy for potentiating response § Cyclosporine: Second line – Caveat: Cannot be combined with phototherapy
When to think of Biologics? § Degree of functional impairment § Patients failed to respond to 4 weeks – potent/ superpotent topical corticosteroids or systemic therapies § Increased Modified PPP area and severity index (m-PPPASI) § > 10% of total surface of palms and soles affected § DLQI > 10
Efficacy of systemic therapies Drug Standard doses Efficacy Acitretin 25 mg/day 53% PUVA Oral Methoxsalen 30 mg alt day 53% Methotrexate 15 mg/day 47% Cyclosporine 200 mg/day 30% Engin B et al. Palmoplantar psoriasis. Clinics in Dermatology 2017; 35: 19 -21 28
Biologics in PPP Etanercept, Infliximab & Adalimumab Used with Success. • Etanercept • Infliximab • Adalimumab 29 SECUKINUMAB , Apremilast Positive Results • Secukinumab • Apremilast Ustekinumab Found good in recent research • Ustekinumab
SECUKINUMAB in Moderate to Severe Psoriasis Secukinumab shows significant efficacy in palmoplantar psoriasis
SECUKINUMAB in Moderate to Severe Psoriasis
Treatment of patient in question § Tab Methotrexate 15 mg/week § Tab Folic acid 1 mg X 5/7 days § Topical Calcipotriol with Betamethasone cream in the morning § Topical Urea ointment at night § Good response after 8 weeks
Nail psoriasis § 10 -78%: concurrent nail psoriasis in palmoplantar psoriatics* § Isolated nail involvement: 5 -10% § 10% more common in males § More frequently associated with: – Scalp psoriasis – Genital psoriasis – Psoriatic arthritis. (70 -80% of psoriatic arthritis patients have nail psoriasis) § Significant physical and psychological handicap § Indicator of severe disease (joints) *Dogra A, Arora AK. Nail psoriasis: The journey so far. Indian J Dermatol 2014; 59: 319 -33
DIP jt involvement: Nail association
Common manifestations of nail psoriasis Common manifestations § Pitting: commonest of nail psoriasis – length of pit • suggestive of duration – deeper pit • suggestive of involvement of intermediate and ventral matrix – may be arranged in transverse or longitudinal rows or disorganized
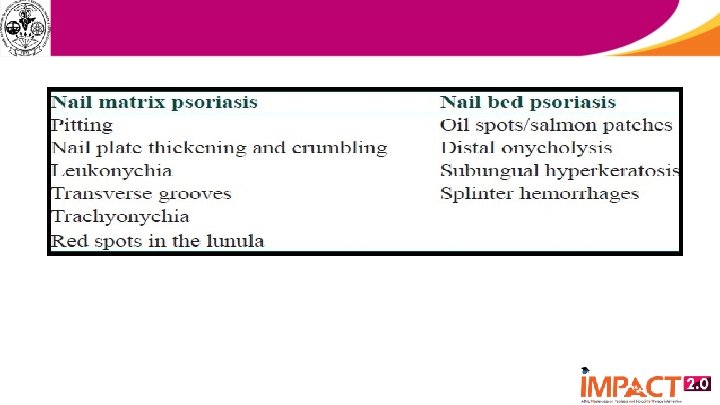
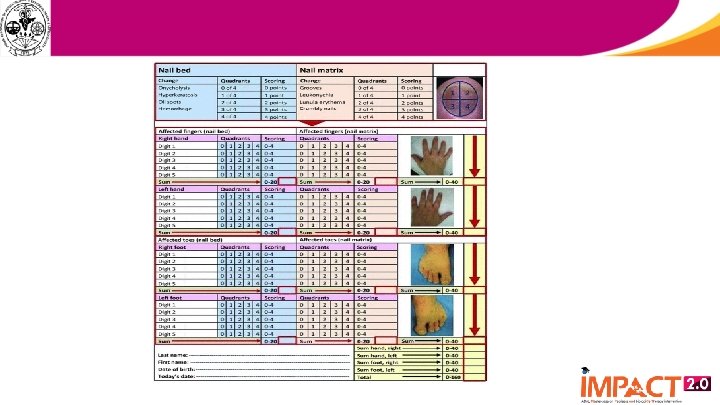
How to evaluate severity? § Nail Psoriasis Severity Index (NAPSI) – Eight features – Four involve the nail matrix • pitting, leukonychia, red spots: lunula, nail plate crumbling – Four of the nail bed • onycholysis, splinter hemorrhages, subungual hyperkeratosis, oil spot 37
Treatment- General measures § Nails should be kept short – avoids exacerbating onycholysis – avoids accumulation of exogenous material under nail § Avoid trauma to nails – prevents onycholysis and entry of pathogens § Protection against irritants § Avoid aggressive manicure of the cuticle – may provoke paronychia § Cosmetic camouflage not advisable 39
Treatment options available Topical therapy § Nail matrix involvement – Intralesional steroids – Tazarotene – Topical potent steroids § Nail bed involvement – Calcipotriol and topical steroids – Tazarotene – Cyclosporine 40
Other options § Clobetasol lacquer § Iontophoresis – Dexamethasone § Intralesional – Methotrexate – Cyclosporine § Laser: PDL*, Fractional CO 2 followed by tazarotene/potent steroids *- Limited nail involvement
Many nails involved § PUVA § Acitretin – Low doses § Methotrexate § Cyclosporine § Biologics – Infliximab – Etanercept – Secukinumab
What is the role of biologics? § Conventional treatment for nail psoriasis – unsatisfactory, tedious and inconvenient § Most of the treatment options – achieve only a moderate efficacy – complete clearance is infrequent § Efficacy of conventional therapy – decreases with time § Role of biologics – efficacy in both the skin and nail components
Thank you 44