Psoriasis By AFSAR FATHIMA Dept of Pharmacology Psoriasis

Psoriasis By AFSAR FATHIMA Dept. of Pharmacology


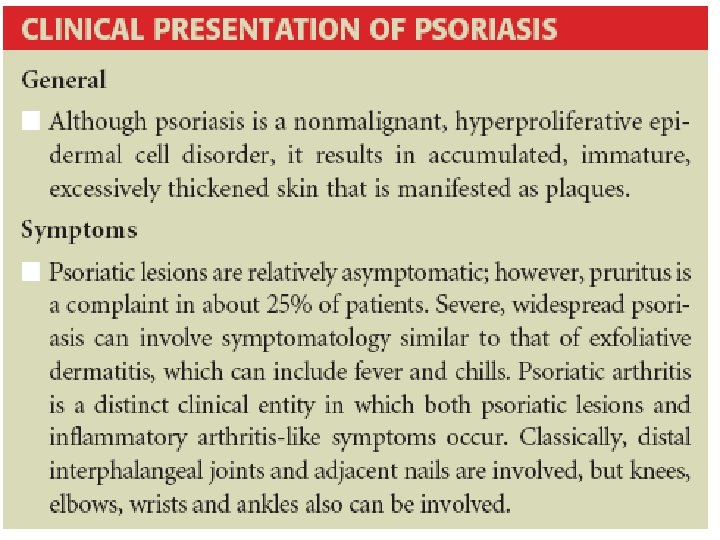
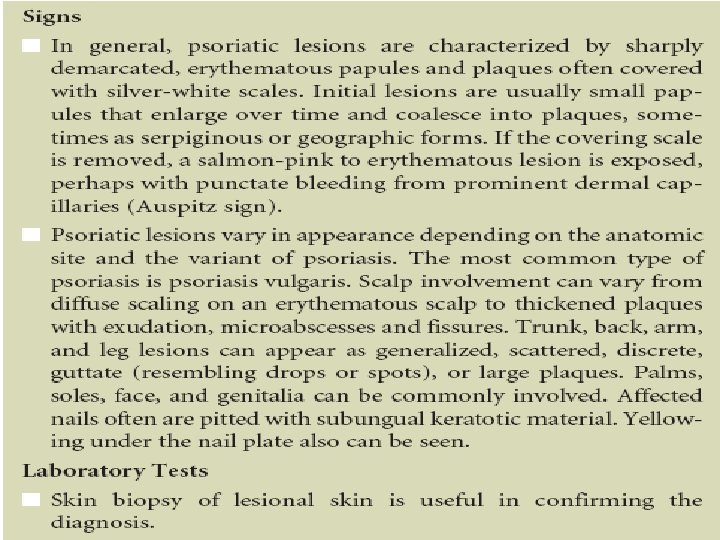
Psoriasis • A non-infectious, chronic inflammatory disease of the skin, characterized by well-defined erythematous plaques with silvery scale, with a predilection for the extensor surfaces and scalp, and a chronic fluctuating course.

• A complex and multi-factorial disease associated with interaction between environmental factors (exogenous or endogenous antigens) • A specific genetic background

Etiology v Climate, stress, alcohol, smoking, infection, trauma, drugs. v Skin injury (rubbing, venipuncture, bites, mechanical pressure induce Psoriatic lesions v Lithium carbonate, β-adrenergic blocking agents, some antimalarial agents, NSAIDS, tetracycline's exacerbate psoriasis and

Pathophysiology • Immunologic mechanisms: – Cutaneous inflammatory T-cell–mediated immune activation requires two T-cell signals that are mediated via • cell–cell interactions by surface proteins • antigen-presenting cells (APCs) – Once T cells are activated, they migrate from lymph nodes and the circulation into skin – In psoriatic lesions, T cells migrate into the epidermis – Once in the skin, activated T cells secrete various cytokines that induce the pathologic changes of psoriasis

• Defects in epidermal cell cycle: As a result of pathogenic T-cell production and activation, psoriatic epidermal cells proliferate at a rate sevenfold faster than normal epidermal cells - The germinative cell population increases in psoriatic skin - Duration of the epidermal cell cycle is nearly eight times faster than normal skin

Treatment • Goals: – directed at skin normalization – reduction or clearing of erythema, papules, and plaques, as well as scales – to achieve resolution of lesions • Assessment of extent – The psoriasis area and severity index (PASI) • Mild: PASI score 12 • Moderate: PASI Score 12 to 18 • Severe: PASI Score >18

Treatment • General Approach – Keratolytic: Salicylates – Non-pharmacologic • Emollients • Balneotherapy – Pharmacologic • Topical • Systemic – Phototherapy: Sunlight, UVB, PUVA

Keratolytic – Used to remove scale, smooth the skin, and decrease hyperkeratosis. Salicylic acid Mechanism of action: Disruption in corneocyte-to-corneocyte cohesion in the abnormal horny layer of psoriatic skin. The keratolytic effect of salicylic acid enhances penetration and efficacy of some other topical agents such as corticosteroids

Adverse Events: salicylism, with symptoms of nausea, vomiting, tinnitus, and hyperventilation. Fatal cases of percutaneous salicylate intoxication have been reported in children and adults. Administration as a gel or lotion, is usually applied two to three times a day in concentrations of 2% to 10%

Non Pharmacologic Treatment • Emollients: used during therapy-free periods to minimize skin dryness that can lead to early recurrence • These agents hydrate stratum corneum and minimize cutaneous transepidermal water loss • Hydration causes the stratum corneum to swell and flattens the surface contour • Effective as moisturizers decrease binding forces within the horny layer, enhance desquamation, and eliminate scaling • Increase pliability of the skin, have antipruritic activity, and possess mild vasoconstrictor activity

Adverse Effects: Folliculitis and allergic or irritant contact dermatitis lotions, creams, or ointments, often need to be applied several times per day (about four times per day) Balneotherapy: Saltwater bath Bath at Dead Sea with UV B exposure (by virtue of it being below sea level). • The Kangal hot spring in Turkey • The Blue Lagoon in Iceland

Pharmacologic Treatment • Mild to Moderate Psoriasis – Topical Treatment Eg: corticosteroids, vitamin D analogues, tazarotene • Moderate to Severe Psoriasis – Systemic Treatment Eg: biologic agents, cyclosporine, acitretin

Corticosteroids Class I corticosteroids: very high-potency – include products such as clobetasol propionate, halobetasol propionate, and betamethasone dipropionate (optimized vehicle) – Used primarily as alternatives to systemic adrenocorticoid therapy when local therapy is feasible – They should be used for finite periods of time (as short as possible) and on relatively small body surface areas

• Class VII corticosteroids are agents with the lowest level of vaso constricting potency. They have a weak anti-inflammatory effect • Hydrocortisone 1%, safest for long-term application. safest products for use on the face and intertriginous areas.

• Intermediate classes: include products with a mediumpotency ranking, used in moderate inflammatory dermatoses. • can be used on the face and intertriginous areas for limited periods of time

Vitamin D analogs • inhibits keratinocyte differentiation and proliferation • provide antiinflammatory benefits – Tazarotene • a synthetic retinoid, Like other topical retinoids, it modulates keratinocyte proliferation and differentiation • Effective for the treatment of mild to moderate plaque psoriasis • adverse effects are mild to moderate pruritus, burning, stinging, or erythema. These local reactions have been shown to be dose- and frequency-related • Tazarotene is available as a 0. 05 or 0. 1% gel and cream, and is applied once a day, usually in the evening. • Tazarotene is often used in combination with topical corticosteroids to decrease the incidence of local adverse events and to increase efficacy

Topical Therapy: Second Line agents – Coal Tar • Down regulates epidermal prolifereation • Coal tar, when applied to normal skin, stimulates transient epidermal hyperplasia followed by a cytostatic effect with epidermal thinning • Coal tar preparations of 2% to 5% tar are available in lotions, creams, shampoos, ointments, gels, and solutions • Coal tar treatment is a burdensome, time-consuming treatment

Adverse events: local irritation, unpleasant odor, staining of skin and clothing, and increased sensitivity to UV light, including the sun.

Antralin: Topical anthralin, particularly with UV light, is long established as an effective approach to the treatment of psoriasis Anthralin possesses antiproliferative activity on human keratinocytes, inhibiting DNA synthesis

Calcinurin hinhibitors: Pimecrolimus and tacrolimus capable of exerting a local immunomodulating effect • normalize hyper proliferation of epidermis

Systemic Therapy: First Line Agents Biologic Therapy: • TNF inhibitors – Infliximab – Etanercept – Adalimumab • T-Cell Activation inhibitors – Alefacept – Efalizuman

Systemic Therapy : Second Line – Acitretin – Cyclosporine – Tacrolimus – Methotrexate – Sulfasalazine – 6 -thioguanine – Hydroxy urea – Tazarotene

Combination, Rotation, sequential therapy • Acitretin + UVB light • Acitretin + PUVA (UVA combined with psoralen, usually methoxsalen) • Methotrexate + UVB light • PUVA + UVB light • Methotrexate + cyclosporine

TH K N A U O Y
- Slides: 28